
Abstract
Background
The utility of Cardiopulmonary Exercise Testing (CPET) to identify higher risk surgical patients remains controversial. There is limited research investigating the value of preoperative CPET to plan perioperative pathways for patients undergoing major pancreatic surgery.
Methods
Retrospective cohort study, comprising two groups before and after a change in referral policy for High Risk preoperative anaesthetic clinic with CPET. Period 1 discretionary referral and Period 2: universal referral. The primary aim was to investigate the impact of this policy change on critical care use (planned vs unplanned) on the day of surgery and on delayed critical care admission. Secondary end points included a comparison of the total number of critical care bed days, days in hospital, complication rates and mortality data between the two cohorts.
Results
177 patients were included; 114 in Period 1 and 63 in Period 2. There was a reduction in unplanned day of surgery postoperative admissions to critical care (28.1% vs. 11.1%, p = 0.008). Seven (6.1%) of patients in Period 1 and 1 (1.6%) patient in Period 2 had delayed admission, though no p value was calculated due to the small numbers involved. Complication rates were similar in each group. The median critical care bed days was 1 (range 0–21) days in Period 1 and 1 (0–13) days in Period 2.
Conclusions
A universal referral policy for preoperative CPET demonstrated a decrease in unplanned day of surgery critical care admissions and a trend towards reducing delayed (>24 h postop) critical care admission which could be investigated in a larger study. No measurable impact was seen on clinical outcomes.
Background
Patients having major elective surgery may benefit from planned postoperative admission to a critical care unit. Advance planning eases the pressure on limited critical care resources. Preoperative Cardiopulmonary exercise testing (CPET) has been embraced by the perioperative medicine community, particularly in the United Kingdom, as a means to highlight patients at higher risk of deterioration after surgery, and hence more likely to benefit from planned critical care admission on the day of surgery, yet this can still be viewed as controversial. 1 CPET is a relatively resource heavy investigation and in a recent survey was only available in 53.8% of 197 acute UK hospital trusts. 2
A recent meta-analysis shows only modest or poor association between commonly measured CPET variables and perioperative outcomes, such as postoperative complications, length of hospital stay, and mortality. 3 The Measurement of Exercise Tolerance before Surgery (METS) study is the largest blinded observational study to date to evaluate the utility of preoperative CPET. METS suggests that the CPET variables Oxygen Consumption at Anaerobic Threshold (AT) and Oxygen Consumption at peak exercise (VO2 peak) are inferior to Dukes Activity Status Index (DASI) questionnaire score to predict major adverse cardiac events after surgery. 4
In common with METS, much of the CPET literature has focused on the mathematical association between selected variables such as AT and VO2 peak and perioperative endpoints. In the evaluation of preoperative CPET, a more fundamental question to address is whether the incorporation of pre-operative CPET into peri-operative planning is associated with a change in clinical outcomes or resource utilisation.
Plausible mechanisms whereby assessment by an anaesthetist at high risk preoperative clinic incorporating CPET may influence these endpoints for patients having major elective surgery are in:
patient selection for surgery, targeting of perioperative interventions towards patients with cardiopulmonary impairment or reduced functional capacity and stratification of patients into either a planned ward based or critical care based pathway on the day of surgery following postoperative recovery.
Critical care encompasses High Dependency (HDU): (levels 1 or 2) care, and Intensive (ITU) care: (level 3). The Intensive Care Society defines level 1 care as intensive monitoring for patients who are at ‘risk of their condition deteriorating… whose needs can be met on an acute ward’. Level 2 care is for those patients who require ‘more detailed observation… including support for a single failing organ system,’ most commonly vasopressor cardiovascular support; whilst level 3 care is ‘advanced respiratory support alone, or basic respiratory support with support of at least two organ systems’. 5
Unplanned day of surgery critical care admissions for elective surgery patients are undesirable as they put pressure on limited critical care resources and the wider hospital system. Patients who suffer delayed admission to critical care after deterioration on a general ward may have particularly poor outcomes, and often require Level 2 or Level 3 support, which may be resource intensive. 6 The report ‘NCEPOD Knowing the Risk’ identified that 65 of 787 patients were not discharged to “the most appropriate location” post surgery and found that this was associated with a mortality rate of 20% at 30 days. 6
A retrospective analysis of 314 colorectal resection patients demonstrated improved survival for those patients who had been referred at surgeons` discretion for preoperative anaesthetic consultation, including CPET. Planned postoperative critical care utilisation was 22% in the CPET group compared with 10% for those not referred. 7 A possible explanation was that CPET identified less aerobically fit patients to be prioritised for planned day of surgery critical care admission postoperatively and that this improves recovery from surgery and led to fewer delayed admissions from the surgical ward to critical care for ‘rescue’ after complications. However direct evidence is limited.
