
Abstract
Background
Acute liver failure is a rare syndrome comprising a coagulopathy of liver origin, jaundice and encephalopathy in a patient with no prior history of liver disease. Paracetamol overdose is the leading cause of acute liver failure in the United Kingdom and often presents with extrahepatic organ dysfunction requiring critical care.
Presentation: We present the case of a patient with hyper acute liver failure secondary to paracetamol overdose.
Management and discussion: Management focused on ensuring the correct diagnosis had been made, administering N-acetyl cysteine, fluid resuscitation and broad spectrum antimicrobials. Early intubation and transfer to a transplant centre were undertaken following development of hepatic encephalopathy. Neuroprotective measures and hypertonic saline were instituted to reduce the risk of intracranial hypertension. High dose haemofiltration was also started to help reduce ammonia levels. Aggressive critical care therapies with specialised input results in good outcomes for patients admitted with paracetamol induced hyper acute liver failure. Liver transplant is reserved for those patients unlikely to survive with medical treatment alone.
Case presentation
Mrs S, a 30 year old female presented to the emergency department confused, nauseous and complaining of abdominal pain. Collateral history revealed she had last been seen 3 days ago and was suspected of ingesting up to 30 g of paracetamol at some point between then and her presentation. Her examination revealed right upper quadrant pain, a prolonged capillary refill time of >5 secs, dry mucous membranes and cool peripheries. She was confused and disorientated with a Glasgow coma score of 13 (E3 V4 M6). She had a pulse rate of 110 bpm, blood pressure of 85/40 mmHg, respiratory rate of 24 breaths per minute and oxygen saturations of 99% on room air. An arterial blood gas showed acidaemia and hyperlactataemia which prompted urgent CT scans of her head, abdomen and pelvis. Imaging showed a homogenous liver with patent portal vein, hepatic artery and hepatic veins and no evidence of infective abdominal pathology. Her CT head was normal. She was referred and admitted to critical care directly from the emergency department. The patient’s blood tests at presentation and on critical care admission are shown in Tables 1 and 2.
Blood results on presentation.
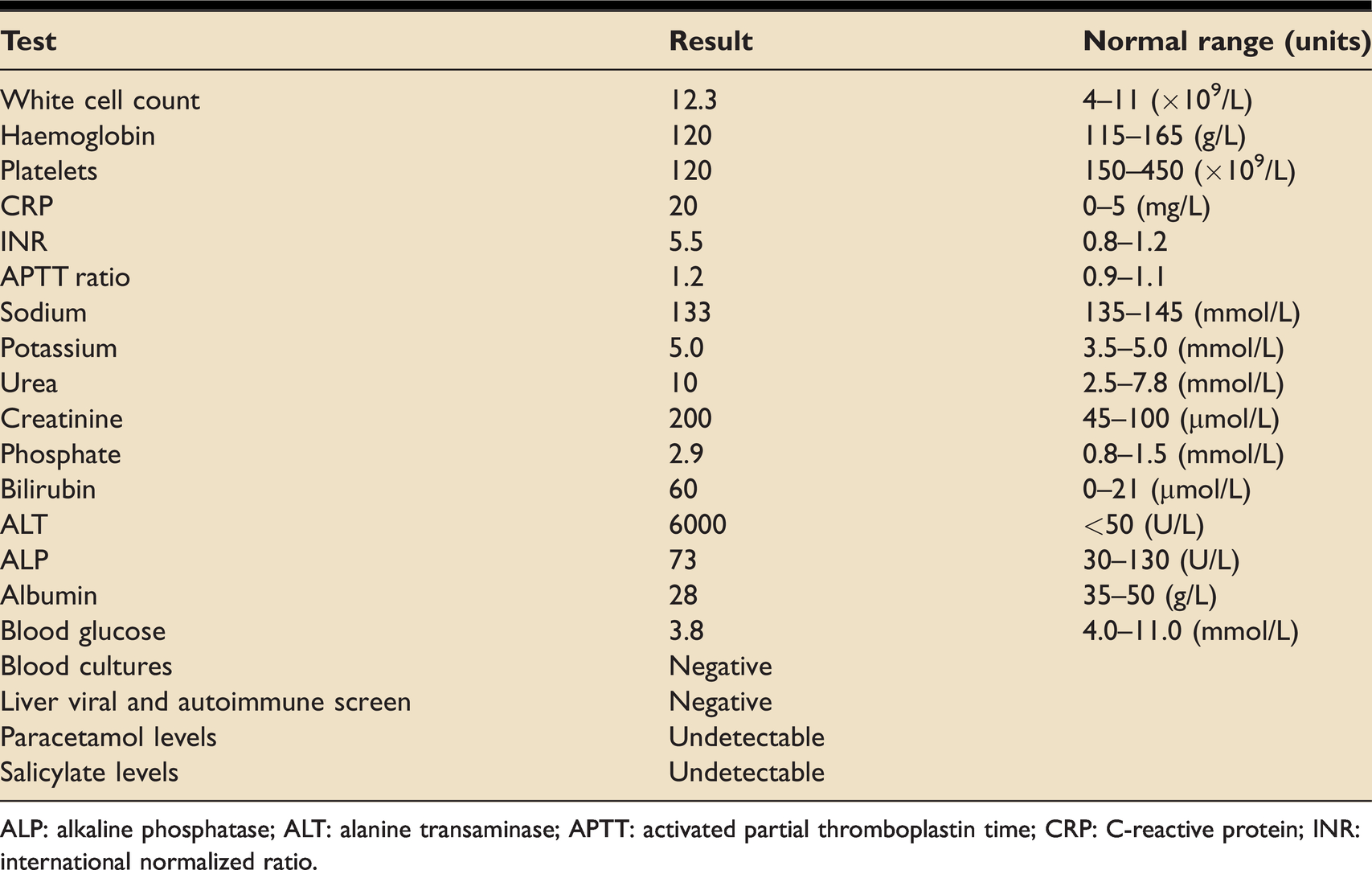
ALP: alkaline phosphatase; ALT: alanine transaminase; APTT: activated partial thromboplastin time; CRP: C-reactive protein; INR: international normalized ratio.
