
Abstract
Introduction
The aim of this study was to investigate nurse and allied health professional experiences and attitudes toward critical care research in Wales.
Methods
Data were collected related to demographic characteristics, involvement in and understanding of research, perceived influences and attitudes towards research. We calculated means (ranges) for continuous variable and frequencies (proportions) for discrete variables and performed an exploratory factor analysis.
Results
Response rate was 55% (n = 575). Most respondents (84%) had participated in research less than five times in the previous 12 months, yet 91% believed research led to improved care patients. Only 32% respondents felt they were encouraged by managers to participate in research. Only 25% respondents had undertaken research training. Few respondents (29%) reported receiving adequate information regarding study progress or results (25%). Linear regression models indicate that a higher level of formal education was associated with a more positive view of research across all attitude factors. Promotion of research by colleagues and recognition/ opportunities for involvement in critical care research, were positively associated with the acceptability and experience of research.
Discussion
A number of factors have been identified that could be targeted to improve recruitment to critical care research, including identification of staff to promote research, improved communication of study progress and findings and management encouragement to attend research training. Staff attitudes were positive towards the benefit of research on patient care in Wales.
Background
Evidence suggests that healthcare systems that actively engage in clinical research report better patient outcomes.1–3 High quality clinical research builds institutional reputation, attracts and retains staff. It provides access to novel or expensive therapies that might otherwise be unavailable.4,5 Effective critical care research requires collaborative working between engaged enthusiastic clinicians, research teams and patients and their families, with adequate time, research infrastructure, governance, institutional and academic support. 6 A key action of the Welsh Government’s Critically Ill Delivery Plan (2018) was to increase the number of critical care healthcare professionals engaged in clinical research. 7 The evaluation of interventions designed to improve outcomes for critically ill patients is a key international priority. 8
The critical care environment presents some unique challenges to researchers, especially when the research is related to end-of-life care. Challenges include recruitment barriers such as gaining access to a clinical site or patients, prognostic uncertainty and the time-sensitive nature of interventions in emergency situations. Additional barriers include challenges related to ethical considerations, informed consent, data collection and the research infrastructure at a hospital such as available personnel and funding.7,9
The nurse and AHP role in critical care research may include identification of eligible patients, involvement in the consent process, caring for the patient according to a study protocol, delivering specific study interventions, recording study data and monitoring for adverse events. 10 A recent survey reported that UK critical care physiotherapists are skilled, experienced and motivated to participate in research, including pursuing defined academic research pathways. 11 The study concluded that wide-ranging training needs and notable barriers preclude further involvement of physiotherapists in critical care research. 11 In a similar Canadian study investigating attitudes of nurses to critical care research, results demonstrated that respondents both endorse and participate in research. 12
Limited other evidence exists regarding both nursing and AHP understanding of the critical care research process, and their perceptions of such research in general. Understanding these attitudes and experiences is an important research priority, as the successful delivery and completion of research in a critical care environment is dependent on engagement of nurse and AHP staff. 11
The aims of this study were to: (a) investigate nurse and AHP personal experiences of working in critical care research; (b) describe environmental characteristics that influence the research culture on critical care units; (c) describe nurse and AHP attitudes towards research and (d) compare differences between nurse and AHP attitudes.
Methods
Design and study population
Ethical approval was not needed for the study due to the involvement of NHS staff as research participants. This was confirmed by the study sponsor. The Research and Development Department of each participating site confirmed local approval for the study.
This study used a cross-sectional questionnaire design, in which all nurses and AHPs working in the general intensive care units in Wales were invited to complete either a paper-based or online questionnaire. Figure 1 illustrates the geographical location of the critical care units in Wales.