This study investigates the impact of anaesthetic clinic consultation, including preoperative CPET, on perioperative planning and short-term outcomes after major elective pancreatic resections.
Methods
This retrospective analysis of data was approved by Research Ethics Committee East Midlands (Ref. 17/EM/0370) and the United Kingdom Health Research Authority in September 2017. Requirement for patient consent was waived.
Our large acute University hospital Trust is the regional referral centre for Hepatobiliary surgery. The high-risk preoperative clinic is delivered by a team of consultant anaesthetists. A CPET service was added to the clinic in 2006, with tests initially run by six of the consultants. Referral to this service for patients requiring major pancreatic surgery was initiated by the surgical team (discretionary referral). An audit of local practice demonstrated that only 89 of 495 (18%) of pancreatic surgery patients were referred by surgeons.
From December 2013, a policy step change to universal referral was introduced. All patients scheduled for elective pancreatic resection were referred to High Risk preop clinic, including CPET, unless subjective assessment implied exceedingly good exercise tolerance. The assessing anaesthetic consultant (one of six) would make a planning recommendation for a surgical ward (level 1) or critical care based pathway on the day of surgery, based on their judgement of comorbidities and functional capacity, and utilising objective information from the CPET.
Study aims
The primary aim of this study was to investigate the impact of this policy change on planned vs unplanned critical care use, including delayed admission to critical care for the two study Periods. The study was conducted after the universal referral policy (Period 2) had been in place for a year, in order to decide whether to continue the service.
Secondary end points included the proportion of patients who underwent CPET before and after the policy change, the level of care given in critical care, the complication rates, a comparison of the number of critical care bed days, the hospital length of stay (LOS), mortality and the number of days at home within the first 30 days postoperatively. 8
Patient selection
A before and after cohort study conducted retrospectively on a clinical registry maintained prospectively by the hepatobiliary surgical (HPB) team. Inclusion criteria: all patients who had undergone elective major pancreatic surgery in a tertiary referral centre (University Hospitals Plymouth NHS Trust) between January 2012 and December 2014. Emergency cases were excluded.
The three-year period was divided into two study intervals; Period 1: a pre-policy change interval (discretionary CPET) from 1 January 2012 to 30 November 2013 and Period 2: a post policy change interval (universal CPET) from 1 December 2013 to 31 December 2014.
Data collection
The clinical registry holds information on patient demographics, co-morbidities, date of surgery as well as both operation and morbidity outcomes. This was cross-referenced with hospital clinical informatics systems to confirm inclusion of all relevant elective pancreatic surgery cases between the reference dates, to obtain hospital length of stay (LOS) and gain mortality data. Manual cross-referencing (iSoft Clinical Manager) of each case was carried out to confirm whether preoperative anaesthetic clinical consultation had occurred, and on what dates. For those patients who had attended an anaesthetic pre-assessment clinic, outpatient letters were reviewed to obtain details of co-morbidities and planned post-surgical care pathway (i.e. critical care or level one-ward based). Co-morbidity data of those who did not attend the anaesthetic pre-assessment clinic were obtained from the surgical outpatient letters. The critical care electronic patient record system (Innovian version 7.1, Draeger, Germany, 2014) was cross-referenced to gain information on critical care unit length of stay, relevant complications (including readmission), level of organ support required and the reason for admission.