Blood results over first 72 h of admission.
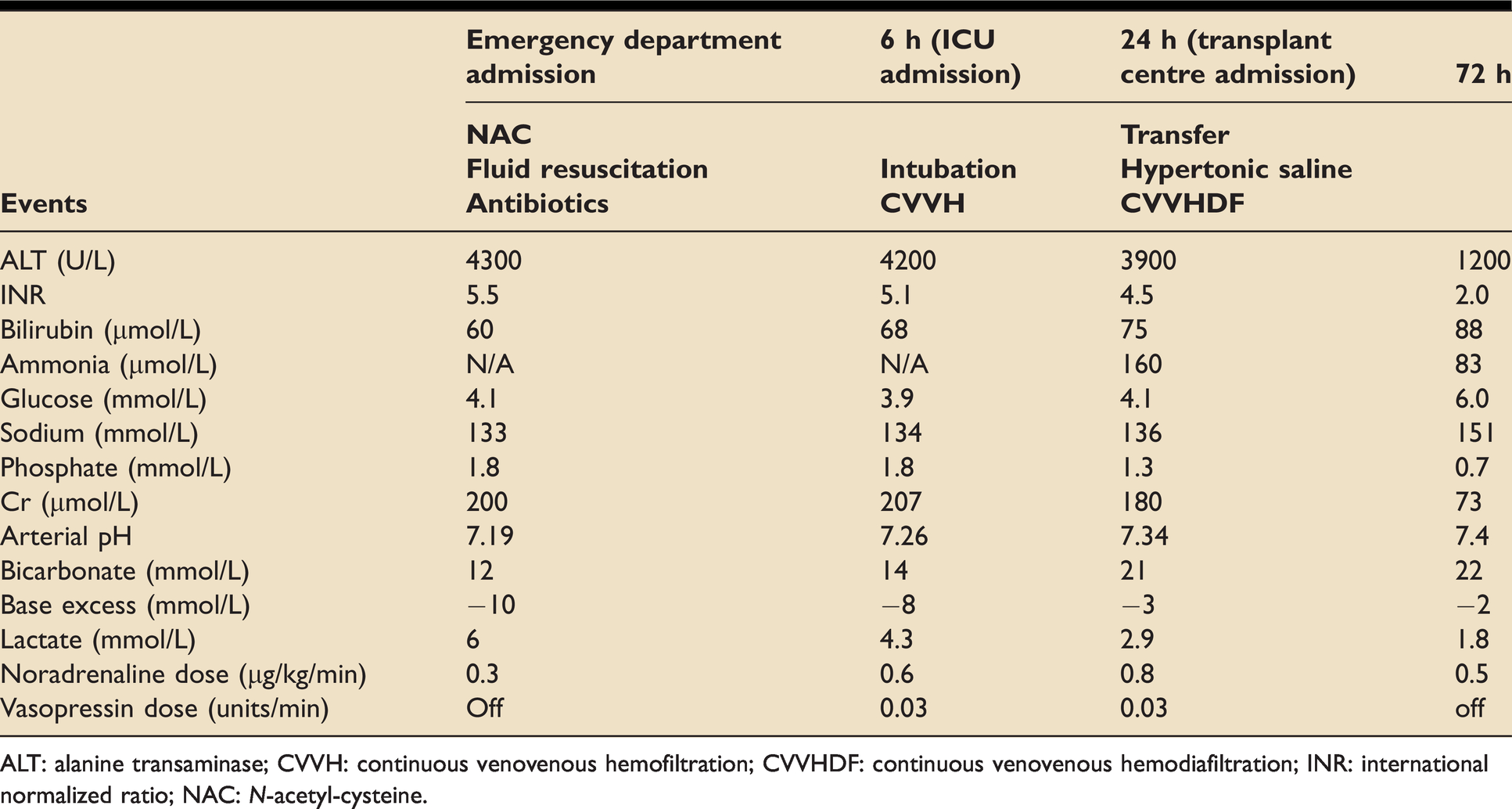
ALT: alanine transaminase; CVVH: continuous venovenous hemofiltration; CVVHDF: continuous venovenous hemodiafiltration; INR: international normalized ratio; NAC: N-acetyl-cysteine.
