
Abstract
Background
ICU patients may require renal replacement therapy (RRT). Sharing RRT equipment carries a risk of BBV transmission, which mainly relates to Hepatitis B (HBV), Hepatitis C (HCV) and HIV. Since 2012, all Glasgow Royal Infirmary ICU patients undergo routine BBV screening, with RRT machines allocated for patients with specific BBV statuses. Routine BBV testing is beneficial to both the individual and society. This study aims to determine if routine BBV testing in the ICU contributes to the discovery of undiagnosed BBV infections.
Methods
This single-centre retrospective observational study examined prospectively collected clinical data from 1069 ICU admissions. Proportions were compared using a two-proportion z-test and a logistic regression model was carried out to determine if deprivation quintile was independently associated with the seroprevalence of BBVs.
Results
The BBV seroprevalence in the cohort studied: 0.45% (HBV), 11.7% (HCV), and 0.91% (HIV). The seroprevalence of HBV in the cohort studied was similar to that of Scotland (p = 0.11), but the seroprevalence of HCV (p < 0.001) and HIV (p = 0.01) were significantly higher than that of Scotland. The relationship between deprivation and BBV seroprevalence was explored for HCV only. The only independent variable associated with a reactive anti-HCV test result was “current or previous illicit drug use” (adjusted odds ratio of 40.2; 95% confidence interval of 21.1–76.4; p < 0.001).
Conclusion
This study shows that routine BBV testing in the ICU is useful in discovering new BBV infections. This is the first observational study focusing on the value of routine BBV testing in an ICU setting to our knowledge.
Introduction
Acute kidney injury (AKI) affects 40–57% of critically ill patients, 1 and is associated with high mortality and morbidity. In the intensive care unit (ICU), patients with AKI require renal replacement therapy (RRT) to mitigate complications of fluid overload, refractory hyperkalemia and metabolic acidosis. Sharing of RRT equipment between ICU patients carries a potential risk of transmission of blood-borne viruses (BBVs), despite decontamination and the use of disposable components. The main risks relate to Hepatitis B (HBV), Hepatitis C (HCV) and human immunodeficiency virus (HIV). 2
A method to minimise the risk of BBV transmission between ICU patients on RRT would be to allocate dedicated RRT machines to patients with specific BBV statuses. Each patient would then only use an RRT machine that was previously used by another patient with the same BBV status. This method would require ICU patients to be screened for BBVs before commencing RRT.
Prior to 2012, ICU patients at the Glasgow Royal Infirmary (GRI) were selectively screened for BBVs if deemed to require RRT based on the aforementioned complications of AKI. Often, patients had to commence RRT before the BBV test results were produced, and thus allocated to any available RRT machine. If the patient’s BBV status turned out to be different from the RRT machine used, the machine would have to be removed from use to be disassembled and thoroughly decontaminated. This is problematic as it limits the number of RRT machines which are then available for use. To avoid the risk of insufficient RRT machines being available for use, since 2012 all patients have been routinely screened for BBVs upon admission to ICU. This allows for appropriate allocation of RRT machine and minimises delay in RRT commencement if the patient does require RRT later.
Aside from its use in determining RRT machine allocation, routine BBV testing allows patients to be aware of their BBV status. BBVs are associated with significant mortality and morbidity worldwide, and knowing one’s status is beneficial to both the individual and society. The individual can commence treatment at the earliest and may avoid long-term complications of the disease – cirrhosis and hepatocellular carcinoma for HBV/HCV, full-blown AIDS for HIV. In addition, the patient can make appropriate lifestyle changes and avoid high-risk behaviours to reduce BBV transmission, thus benefiting society. HCV is a pertinent issue in Scotland, with approximately 34,500 people chronically infected with HCV and over 40% of this population remaining undiagnosed. The Scottish government aims to eliminate HCV by 2030, and is researching cost-effective and innovative approaches to finding undiagnosed patients. 3 Current relevant studies comprise some seroprevalence surveillance studies in emergency departments4,5 and primary care 6 across the UK, but none in the ICU setting.