Where registry records were unclear, a manual search of surgical outpatient letters and patient notes was conducted and reviewed for information on recovery and complications encountered within 30 days of surgery.
Statistical analysis
This was effectively a “before and after” service evaluation, with enhanced capture and analysis of clinical outcomes, so no formal power calculation was conducted. Statistical review was undertaken using IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp. Pearson’s chi-square test was used to analyse categorical variables. Continuous variables were compared with non parametric tests (Mann Whitney) and a p-value of <0.05 was considered significant.
Results
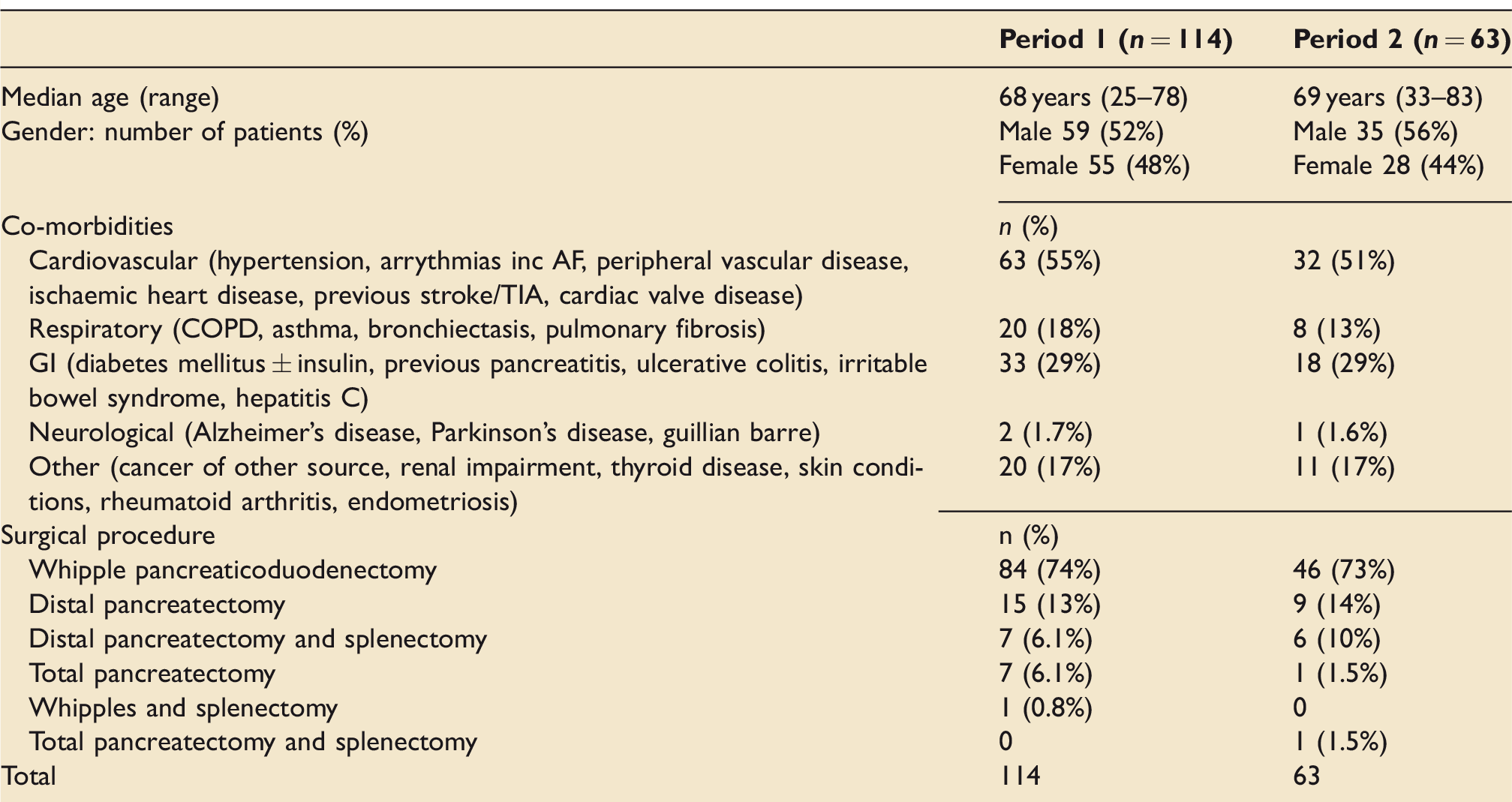
There were a total of 177 patients across the two groups; 114 in Period 1 and 63 in Period 2. The majority of patients underwent a Whipple pancreaticoduodenecotmy (See Table 1).