Management and treatment
Due to significant acute coagulopathy, jaundice and encephalopathy and in the context of the history, a diagnosis of hyper acute hepatic failure due to paracetamol overdose (POD) was made. N-acetyl-cysteine (NAC) and fluid resuscitation with 0.9% sodium chloride were initiated. In view of her hypotension, arterial and central venous lines were inserted to facilitate pressure monitoring and noradrenaline administration. A 20% glucose infusion to treat hypoglycaemia was commenced. Mrs S was intubated in critical care due to progressive hepatic encephalopathy (HE) causing confusion and agitation. After discussion with the regional transplant centre, broad spectrum antibiotics and antifungals were initiated. A dialysis catheter was inserted and haemofiltration was commenced. Mrs S was subsequently transferred to the liver transplant centre where renal replacement therapy in the form of continuous venovenous haemodiafiltration (CVVHDF) without anticoagulation was continued at a dose of 90 mls/kg/hr. Hypertonic saline was commenced with the aim of gradually increasing her sodium to 145–150 mmol/L. See Table 2 for blood results over the first 72 hours following presentation.
Having initiated the above treatment, the MDT team decided to observe Mrs S. She was managed medically and did not meet transplant criteria. Mrs S was nursed with full neuroprotective measures and did not demonstrate any clinical signs of raised intracranial pressure. Mrs S was kept sedated and ventilated until her serum ammonia level was consistently <100 umol/L. Her condition improved and she was eventually weaned from mechanical ventilation after 8 days and was discharged home from hospital 3 weeks after her admission. She required intensive rehabilitation input and although she has remained out of hospital, has a significantly reduced physical capacity.
Discussion
POD remains the commonest cause of acute liver failure (ALF) in the UK. ALF is a rare condition that occurs in patients without pre-existing chronic fibrotic liver disease. It occurs when a defined liver insult results in acute liver injury (coagulopathy: INR > 1.5, and jaundice) which progresses to HE. Coagulopathy, jaundice and impaired consciousness can also be seen in other conditions such as sepsis with disseminated intravascular coagulation. However, if there is no primary liver insult, these cases should be managed as secondary liver injury with the treatment being directed towards treating the underlying cause. Determining the presence of pre-existing fibrotic liver disease can often present a difficult clinical challenge. 1
Classification of acute liver failure