The aim of this study is to determine if routine BBV testing in ICU patients contributes to the discovery of undiagnosed patients with BBVs. The objectives of this study are to compare the seroprevalence of BBVs between the cohort studied and that of Scotland, to determine the incidence rates of new reactive BBV test results in the cohort studied, and to determine the relationship between deprivation and the seroprevalence of BBVs.
Methods
Ethics
As all required information was collected prospectively as part of routine clinical care and the results of the study would be fully anonymised, this study was confirmed to not require approval by an NHS Research Ethics Committee or NHS Greater Glasgow and Clyde Research and Development Department prior to data collection.
Study design, location and participants
This retrospective observational study was conducted over a seven-month period, from 27 September 2018 to 16 April 2019, in the ICU of a 1000-bed teaching hospital (Glasgow Royal Infirmary, Scotland, United Kingdom). All data had been collected prospectively for clinical purposes and was available from IntelliSpace Critical Care & Anesthesia (Philips) and NHS Clinical Portal.
The inclusion criteria were the following: all level three GRI ICU index admissions from 1 January 2015 to 31 December 2018, with an ICU stay of three days or more. Level three patients in ICU refer to those who require advanced respiratory support alone or monitoring and support for two or more organ systems. An index ICU admission refers to the first ICU admission within a hospital admission. Exclusion criteria were age under 16, non-index ICU admissions and patients with incomplete postcodes or postcodes outwith Scotland. The cohort studied consisted of 1069 ICU admissions. Figure 1 shows the selection of eligible admissions included in this study.
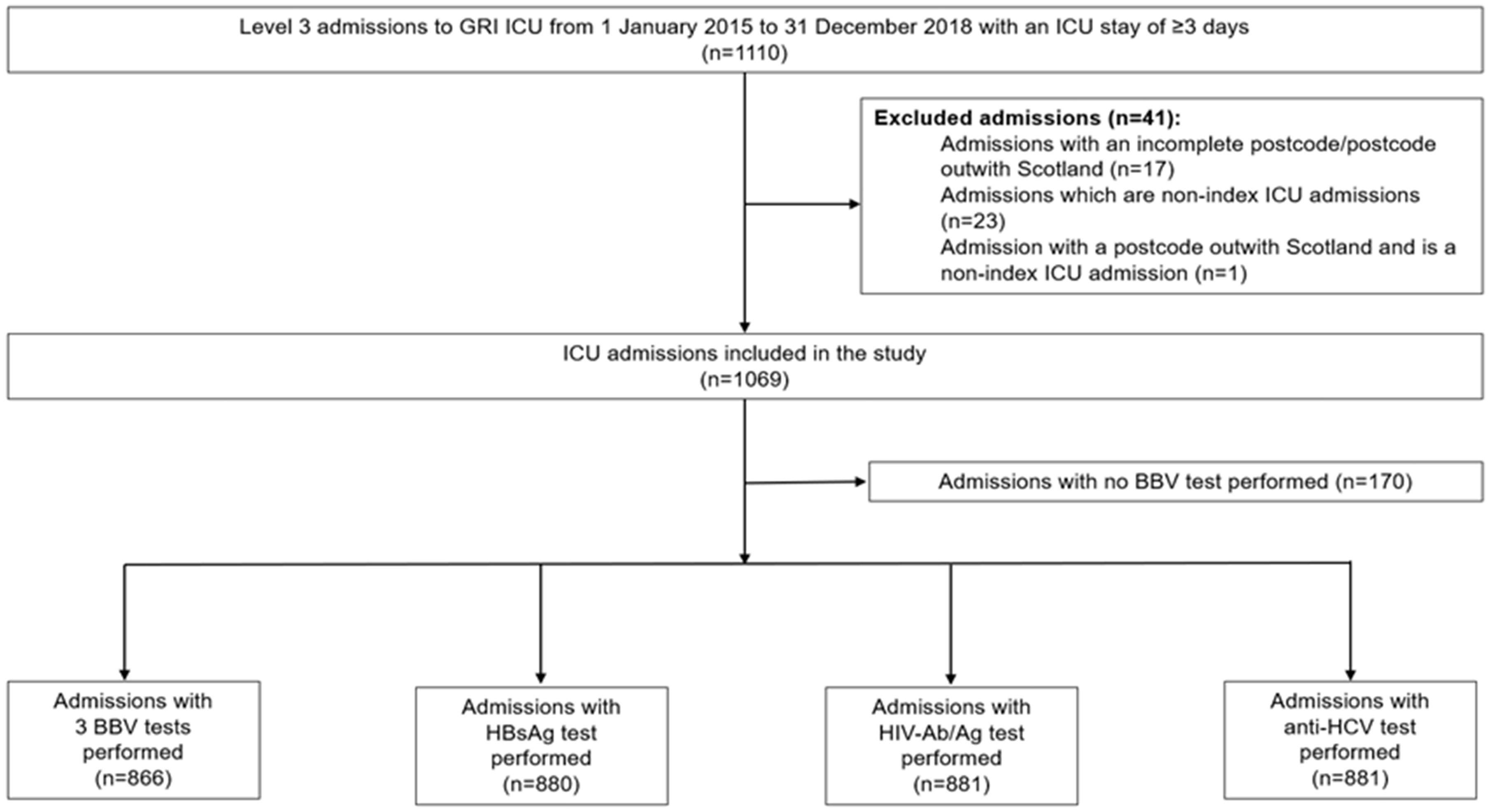
Study consort diagram. Flow diagram showing selection of eligible admissions included in the study.
Data collection