During period 1, 29.8% (34/114) of patients underwent CPET. In period 2, 88.9% (56/63) of patients had a CPET (p < 0.0001). The seven patients who did not undergo CPET testing during period 2 (universal CPET) were characterised as subjectively aerobically fit on the basis of a history of regular strenuous physical exertions without symptoms.
Critical care bed use on the day of surgery (either planned or unplanned) for Period 1 was 55.2% (63/114) and 57.1% (36/63) in Period 2. There was a decrease in unplanned admissions from 28.1% in Period 1 to 11.1% in Period 2 (see Figure 1) (p = 0.008).
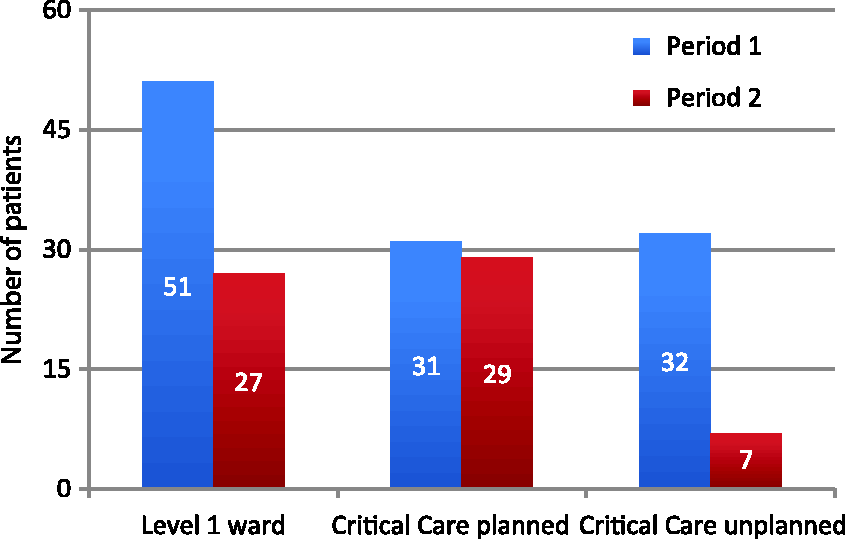
Patient’s day of surgery destination, Critical Care admission divided into planned and unplanned. p = 0.008.
The proportion of patients in each period who were admitted for delayed critical care more than 24 h after their operation was 6.1% (7/114) in Period 1 and 1.6% (1/63) in Period 2. This is a marked reduction, but since only one patient was admitted in Period 2, statistical advice is that it is not appropriate to calculate a Chi-square p value.
In Period 1, 40% (25/63) of the patients admitted to critical care on the day of surgery received Level 1 care (monitoring) only, and 60% (38/63) received organ support; 30 patients received level 2 care and the remainder received level 3 care (See Figure 2). Of delayed critical care admissions (i.e. >24 h following surgery) from the ward, six had undergone a Whipple pancreaticoduodenectomy and one a laparoscopic distal pancreatectomy with splenectomy. All received organ support; three needed level 2 care, i.e., vasopressor support and four had level 3 care: intubation and positive pressure ventilation for respiratory failure (1) and for management after laparotomy for anastomotic leak (3).
In Period 2, 43% (15/35) of the patients admitted to critical care on the day of surgery required Level 1 care (monitoring) only and 57% (20/35) of patients received organ support: 15 of these patients received level 2 care and 5 received level 3 care. The single patient in Period 2 who underwent delayed admission (i.e. >24 h postop) to critical care was a readmission who had been on a planned day of surgery critical care pathway after a Whipplès procedure involving a technically difficult pancreatico-gastic anastomosis due to a necrotic tail of pancreas. This patient subsequently developed an anastomotic leak and sepsis and was admitted to ITU for prolonged vasopressor (level 2) support.