Various classifications and nomenclatures exist to describe the different presentations and patterns of ALF. The most commonly used classification in the UK is the O’Grady classification. 2 This divides patients into ‘hyper acute’, ‘acute’ or ‘subacute’ dependent upon the time interval between jaundice and the development of encephalopathy (Figure 1). Hyper acute liver failure refers to disease where encephalopathy develops within 7 days of jaundice and is commonly seen with POD. The transplant-free prognosis for medically managed hyper acute presentations is better than that of acute and subacute presentations. Acute and subacute presentations are less likely to survive without liver transplantation, which reflects the very different nature of the disease process underlying these syndromes. Recent data suggests that even in severe cases of POD-ALF, survival with good quality medical care approaches that of emergency liver transplantation. 3 This emphasises the fact that the aggressive application of critical care therapies can make a significant difference in this cohort of patients. The European Association for the Study of the Liver (EASL) have recently published evidence based guidelines on the management of acute liver failure. 1
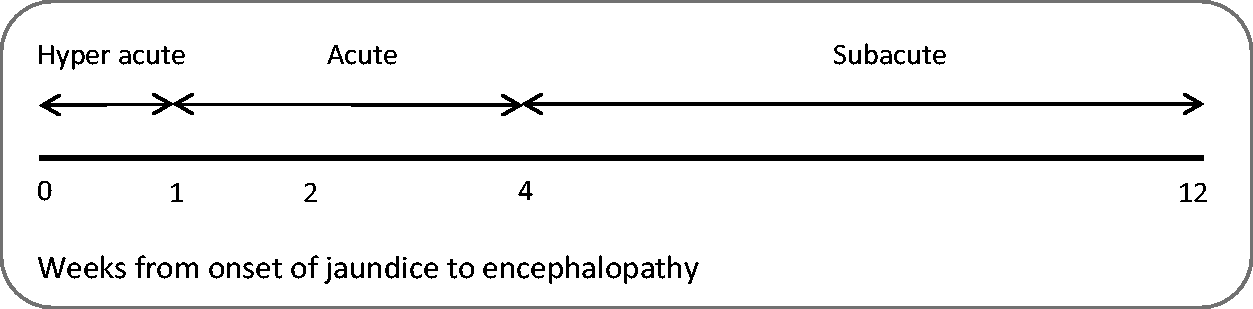
O’Grady Classification of Acute Liver Failure. 2
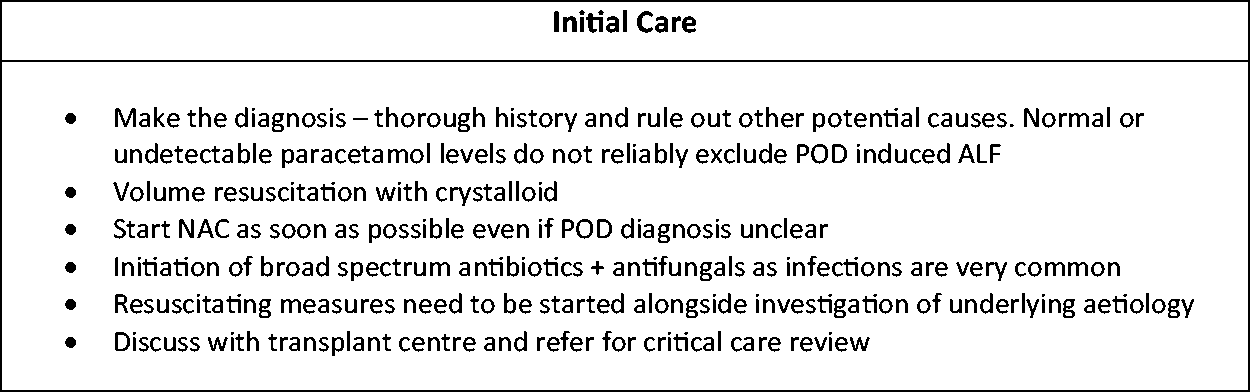
Summary of initial care.
Summary of neurological care.
Summary of cardiovascular management.
Summary of renal management.
Making the diagnosis and initial management
Paracetamol metabolism produces the hepatotoxic intermediate metabolite N-acetyl-para-benzo-quinone imine (NAPQI). Usually this is rapidly detoxified by a glutathione dependent pathway within the liver. However, in POD, glutathione stores become depleted and damaging NAPQI accumulates causing hepatonecrosis, liver dysfunction and hepatocyte enzyme release. Significant POD therefore commonly presents with aminotransferases that are in the thousands, a mildly elevated bilirubin and a significant coagulopathy. Neurological features can develop within just a few hours and progress rapidly to grade 3 or 4 HE (see Table 3). ALF is often accompanied by a significant metabolic acidosis, hyperlactataemia and hypovolaemia. Therefore, in addition to a full blood count and renal profile, liver function tests, a coagulation profile and an arterial blood gas must be done if ALF is suspected. Paracetamol levels are important as they may provide a clue to aetiology when history is unavailable. However, POD cannot be excluded on the basis of a low paracetamol level as a significant number of patients present late or have taken a staggered overdose. The history, if available, is often vital in making the diagnosis. Once ALF is strongly suspected, a liver disease screen including viral, autoimmune and toxicology should be undertaken to rule out other potential causes of ALF (see Table 4). Ultrasound imaging to assess the vascular inflow and outflow to the liver should also be performed, though CT scanning may be required in some cases as was presented here.
West Haven Hepatic Encephalopathy Criteria.

Initial investigations to help establish the cause of acute liver failure.
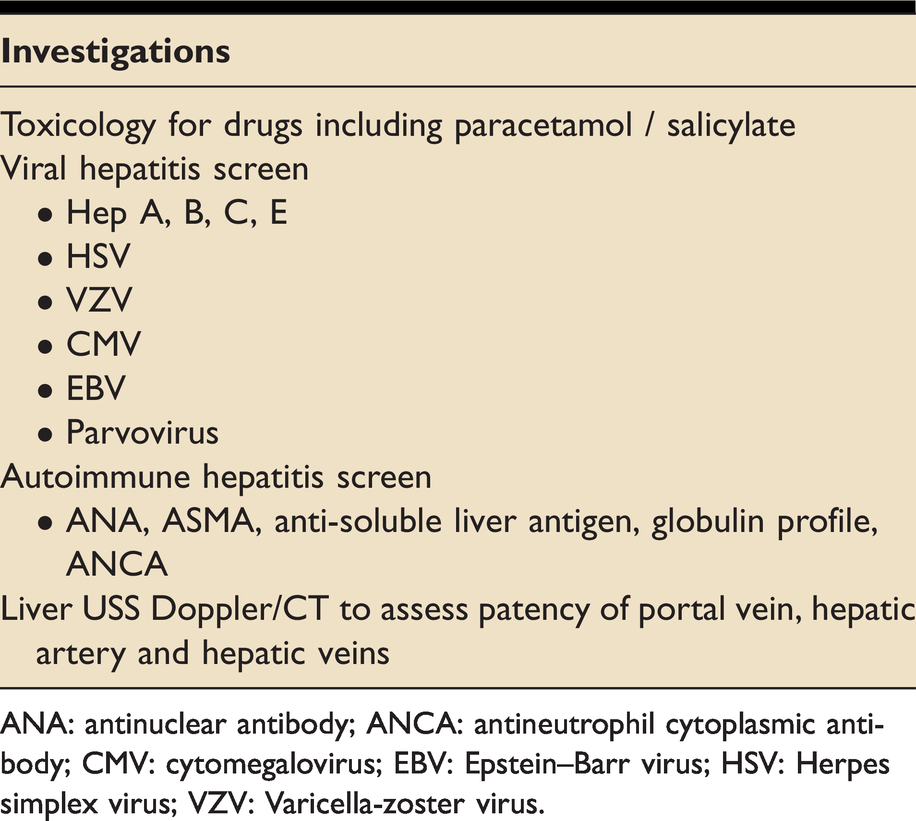
ANA: antinuclear antibody; ANCA: antineutrophil cytoplasmic antibody; CMV: cytomegalovirus; EBV: Epstein–Barr virus; HSV: Herpes simplex virus; VZV: Varicella-zoster virus.