The following data, available in medical records, were collected for every included ICU admission: age, gender, postcode, type of ICU admission (medical or surgical), evidence of illicit drug use (current or previous), evidence of alcohol excess (current or previous), vital status at ICU discharge (alive or deceased), length of ICU stay, and BBV test results in the admission. Postcodes were matched on the Scottish Index of Multiple Deprivation (SIMD) 2016 Index Lookup 7 to determine its allocated deprivation quintile. Medical ICU admissions included patients suffering from medical conditions, while surgical ICU admissions included patients who recently had surgery or could potentially require surgery. Evidence of illicit drug use and alcohol excess were obtained from past medical history. For each BBV test result, the following were recorded: status (reactive/positive or non-reactive/negative) and evidence of previous tests. If the test showed a positive status and there were no previous tests, the result would be recorded as a “first positive”. For positive HCV-antibody (anti-HCV) test results, the associated HCV-RNA/antigen test result was also recorded. A positive anti-HCV test with a positive HCV-RNA antigen test was classified as “viraemic HCV infection”, while a positive anti-HCV test with a negative HCV-RNA/antigen test was classified as “non-viraemic HCV infection”.
Statistical analyses
Continuous variables were expressed as medians and interquartile ranges. Proportions were compared using a two-proportion z-test on Minitab 17 Statistical Software. The tests were two-sided and a p-value of less than 0.05 was considered to be statistically significant. A logistic regression model was carried out on IBM SPSS Statistics 21 to determine if deprivation quintile was independently associated with the seroprevalence of BBVs. Variables with p-value less than 0.10 in the univariate analysis were entered in the final models. The results were expressed in terms of the odds ratio (OR) with a corresponding 95% confidence interval (CI).