13
Participation was voluntary and consent implied by questionnaire return. Of the 14 ICUs in Wales, one was unable to participate in the study due to lack of available principal investigator. Nurses and AHPs (physiotherapists, dietitians, pharmacists, speech therapists and psychologists) working in adult, general ICUs in Wales were invited to participate in the study. Map of critical care units in Wales. Permission to re-use figure granted from Welsh Deanery for Dentists.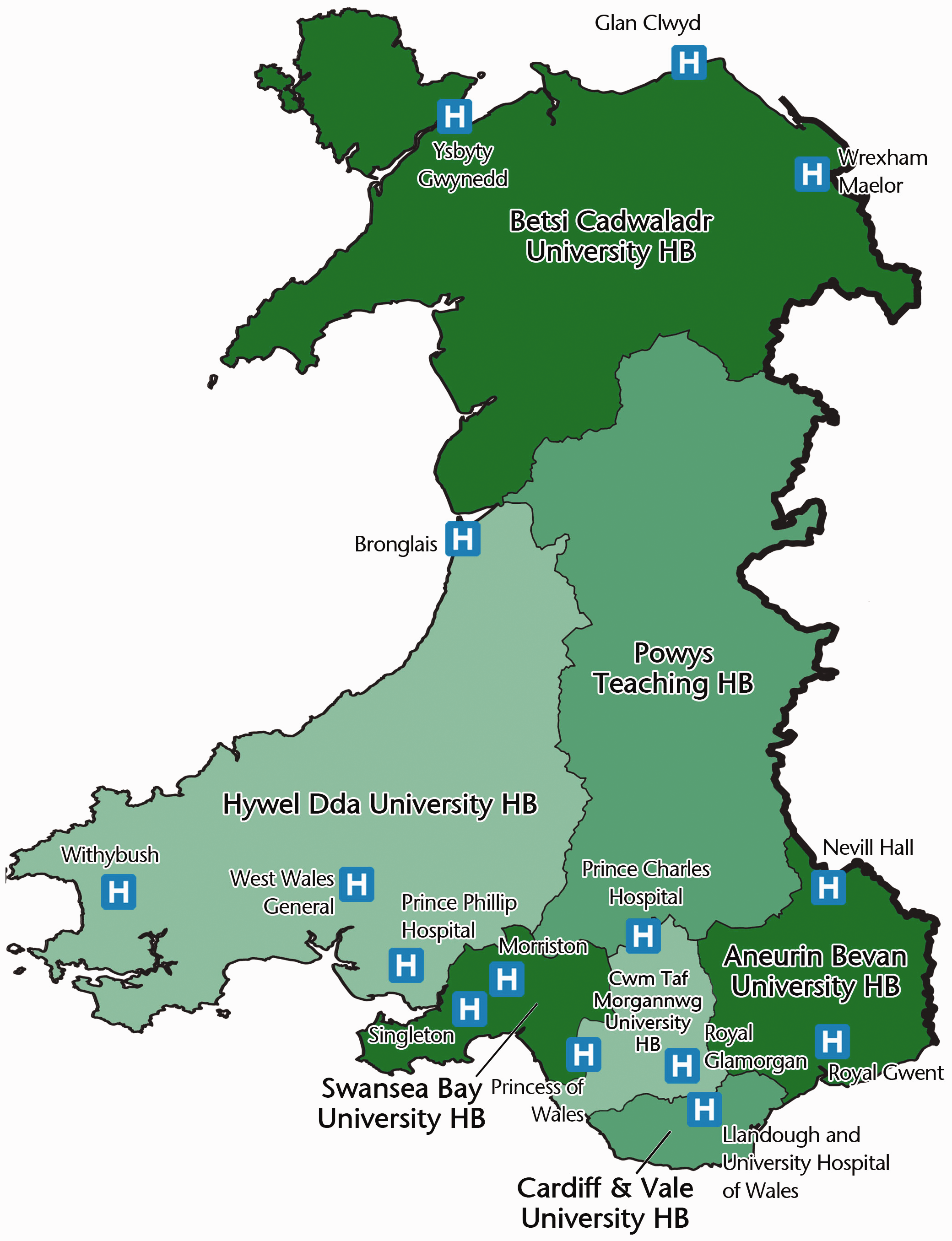
Questionnaire
A previously developed questionnaire was used for this study, with the permission of the authors. 12 The questionnaire consists of four sections; research experience, ICU/hospital characteristics, attitudes about research and demographic data. Respondents are required to complete 64 closed-ended questions and a free-text, open-ended comment section. The questionnaire can be found in Additional file 1 (Supplementary Material). Likert-scale response options (strongly disagree, disagree, unsure, agree and strongly disagree) were used to describe ICU/hospital characteristics and personal attitudes about research.