Initial management (Figure 2) includes crystalloid-based volume replacement to counteract hypovolaemia, initiating broad spectrum antimicrobial agents and starting NAC (which increases glutathione levels). They should be initiated as soon as practically possible and should be continued regardless of paracetamol levels. 4 Most patients with hyper acute liver failure need to be looked after in a critical care environment as extra hepatic organ dysfunction is common and deterioration can be rapid. All cases of hyper acute liver failure should be referred to critical care and discussed with a transplant centre as soon as possible.
Neurological care
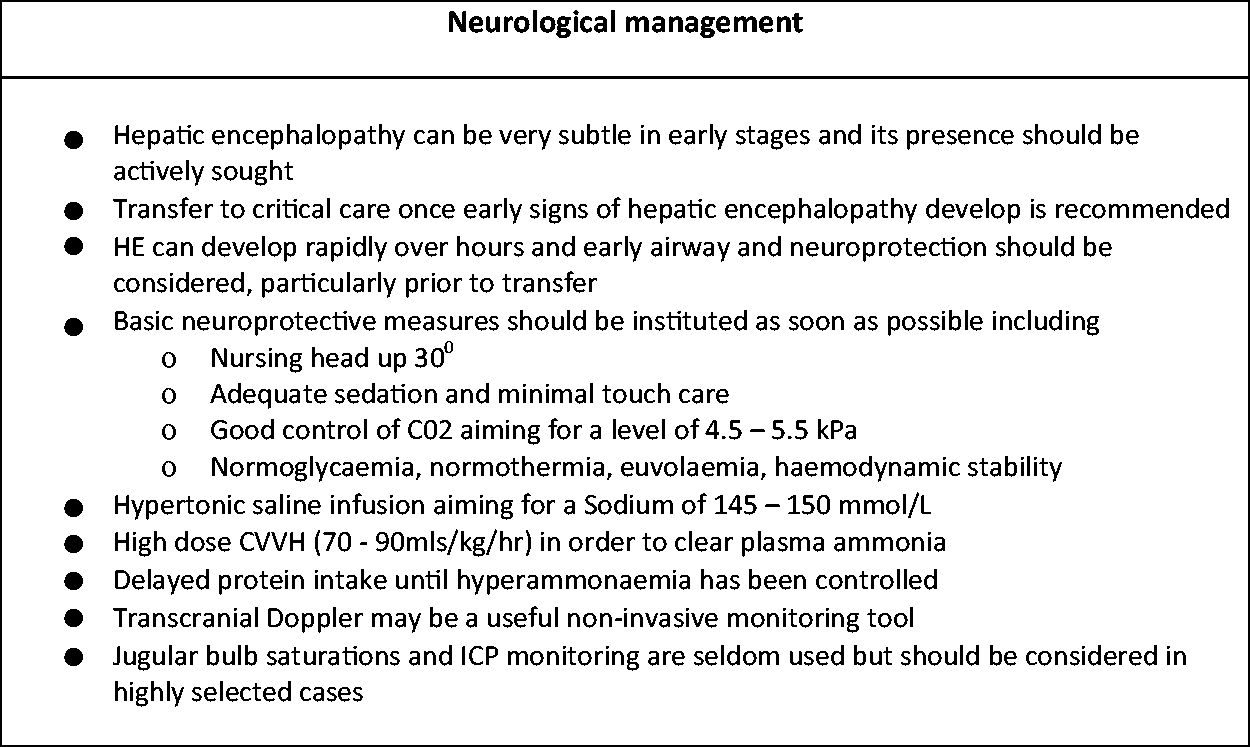
A common cause of death and therefore a main focus of supportive treatment is cerebral oedema (CO). Circulating ammonia levels are associated with the development of HE and CO. Circulating ammonia increases when hepatic ammonia detoxification through the urea cycle is impaired. This is exacerbated by the impaired excretion of ammonia due to concurrent renal dysfunction. Ammonia easily crosses the blood brain barrier, is a potent neurotoxin and leads to the impairment of multiple metabolic pathways within astrocytes leading to cell swelling and cell death. 5 High and persistent ammonia levels are associated with an increased risk of intracranial hypertension (ICH) and cerebral herniation.6,7 Hyponatraemia, a common finding in ALF, further exacerbates CO and the risk of ICH. 8 Unfortunately, cerebral autoregulation, which should preserve cerebral blood flow in the face of hypotension, is lost in ALF so that reductions in mean arterial pressure result in a reduction in cerebral perfusion. 9 On the other hand cerebral hyperaemia, often exacerbated by sepsis, can also provoke ICH. The prevention and control of infection is therefore highly important for this group of patients particularly as bacterial infection has been demonstrated in up to 80% of ALF patients and fungal infection in 32%. 10
As HE can be subtle in early disease, and can progress rapidly over hours to coma and ICH, transfer to critical care once HE develops is recommended. This allows for neuroprotective measures and airway protection to be delivered in a timely manner. Basic neuroprotective measures should be initiated from the outset. Control of serum ammonia is of paramount importance to reduce the risks of intracranial hypertension. High dose haemofiltration has been shown to clear serum ammonia in a dose dependent manner. 11 High dose CVVH should be initiated early in patients with ALF, particularly if high grade HE is predicted and even in the absence of renal dysfunction. Ammonia production is theoretically minimised by short term protein restriction. The European Society for Clinical Nutrition (ESPEN) recommends deferring protein intake for 24 – 48 hours until hyperammonaemia is controlled. 12 When protein is introduced, serum ammonia levels should be monitored to ensure hyperammonaemia does not recur.