Results
Patient characteristics
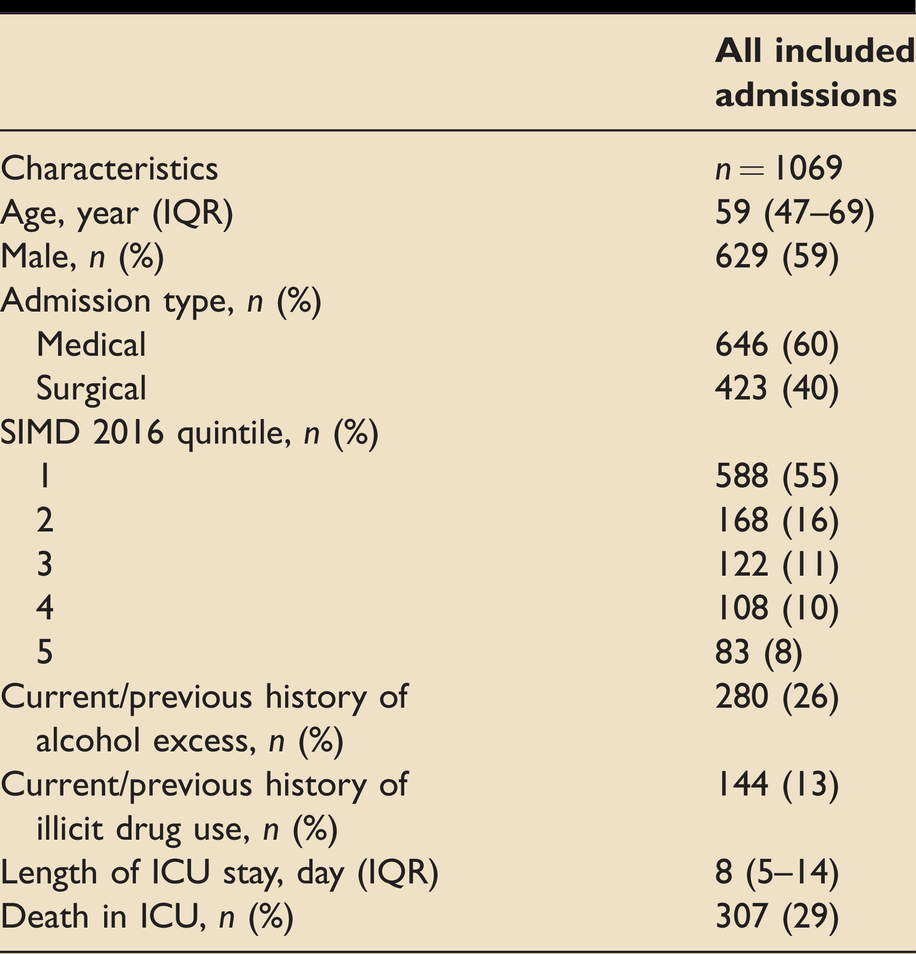
The baseline characteristics of patients in all included admissions are shown in Table 1. In total, 1069 admissions were studied. The median age of patients studied was 59 (47–69) years old, and males represented nearly 60% of all patients. Medical admissions constitute 60% of the included admissions. The median length of ICU stay was 8 (5–14) days, and nearly 30% of patients died in the ICU. Over half of the patients reside in SIMD deprivation quintile 1 postcodes (most deprived), and less than 10% reside in deprivation quintile 5 (least deprived) postcodes. Approximately 25% of patients had a current/previous history of alcohol excess, while 13% had a current/previous history of illicit drug use.
Baseline characteristics of patients in all included admissions.
Comparison of BBV seroprevalence between GRI ICU and Scotland
Of 1069 admissions, at least one BBV test was performed in 899 admissions, and 866 admissions received all three BBV tests. Table 2 shows the number of each BBV test performed, the number of reactive test results and seroprevalence of each BBV in the cohort studied and Scotland. The number of individual BBV tests performed: 880 HBV surface antigen (HBsAg) tests, 881 HCV-antibody (anti-HCV) tests and 881 HIV-antibody/antigen (HIV-Ab/Ag) tests. The number of reactive tests for each BBV: 4 HBsAg tests, 103 anti-HCV tests and 8 HIV-Ab/Ag tests. The seroprevalence of each BBV was calculated as (number of reactive tests results)/(total number of tests performed). The seroprevalence of each BBV in the cohort studied: 0.45% (HBV), 11.7% (HCV), and 0.91% (HIV). The seroprevalence of HBV in the cohort studied was similar to that of Scotland (p = 0.11), but the seroprevalence of HCV (p < 0.001) and HIV (p = 0.01) were significantly higher than that of Scotland. 8
Comparison of seroprevalence between GRI ICU and Scotland, and incidence rates of new reactive BBV tests in GRI ICU.