For the patients experiencing delayed (>24-h postop) admission from the ward, the mean LOS in critical care for the seven patients in Period 1 was 5.7 days (median 3.00, range 1–15 days) and hospital LOS 21.7 days (median 21, range 11–43 days). The single readmitted patient in Period 2 had a critical care LOS of seven days and a hospital LOS of 92 days (See Figure 3).
We used the Clavien–Dindo classification categorise complications within 30 days of surgery (See Table 2). 9 A score of ‘0’ means that the patient did not have a complication. An increase in score reflects an increase in the severity of the complication. Major complications score 3–5. Superficial or deep wound infection, leak (bile/pancreatic), bleeding and lower respiratory tract infection accounted for the majority of the complications.
Patient demographics.
Complication rates, mortality data, critical care LOS, hospital LOS and number of days at home for each period.
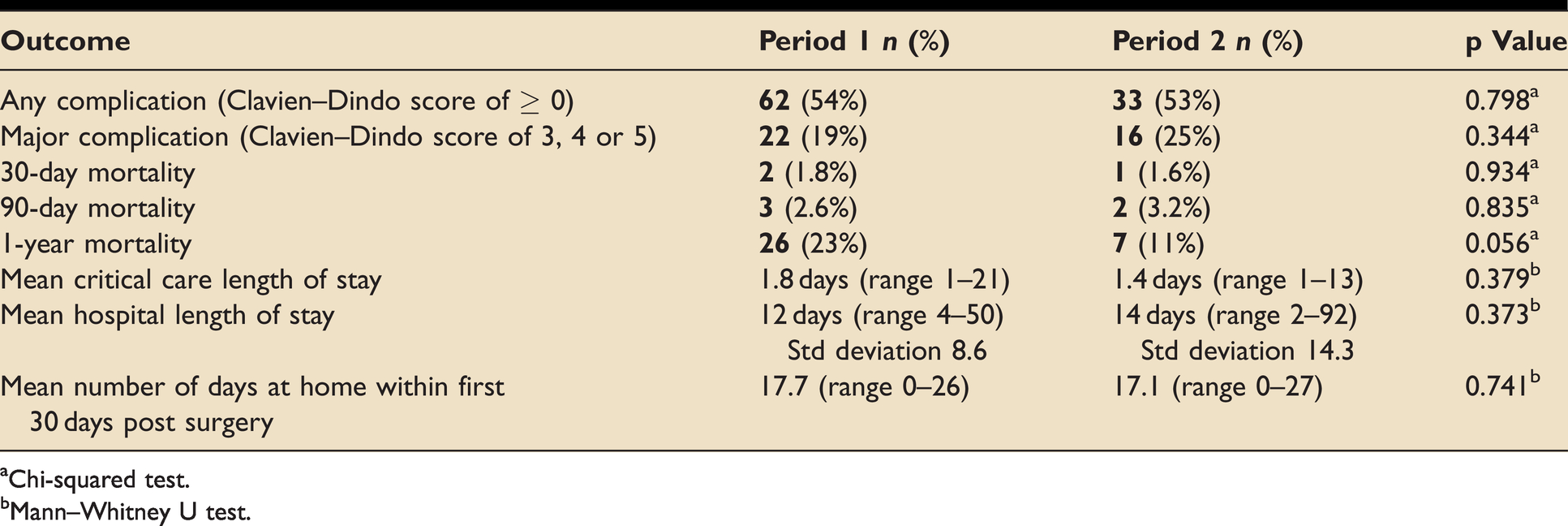
aChi-squared test.
bMann–Whitney U test.