There have been four randomised controlled trials of treatments for neurological care in acute liver failure. The use of prophylactic phenytoin did not reduce the frequency of subclinical seizures or CO in ALF. 13 L-ornithine L-aspartate (LOLA) infusion was trialled to assess if it could usefully reduce ammonia. When compared to placebo, LOLA use over 3 days did not lower serum ammonia or improve survival in ALF. 14 In a trial comparing the use of prophylactic therapeutic temperature management (34°C vs 36°C) to prevent ICH, lower temperatures did not reduce the incidence of ICH nor improve survival in ALF. 15 On the other hand, the use of hypertonic saline to maintain Na levels in the range 145–150 mmol/L significantly reduced the risk of intracranial hypertension. 8 This treatment should therefore be initiated as soon as practically possible in high risk or hyponatraemic patients.
Intracranial pressure monitoring is less commonly used in the UK nowadays due to the uncertainty of benefit compared to harm during patient management; there is observational data suggesting that intracranial pressure monitoring may not improve outcomes for these patients. 16 Transcranial Doppler, jugular venous bulb saturations and serial CT imaging have also been used to aid management but are neither validated nor commonplace. A summary of neurological management is presented in Figure 3.
Cardiovascular care
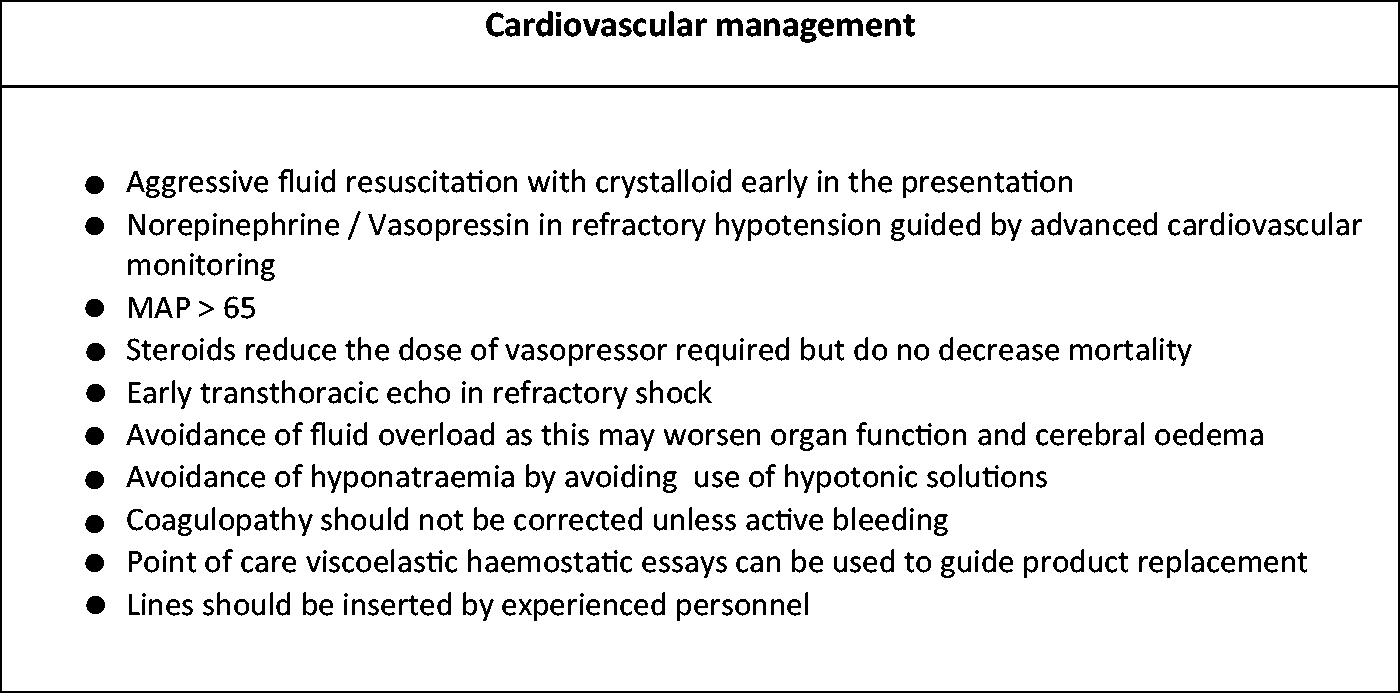
Most patients with acute liver failure are initially volume deplete. Arterial lactate is usually markedly elevated on presentation, reflecting both hypovolaemia and the impaired clearance of lactate by the failing liver. Volume resuscitation with crystalloid solution is required in order to restore circulating volume. There is no evidence favouring one crystalloid over another and the EASL guidelines recommend the use of 0.9% NaCl or balanced crystalloid solutions that do not require hepatic metabolism. 1 Studies show many patients have a hyper dynamic circulation in ALF; one study found a mean cardiac index of 4.3 L/min. 17 Persistent hypotension once adequate volume resuscitation has been carried out is likely to be due to vasodilatation and the use of vasopressors such as norepinephrine and vasopressin guided by advanced cardiovascular monitoring is recommended. A MAP target has not been defined in the literature but experts recommend a MAP ≥ 65 mmHg to ensure adequate cerebral and systemic perfusion. It is recommended to obtain a transthoracic echocardiogram to rule out any significant cardiac disease. Steroids reduce the dose of vasopressor required but have not been shown to reduce mortality. It is important to avoid fluid overload as this is linked to peripheral oedema which may worsen organ dysfunction and drive intracranial hypertension.