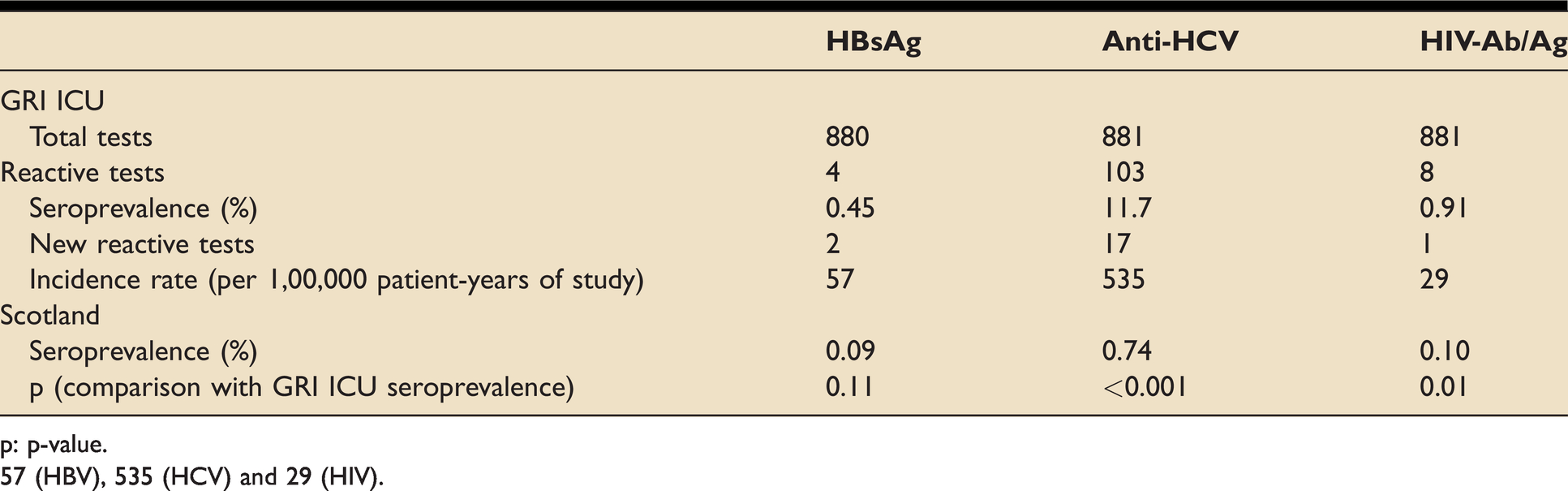
p: p-value.
57 (HBV), 535 (HCV) and 29 (HIV).
Incidence rates of new reactive test results
The incidence rate of new reactive test results for each test is shown in Table 2 and is calculated by
The incidence rates of new reactive test results (per 100,000 patient-years of study).
Relationship between deprivation and BBV seroprevalence
Due to the small number of reactive test results for HBV and HIV, the relationship between deprivation and BBV seroprevalence was explored for HCV only. Table 3 shows the logistic regression model results, with recorded clinical data up to the time of BBV testing as independent variables, and a reactive anti-HCV test result as the dependent variable. All five SIMD 2016 deprivation quintiles were not independently associated with a reactive anti-HCV test result. In addition, current or previous history of alcohol excess was not independently associated with a reactive anti-HCV test result. The only independent variable associated with a reactive anti-HCV test result was current or previous illicit drug use (adjusted OR of 40.2; 95% CI of 21.1–76.4; p < 0.001).
Unadjusted and adjusted odds ratios (ORs) for reactive anti-HCV test results.