Discussion
The primary aim of this study was to examine the effects of universal preoperative anaesthetic consultation including Cardiopulmonary Exercise Test on the use of critical care beds (a surrogate marker for resource utilisation) in patients undergoing major elective pancreatic surgery. This small study has demonstrated that such a policy can reduce unplanned critical care admissions on the day of surgery, and may reduce delayed (>24 h postoperative) admissions to critical care for rescue from complications. However we did not demonstrate a change in length of stay in critical care or in hospital, nor any difference in clinical outcomes.
Much of the CPET literature has focused on mathematical associations between selected variables such as AT and VO2 peak and postoperative endpoints.3,4,10–12 In some of these studies, admission to critical care (planned or delayed) has been used as an independent variable to adjust regression analyses.10,13 However, there is limited evidence to address the more fundamental question of whether prospective incorporation of a preoperative high-risk anaesthetic clinic including CPET into a peri-operative pathway impacts resource utilisation or clinical outcomes. In two studies investigating the impact of discretionary CPET for major elective colorectal resections, clinical endpoints in those who attended preoperative anaesthetic clinic were either in line with, or better than in those who were not referred, despite being older and having more co-morbidities. In both studies there was an increase in planned day of surgery critical care admission, which may have partially accounted for the observed results.7,14
A further study stratified elective colorectal surgical patients into different care pathways based on a 30-day postoperative mortality prediction score, incorporating CPET variables and other factors determined in a preoperative clinic. Those with predicted mortality <1% were stratified to postoperative surgical ward and those with predicted mortality >4% allocated to day of surgery HDU care. If predicted 30-day mortality was 1–3% (“intermediate” risk) then patients were allocated to either HDU or planned ward care on the day of surgery, depending on HDU availability and a consensus decision of the attending clinical team. Amongst this intermediate risk group, those with planned postoperative critical care had a substantially lower rate of complications. 15
It is a fundamental assumption of perioperative planning that HDU admission is unequivocally beneficial for this group of patients but the evidence to support this premise is tenuous. Best practice recommendations in settings such as emergency laparotomy and major elective surgery include risk scoring with early planned use of critical care for patients at high risk for adverse outcomes.16,17 Many patients die in hospital of complications after surgery without ever being referred to critical care, but it appears that the “best” hospitals are better at rescuing patients from complications.18–20 There is a fairly consistent signal from observational studies that delayed critical care admission is associated with worse outcomes.6,10,13 Evidence for an “ICU effect”, that is, a benefit for planned day of surgery admission for elective surgical patients is less convincing, though this is partially attributable to the methodological challenges of conducting trials in which critical care admission is allocated at random.10,21
Our study has many limitations. The cohort of patients in the two periods is broadly comparable in terms of baseline characteristics and co-morbidity burden, yet retrospective observational studies conducted in small cohorts such as ours are vulnerable to confounding. A prospective randomised study design could mitigate against this, though it is hard to imagine a randomised trial of such a highly complex intervention as a preoperative clinic: the dearth of these studies in the literature are testimony to this. Process factors that can affect length of stay in critical care or hospital such as bed occupancy rates, discharge planning and social care requirements, were not reported. There are likely to have been many unquantified patient related factors, such as cancer staging and histological type, and differences in the quality of surgical and perioperative care which also affected outcomes. For example there appears to be a trend towards better mortality at one year associated with period two, however since ours is a small study, prone to statistical alpha error, it is unlikely that this effect is real. Conversely it is likely that our study, in common with that of Carlisle et al conducted in 314 elective colorectal patients, is underpowered to investigate the effect of a “high risk” CPET clinic on delayed critical care admissions. 10
Second, our analysis is limited to short and medium-term outcomes in patients having major elective surgery for pancreatic cancer in the NHS, and may not be transferable to other settings.
Thirdly, the two periods were consecutive: it is likely that overall perioperative care improved with advances in time, and there is a 2% year-on-year relative reduction in mortality in the general population which probably also translates to the surgical population, but we have not adjusted for these factors. 22
Fourth, our preassessment team comprised of a heterogeneous group of many consultant anaesthestists interpreting the CPET reports during the study periods. Results are thus prone to inter-observer variation, however the study design reflects the impact of a ‘real life’ high-risk perioperative clinic setup on perioperative outcomes.
