
Abstract
Number of subjects currently participating in high-endurance aerobic exercise training regimens and competitions has substantially increased in recent years. While there is no doubt that regular exercise practice is fundamental for the maintenance of a good health, there have been reports of cardiac structural changes of subjects exposed to strenuous endurance physical exercise. This article reports a case of a 47-year-old male very successful sportsman—including being a six-time Ultraman winner—who has accumulated more than 50,000 h of training and competition in his 35-year career, averaging 25–30 h/week. Despite this huge amount of aerobic exercise, about 25 times larger than typically recommended dose for health purposes (i.e. 75 min of vigorous exercise per week), no major abnormalities were detected in electrocardiograms (rest and maximal exercise), transthoracic echocardiogram, and magnetic resonance imaging. In fact, after this complete evaluation, his heart was found to be quite normal.
Keywords
It is well established that regular physical exercise is of paramount importance for a healthy lifestyle 1 in a clear dose–effect relationship between exercise volume and health benefits. A considerable increase in the number of people training and competing has been seen lately, particularly middle-aged individuals, both recreationally and professionally, especially in long-distance/duration mass sport events, most likely exceeding two million subjects in United States. 2 Sanchis-Gomar et al. 3 retrieved data from 834 European cyclists who had completed the Tour de France between 1930 and 1964 and found that they lived 8 years longer as compared with their native general population. In the same line of thinking, Pelliccia et al. 4 studied 114 Olympic athletes submitted to several years of intense long-term exercise and did not find adverse consequences to the heart. Nonetheless, there is still some concern about the risks of sudden death during the races (although absolute risk seems to be quite low and lower than 1/100,000 participations)2,5 and to a potential harm from “exercise exaggeration.”6,7 While this is one area far from consensus,8,9 there is some evidence suggesting that competing in marathons and/or longer events could lead to deleterious structural heart changes and a slightly higher risk of atrial fibrillation in later life.8–10 This article presents a very unique case report of a 47-year-old male athlete who has been highly successful in competing at international level for over 35 years in long- and very long–duration sport events. By carefully examining the structure and function of his heart, some structural and functional changes would be expected.
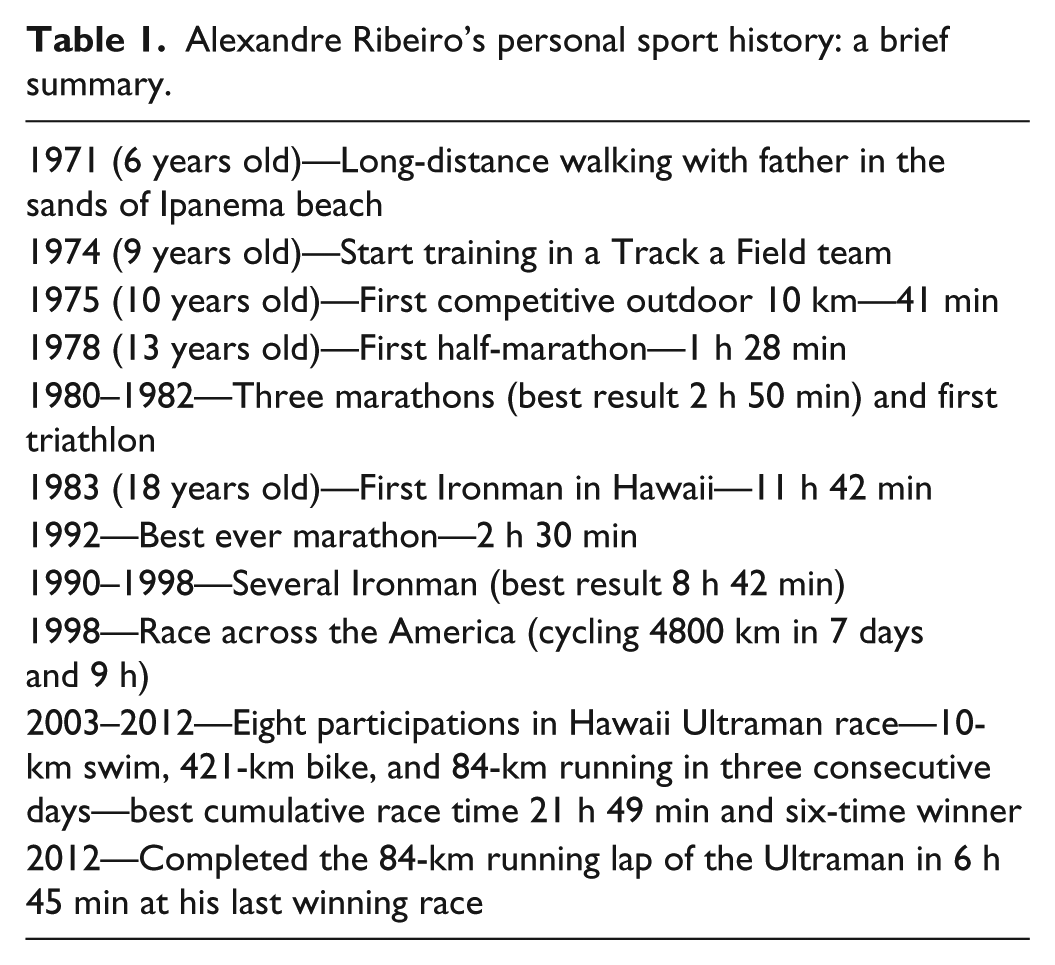
Just 2 weeks after an outstanding victory at 2012 edition of the Ultraman competition, Mr Ribeiro, a Brazilian athlete born in 1965, after reading and signing a consent form, volunteered to be submitted to clinical examination, resting and exercise electrocardiogram (ECG), transthoracic echocardiogram, cardiac magnetic resonance (CMR), and a maximal treadmill cardiopulmonary exercise testing (CPET). He has also agreed in sharing with us his amazing sport history as summarized in Table 1. His typical training schedule for the last three decades involves swimming, cycling, and running, divided in two or three daily sessions, amounting somewhere between 4 and 8 h/day, for an estimated training load between 250 and 400 METs-h/week. It is not uncommon running 50–70 km or pedaling for 5 or 6 h in a single training session. Interestingly, he does not regularly use global positioning system (GPS) or heart rate monitors and also denied use of protein or vitamin supplements. He has never had a major sport injury or lesion in his long career, and regular stretching exercises are not part of his routine.