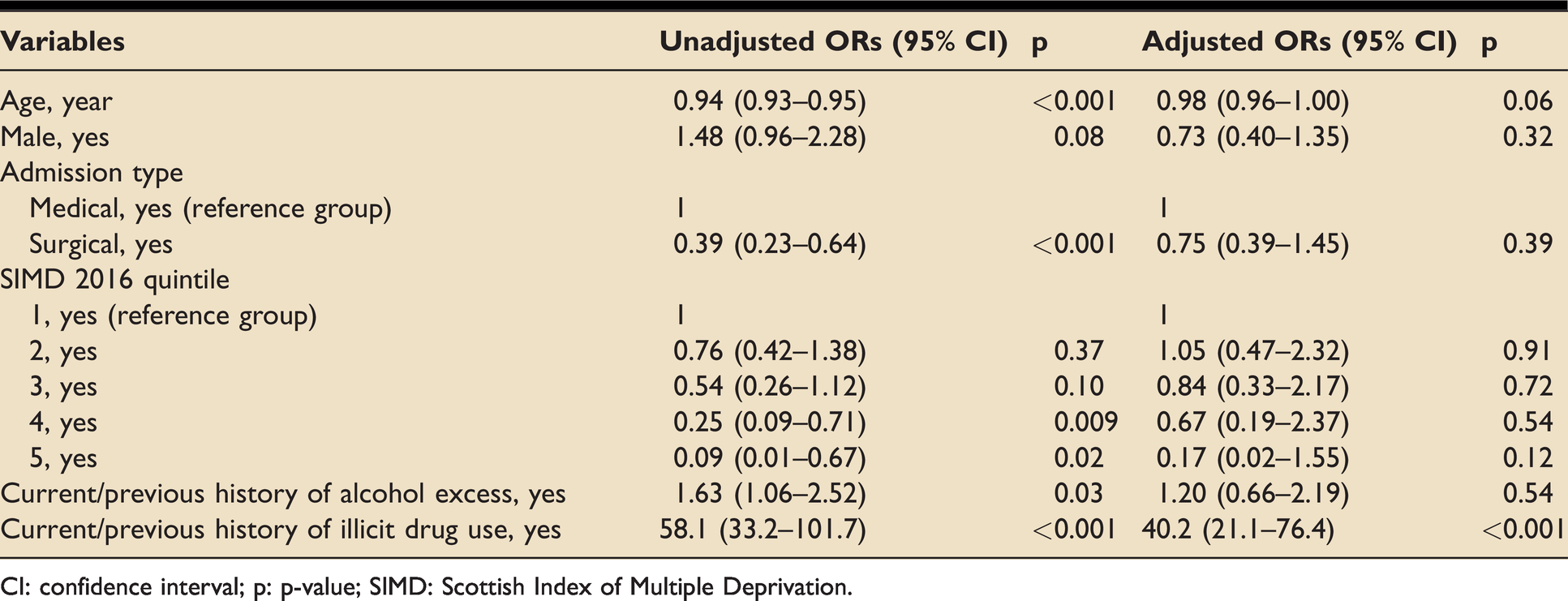
CI: confidence interval; p: p-value; SIMD: Scottish Index of Multiple Deprivation.
Viraemic HCV seroprevalence and incidence rate of new reactive test results
For patients with a reactive anti-HCV result, HCV-RNA/antigen tests were performed to determine viraemic or non-viraemic HCV infection. Although this was not a primary objective of this study, it was possible to calculate the seroprevalence and incidence rate of viraemic HCV infections. Of 881 anti-HCV tests performed, there were 51 reactive HCV-RNA/antigen test results, of which 10 were new reactive test results. This gives a viraemic HCV seroprevalence of 5.8%, and an incidence rate of new reactive test results of 298 per 100,000 patient-years of study.
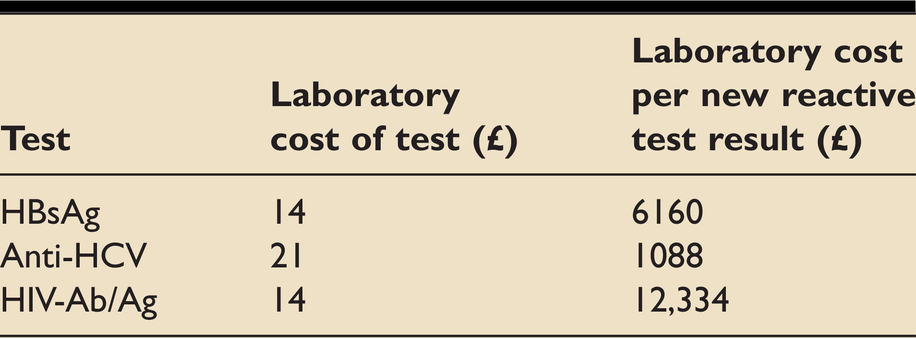
Laboratory cost per new reactive test result
The approximate laboratory costs for each BBV test were obtained from the relevant department (Booth MG, personal communication, 2019), and the laboratory cost per new reactive test result could be calculated (Table 4): £6160 (HBsAg), £1088 (anti-HCV) and £12,334 (HIV-Ab/Ag).
Laboratory costs of BBV tests and calculated laboratory cost per new reactive test result.