Fifth, it is an undeniable limitation that our study focuses on data that is now seven years old, susceptible to recall bias. It is also likely that in the intervening period our local practice in terms of interpretation of preoperative CPET and the manner in which this influences perioperative care has evolved has involved in line with clinician experience and international guidance. 1 However, since the literature in this area remains thin, we believe that there is a value in reporting our experience.
Finally, preoperative high risk clinic with CPET may influence case selection. From the limited information available we cannot be certain that the threshold for selection of patients for major resection was the same in the two periods. It is possible that the decision to operate may have been either more liberal or more restrictive in the second cohort, partially driven by anaesthetic consultation, and that this also influenced short and longer-term outcomes. To illustrate this point with the extreme case: if a high risk clinic recommends that no patients proceed to surgery, then the peri-operative complication rate will become zero, but this does not mean that perioperative care has improved!
Does our study have any implications for clinical practice?
We believe so. Uncertainty pervades clinical practice - if high-risk periop clinic with CPET provides special spectacles through which to predict likelihood of requirement for higher levels of monitoring and support, then so much the better. Comparing requirement for a higher than anticipated level of care before and after our step change in policy for referral by the surgical team for complex anaesthetic assessment, it appears that the major advantage of a “universal” policy is to identify in advance a requirement for specific individuals to be on a planned postoperative critical care based pathway, rather than trying to catch up on the day of surgery. This has a deep intrinsic value for the system.
Conversely, a critical interpretation is that a policy of universal over discretionary referral to a high-risk clinic incorporating CPET, which is in itself resource heavy, results in increased planned day of surgery critical care, further increasing resource utilisation, yet with no meaningful patient benefit. Is reduction of unplanned day of surgery critical care admissions a meaningful outcome in itself? We believe so: unplanned alterations in perioperative care pathways may stretch anaesthetic and recovery nurse capacity, for example whilst patients have extended stays in recovery waiting for a critical care bed to become available. This can create additional systemic pressure and potentially contribute to critical incidents.
A hybrid view is that this study supports a PACU (post anaesthesia care unit) model whereby level 1 and 2 care as defined by the ICS are provided outside of a traditional critical care unit. 5 A high proportion of patients in both cohorts in this study were admitted to critical care for monitoring or vasopressor infusion only (Figure 2)-levels of support which can conceivably be safely and effectively delivered in an enhanced ward or recovery setting. 23
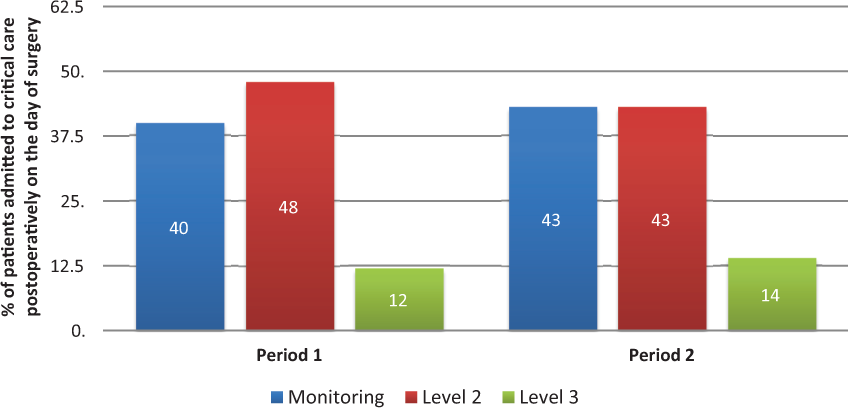
Level of support received after day of surgery Critical Care admission in each period.