Paper-based questionnaires were distributed by a principal investigator at each site over a two-month period, to ensure staff on annual/sick leave were included. In some units, posters were used to advertise the study to the staff, which included a link to the online questionnaire. The online questionnaire was developed using SurveyMonkey. 14 Each principal investigator completed a unit data questionnaire, providing details on local demographics including the number of nurses and AHP staff employed.
Statistical analysis
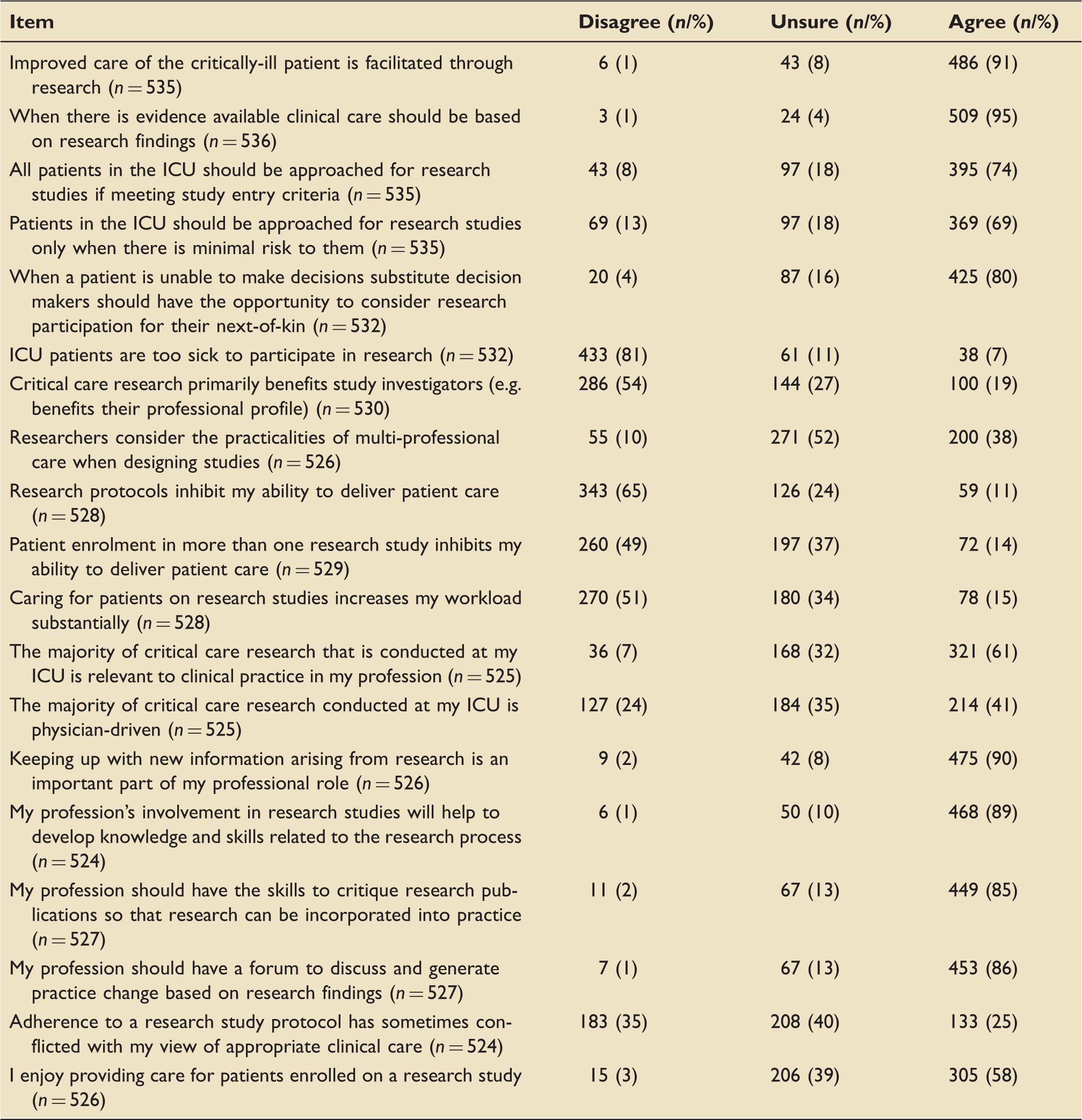
The Likert-scale was scored as 1 for strongly disagree, through to 5 for strongly agree. For the descriptive purposes, the 5-point Likert-scale scores were collapsed into three categories; disagree (1, 2), unsure (3) and agree (4, 5). 12 Responses were analysed using means and ranges for continuous variables and frequencies and proportions for discrete variables. Free text box responses were collated and presented using simple thematic analysis.