Discussion
In this study, routine BBV testing was supposed to be carried out for all included ICU admissions. However, only approximately 81% of included patients received all three BBV tests, with 16% of included patients not receiving a single BBV test. This highlights the lack of a strict protocol to ensure that all ICU patients receive three BBV tests in their index ICU admission. A more thorough protocol should be in place to ensure no ICU patient misses the BBV tests and thus avoid the missed opportunity to potentially detect a new reactive test result.
This observational study shows that routine BBV testing in the GRI ICU is useful in discovering new reactive BBV test results. This is beneficial for both the individual and society – allowing the patient to commence treatment without delay, and modifying behaviour and lifestyle to prevent transmission of the BBV. Similarly, a large seroprevalence surveillance study conducted across nine emergency departments in the UK also discovered new reactive BBV test results. 4 The cohort studied had a higher HIV and HBV seroprevalence, but a lower HCV seroprevalence compared to this study. Although routine BBV testing is useful in discovering new reactive BBV test results, the costs should be considered in a holistic evaluation of its usefulness. The laboratory cost per new reactive test result in this study is higher than that in the larger aforementioned study. The laboratory cost per new HIV test result in the cohort studied was £12,334 but this could be attributed to its undiagnosed HIV seroprevalence of 0.11%. For HIV screening, an undiagnosed seroprevalence of 0.1% is consistently considered to be cost-effective. 9 As such, the high laboratory cost per new reactive HIV test result in the cohort studied does not necessarily diminish the value of routine BBV testing in this cohort.
In this cohort, over half of the patients resided in the most deprived areas of Scotland (SIMD deprivation quintile 1). This skewed representation of deprivation quintiles is typical of patients admitted to the GRI, as the GRI receives patients residing in the more deprived areas of Glasgow. Despite this, there was no association between SIMD deprivation quintile and anti-HCV seroprevalence after adjusting for the other independent variables. Current or previous illicit drug use was the only independent variable associated with higher anti-HCV seroprevalence. A possible explanation could be the collinearity between SIMD deprivation quintile and illicit drug use, with a larger number of illicit drug users residing in the most deprived quintiles. In addition, it was not possible to categorise illicit drug use into different routes, thus the association between people who inject drugs (PWID) and HCV seroprevalence could not be confirmed.
The initial objective was to explore the association between deprivation and the seroprevalence of all three BBVs. However, as BBV seroprevalence is typically a low percentage, sufficient numbers for HBV and HIV seroprevalence were not obtained. An assumption for carrying out a logistic regression is to have a sample size of at least ten times the number of variables tested. Only the numbers for anti-HCV seroprevalence fulfilled this assumption thus only the association between SIMD deprivation quintile and anti-HCV seroprevalence could be explored.
There are several limitations to this study. This observational study was based on the GRI ICU, so the results may not be applicable to the ICU in other hospitals. Majority of the patients admitted to the GRI reside in the more deprived areas of Glasgow, and this could lead to a very skewed representation of deprivation quintiles. The numbers obtained for BBV seroprevalence was very low, and this is expected as reactive BBV test results are typically regarded as rare events. As a result, the numbers in this study could be used to aid statistical power calculation for larger studies in the future. Furthermore, illicit drug use and alcohol consumption are social risk factors provided by patients, and there could be respondent bias if patients do not truthfully report them, leading to underestimation of these numbers.
Conclusions
This is the first observational study focusing on the value of routine BBV testing in an ICU setting to our knowledge. The BBV seroprevalence in the cohort studied is higher than that of Scotland. Among the independent variables studied, only “current or previous illicit drug use” was associated with a higher anti-HCV seroprevalence. Larger observational studies with more information on all associated costs are required to fully evaluate the value of routine BBV testing in the ICU.
Footnotes
Author’s contributions
YYT: Literature review, data acquisition, data analysis, data interpretation, reporting. MGB: Conception of research, initial design of research, reviewing.
Acknowledgements
Participating investigators: YYT is very grateful to Dr Shaw, who provided his expert advice on statistical analysis strategy and interpretation. This work was performed at the Glasgow Royal Infirmary.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NHS Greater Glasgow and Clyde.