Derangements in INR are often severe in acute liver failure but due to the INR being of prognostic importance, correction is avoided unless bleeding occurs or high risk interventions are planned. The reduction in pro-coagulant factors is paralleled by a reduction in anti-coagulant factors such as proteins C & S. As a result a balanced coagulopathy occurs without an increased bleeding tendency. 18 Point of care viscoelastic haemostatic essays (TEG/ROTEM) may be useful if clinical doubt exists. A summary of cardiovascular management is presented in Figure 4.
Respiratory care
Specific respiratory issues in acute liver failure are uncommon and related to usual complications of critical care, including aspiration and ventilator associated pneumonia. Suctioning of the respiratory tract and physiotherapy should be undertaken carefully due to the increased risk of bleeding and raised ICP.
Renal management
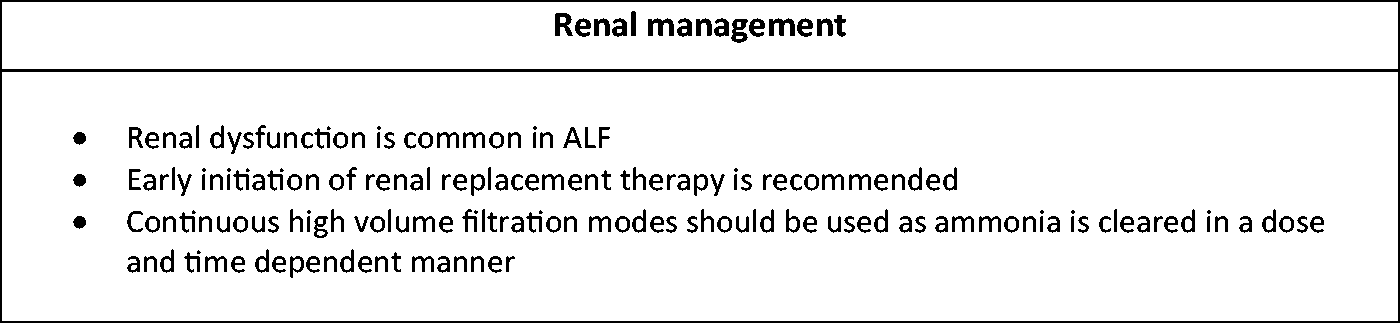
Renal dysfunction in acute liver failure is very common and forms part of the poor prognostic criteria. As well as the common indications for renal replacement therapy, early initiation is specifically recommended for control of ammonia and metabolic acidosis (Figure 5). Ammonia is cleared from the plasma in a dose dependent manner with no evidence of a plateau. 11 High volume continuous haemofiltration 70–90 mls/kg/hr is therefore recommended. Continuous renal replacement therapy has been shown to have superior outcomes when compared with intermittent replacement therapies. 19
Transfer to a transplant centre – When and how
As hyper acute liver failure is rare, the experience of specialised units is needed in order to optimally manage these patients. Transfer should be considered in patients with significant acidosis despite fluid resuscitation (pH < 7.3), a requirement for glucose support, an associated AKI or any degree of encephalopathy. 1 Due to the severe and dynamic nature of ALF, the transfer of these patients should involve experienced clinicians. Intubation prior to transfer should be considered in all patients with encephalopathy and transfer should be in accordance with established critical care transfer guidelines. Rescue neuroprotective therapies such as hypertonic fluids, hyperventilation and barbiturates should be available.