Factor analysis was performed using Stata SE version 16.0 on the original Likert-scale scores. Scores were reversed for negatively phrased items. The number of potential factors was identified using a scree plot and parallel analysis. Factors were then rotated obliquely; items that did not load at a threshold of 0.3, or loaded onto more than one factor, were excluded from analysis. The consistency of questionnaire items associated with each factor was assessed using Cronbach’s alpha. A value of 0.7 or greater was considered acceptable. Mean Likert scores were calculated for each factor by averaging the component items (using the reversed scales where appropriate) for each record where at least half the items were completed.
A linear regression analysis accounting for clustering by hospital was performed to examine the relationship between each attitude factor and the three environmental factors, as well as length of time working as a critical care nurse/allied health practitioner, frequency of caring for patients on a research study, experience of developing a research proposal, or analysing research findings and highest qualification level.
Results
Respondent and site characteristics
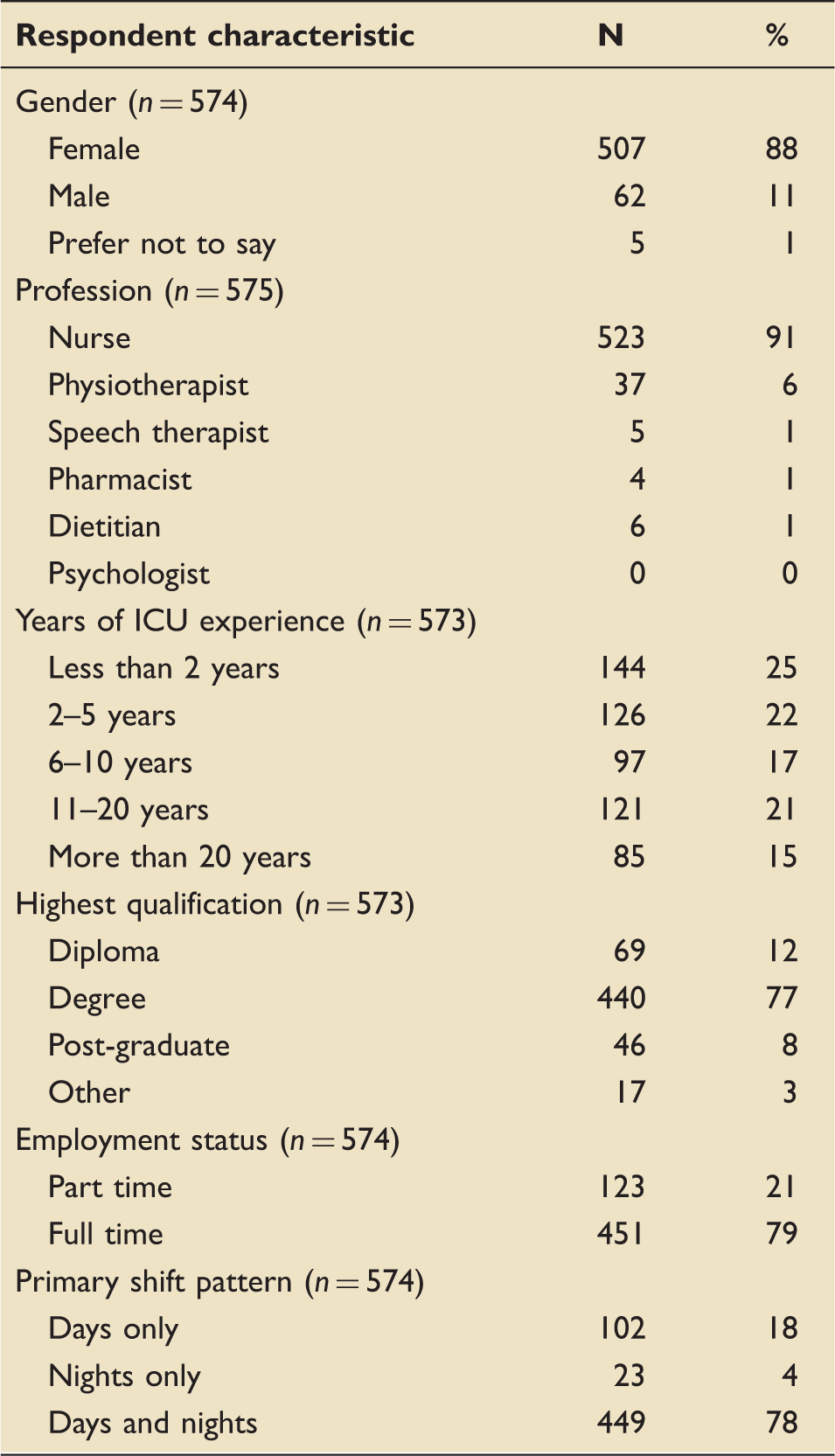
Demographic characteristics of respondents.
Free text responses to the question “what would facilitate the conduct of research studies in your ICU?” included; more protected time to undertake research (n = 42), more dedicated research staff (n = 49), improved communication/information (n = 77), improved collaborative working between whole multi-disciplinary team (n = 15), more funding for staff and/or training (n = 30) and managerial support (n = 2). A number of methods for improving communication were suggested. These included use of posters, a Facebook page, an annual report and a research notice board. The use of plain language was identified as key to improved communication.
Research training, experience and understanding of research activities.
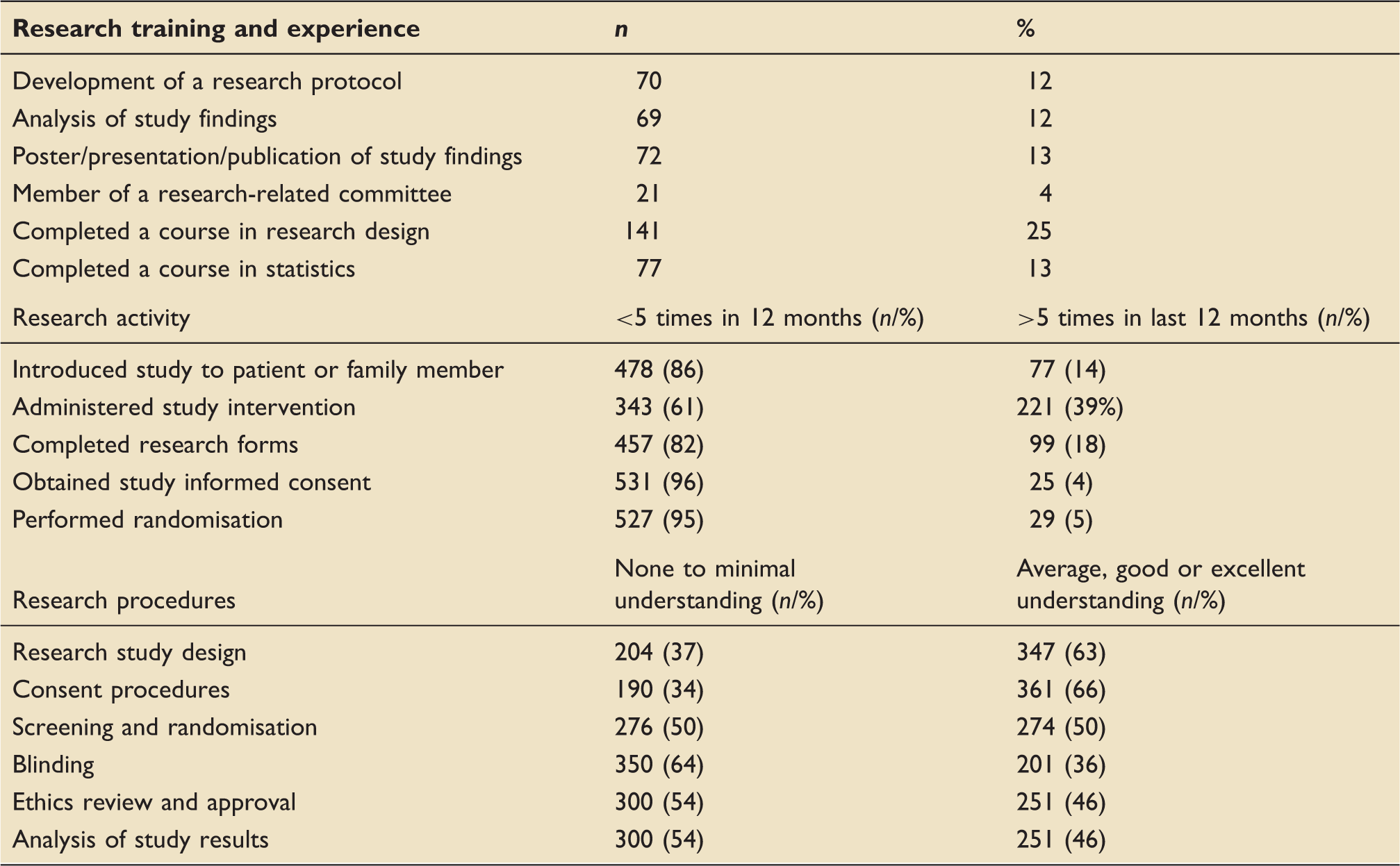