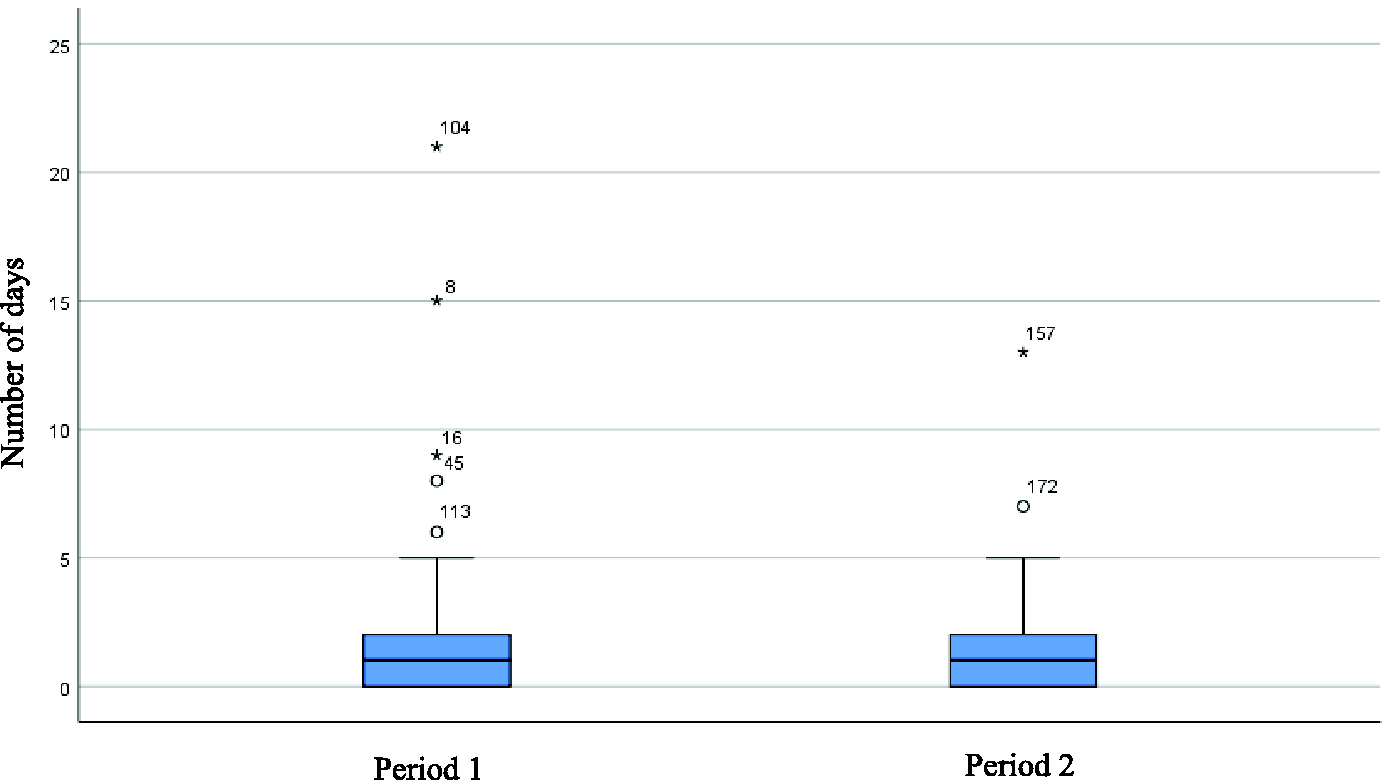
Box and Whisker plot. Number of days in critical care between Period 1 and Period 2. Median 1.0 days (range 1–21) Period 1 and 1.0 days (range 1–13) Period 2. Mann–Whitney p = 0.379.
A high-risk clinic incorporating CPET may have utility to risk stratify patients prospectively into planned perioperative care pathways: HDU, enhanced care unit and general surgical ward however this requires further research. It is also possible that other factors such as frailty have an influence on outcomes. To date these have not been well quantified in the perioperative literature.
In conclusion, this retrospective observational study conducted before and after a step change in preoperative assessment arrangements in a small cohort of patients having major elective pancreatic resection showed a decrease in unplanned critical care admission on the day of surgery. The study was underpowered to investigate the impact of this change on clinical outcomes.
Footnotes
Acknowledgements
Dr Mathew Jenkins who aided with the initial data collection. Mr Roy Powell at the Royal Devon and Exeter research and development department for statistical assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.