Alexandre Ribeiro’s personal sport history: a brief summary.
Mr Ribeiro is a White man, aged 47 years when evaluated, 179.3 cm in height and 69.7 kg in body weight, proportionately distributed in a 2-5-3 ectomesomorph somatotype. He was asymptomatic for cardiorespiratory system with a normal physical exam and basic blood laboratory data and a resting blood pressure of 138/84 mm Hg. His resting ECG showed a very mild sinus bradycardia of 58 beats/min (bpm), voltage criteria for left ventricular hypertrophy, and high positive T-waves (see Figure 1). His cardiac vagal index as assessed by the 4-s exercise test 11 was 1.68 corresponding to the 75th–90th percentile range for his age group. During treadmill CPET using a ramp protocol, he got exhausted at the maximal speed of 20 km/h and 0% incline with a maximum heart rate of 197 bpm. Maximum VO2 (maximal oxygen consumption) was 66 mL/(kg.min) (about 175% of the age-predicted value) at a VE (expired ventilation) of 116 L/min. O2 pulse curve was completely normal with values progressively increasing toward the end of effort. Cardiorespiratory optimal point was 18.9, corresponding to almost 1 standard deviation below the age- and gender-predicted value, reflecting excellent interaction of both systems at submaximal exercise level. 12 The recovery heart rate measured at 1 min post-exercise was 166 or 31 bpm lower than maximum value while walking at 5 km/h. Exercise and post-exercise ECG were absolutely normal with no arrhythmias or J-point or ST-segment changes.

Resting electrocardiogram of a 47-year-old male sportsman—6-time Ultraman winner.
Imaging studies were performed with high-quality equipments handled by well-trained and experienced specialized physicians 2 weeks after his last Ultraman victory in 2013. Magnetic resonance study revealed normal resting biventricular volumes and systolic function—left ventricular indexed end-diastolic volume 97 mL/m2 (absolute value of 182 mL) and end-systolic volume 32 mL/m2 (absolute value of 60 mL) resulting in an ejection fraction of 67% and right ventricular indexed end-diastolic volume 88 mL/m2 (absolute value of 164 mL) and 66% ejection fraction, normal left ventricle indexed mass of 75 g/m2 (141 g) and maximum wall thickness of 0.9 cm in the septal wall. Left atrial volume was slightly increased to 36 mL·m2 (area of 28 mm2). No fibrosis was detected in the delayed enhancement images. The extracellular volume was measured at mid-septal wall using a parametric T1 map (Molli sequence) before and after injection of 0.2 mmoL/kg of gadolinium contrast, and the result was normal at 24.5%. Myocardial T2 times measured using a parametric T2 map sequence in all 16 myocardial segments were normal for this sequence and equipment, between 43 and 45 ms, indicating absence of myocardial edema. Resting transthoracic echocardiogram revealed normal mean two-dimensional (2D) global strain—19%—and just a minor increase in 2D strain at right ventricle free wall—mean 26% and apex 33%—with normal systolic and diastolic functions.
Despite some claims that high-volume training and/or marathon running could induce cardiac damage, 6 a more recent state-of-the-art paper 13 has indicated that atypical findings such as marked cardiac dilation, reduced deformation, or small patches of delayed gadolinium enhancement may be, in reality, commonly encountered in well-trained athletes and, at present, with unknown prognostic significance. Therefore, as also recently stated, 8 the competitive exercise does not induce cardiac damage in individuals with healthy hearts, but induces physiological functional and structural cardiac adaptations, with positive effects on life expectancy. As a matter of fact, as further characterized by the athlete reported here, to develop an athlete’s heart is by no means a prerequisite for a beneficial effect of training on health or to achieve top results in long-distance competitive events. 8
In summary, considering the unique athletic profile of this middle-aged man, encompassing a very successful career and an amazing total volume of training in the last 35 years of over 50,000 h of vigorous aerobic exercise—at least 25 times larger than an age-matched subject according to current health guidelines (75 min of vigorous exercise/week 14 ) and well-above the criteria of 4500 h for high-volume lifetime training 15 —it is worthwhile to find that this six-time Ultraman winner has quite a normal heart with no major findings suggestive of “athlete’s heart” adaptations, except by a mild left atrial enlargement. Therefore, this case report reinforces the concept that regular exercise, even when kept at high-intensity/volume for many years, should be regarded as a healthy practice. 8 Nevertheless, considering that some subjects present structural and functional heart changes, it is reasonable to point out a need for well-controlled and population-based long-term studies evaluating the natural history and prognostic significance of these high-volume training “adaptations.”
Footnotes
Acknowledgements
The authors thank Mr Ribeiro for providing detailed information about his sports training history.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was partially supported by research grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico CNPq/Brazil (304328/2011-1) and Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro—FAPERJ/Brazil (E-26/102.289/2013).