Liver transplantation
Liver transplantation for POD induced ALF is considered in patients who are unlikely to survive with medical treatment alone. The Kings College Criteria (Table 5) were derived from a 566 patient dataset from the ‘70 s & ‘80 s, and are used to identify this subgroup. 20 Due to improvements in the survival of medically managed patients over the last 20 years it has become less clear which patients will do poorly without transplantation. 21 Newer paracetamol specific scoring systems which assess dynamic changes in patient status have been devised. 22
Kings College Hospital Criteria for liver transplantation in paracetamol induced ALF.
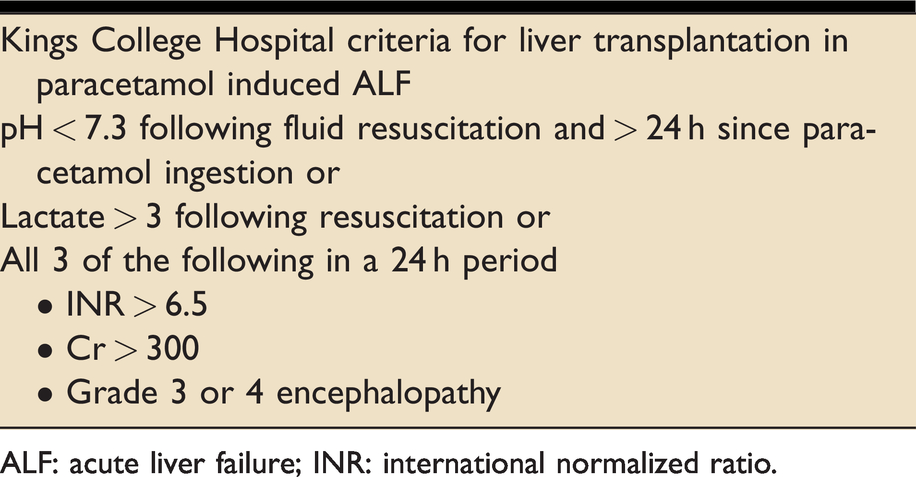
ALF: acute liver failure; INR: international normalized ratio.
Plasma exchange
As a result of a randomised control trial, transplant centres are increasingly using high volume plasma exchange for patients with severe ALF that cannot be transplanted. In this trial plasma exchange led to a significant improvement in survival when compared to standard medical therapy, though this was isolated to the group of patients with ALF who did not undergo transplantation. 23 Furthermore the use of plasma exchange is highly resource intensive, removes the best indicator of liver synthetic function from the clinician’s toolkit and may therefore adversely prejudice decisions around transplant listing. Therefore outside of transplant centres, plasma exchange should only be used for patients with ALF under exceptional circumstances and following discussion with the local transplant centre. There is currently no evidence that supports the use of any other extracorporeal liver support device in ALF.
Conclusions
Paracetamol induced hyper acute liver failure is a rare condition manifesting with a clinical triad of liver-related coagulopathy, jaundice and encephalopathy. Aggressive critical care treatments emphasising neuroprotection, ammonia clearance and emergency liver transplantation in specific cases has led to progressive improvements in survival. Therefore early critical care admission and discussion with a transplant centre should be considered for all cases. Transplant-free survival in POD-ALF is improving so that identifying patients who will truly benefit from transplantation is becoming more difficult.
FFICM curriculum covered
Top 30 Cases: Case 12 – Acute liver failure following paracetamol overdose.
Domains: 3.5, 3.10, 4.8, 7.1 and 10.1 Domain 3.5 – Recognises and manages the patient with, or at risk of, acute liver failure Domain 3.10 – Recognises and manages the patient following intoxication with drugs or environmental toxins Domain 4.8 – Recognises and manages electrolyte, glucose and acid -base disturbances Domain 7.1 – Identifies and attempts to minimise the physical and psychosocial consequences of critical illness for patients and families Domain 10.1 – Undertakes transport of the mechanically ventilated critically ill patient outside the ICU
Consultant appraisal and revalidation items covered
Update in management of acute liver failure following paracetamol overdose When to admit to critical care, initial stabilisation and management When to refer and transfer to a transplant centre
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.