A total of 89/575 (15%) respondents had taken part in a study as a participant and 65 /89 (73%) of these had reported the experience to be either positive or very positive. A total of 86/89 (97%) stated that they would participate in another research study.
Environmental characteristics influencing critical care research
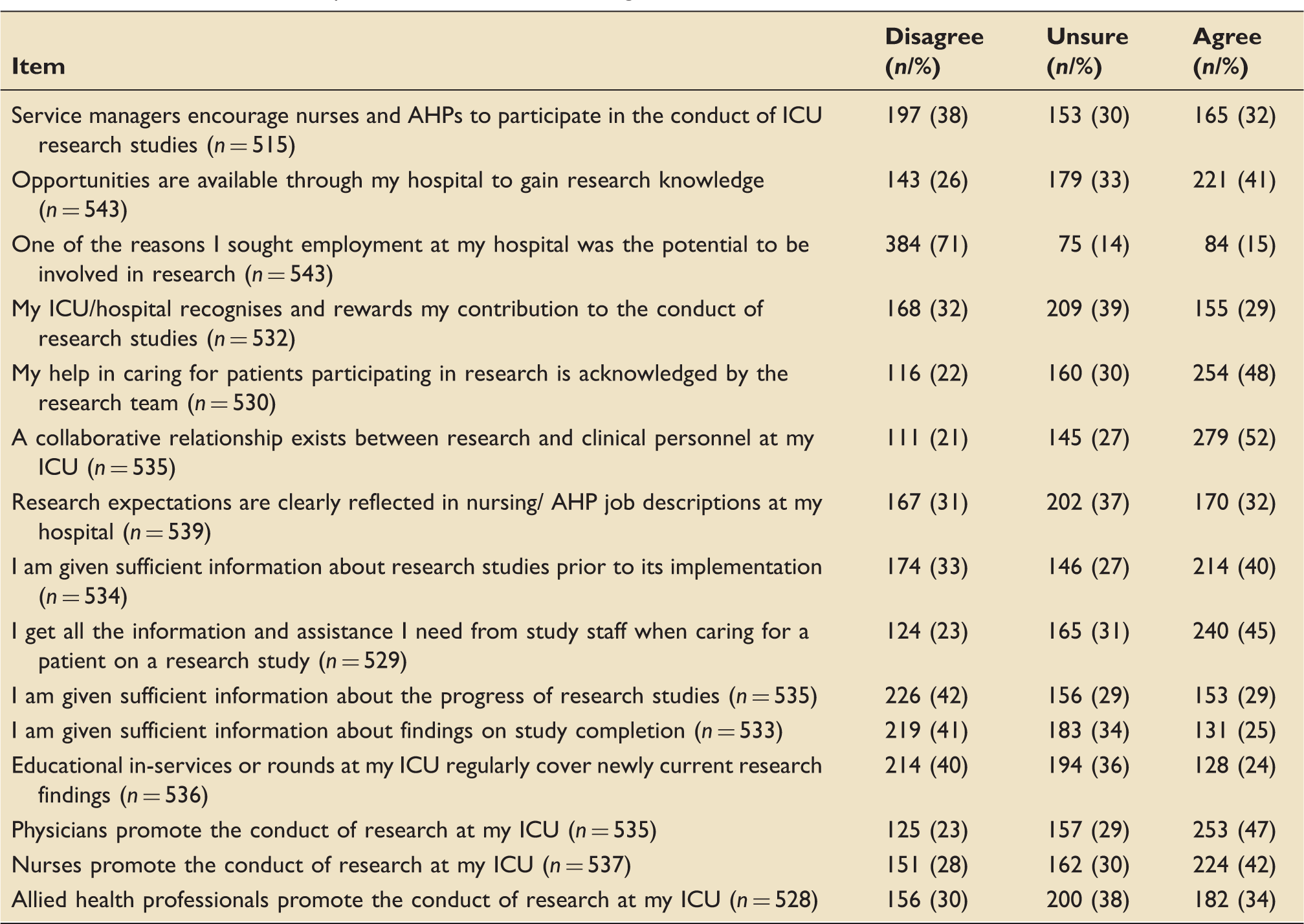
Perceived ICU and hospital characteristics influencing research culture.
Respondent attitudes towards research
Respondent attitudes to critical care research.
Variables associated with environmental factors influencing research
Exploratory factor analysis (see Additional file 2, Supplementary Material) found three environmental factors. Environmental factor E1 was related to the opportunity and recognition to get involved in research (questionnaire items 12 b-12 g and 12 n); factor E2 concerned information about studies (questionnaire items 12i-12 k); and factor E3 concerned promotion of research by managers and other health professionals (questionnaire items 12 a, 12 l, 12 m, 12o). One item (12 h) loaded onto two factors and was excluded. Cronbach’s alpha was acceptable for each factor (α = 0.86, 0.87 and 0.76). Mean scores (and standard deviations) for each factor were 3.04 (0.77), 2.92 (0.91) and 3.00 (0.78).
Variables associated with respondent attitudes towards research
Examination of the scree plot indicated three to six attitudinal factors. For each model, Cronbach’s alpha was calculated and potential underlying concepts considered for all models. The 3-factor model gave the best fit, and is presented here. Attitudinal factor 1 related to research acceptability (items 13a-c and 13 e); factor A2 related to engagement and the impact/importance of research findings on nursing practice (items 13 n-13q); and factor A3 related to the experience of supporting research projects (items 13 d, 13f-g, 13i-k, 13 m and 13 r-s). Cronbach’s alpha was acceptable (α = 0.72, 0.82 and 0.72 respectively). Mean scores (and standard deviations) for each factor were 4.15 (0.56), 4.11 (0.52) and 3.32 (0.50).
Linear regression models.
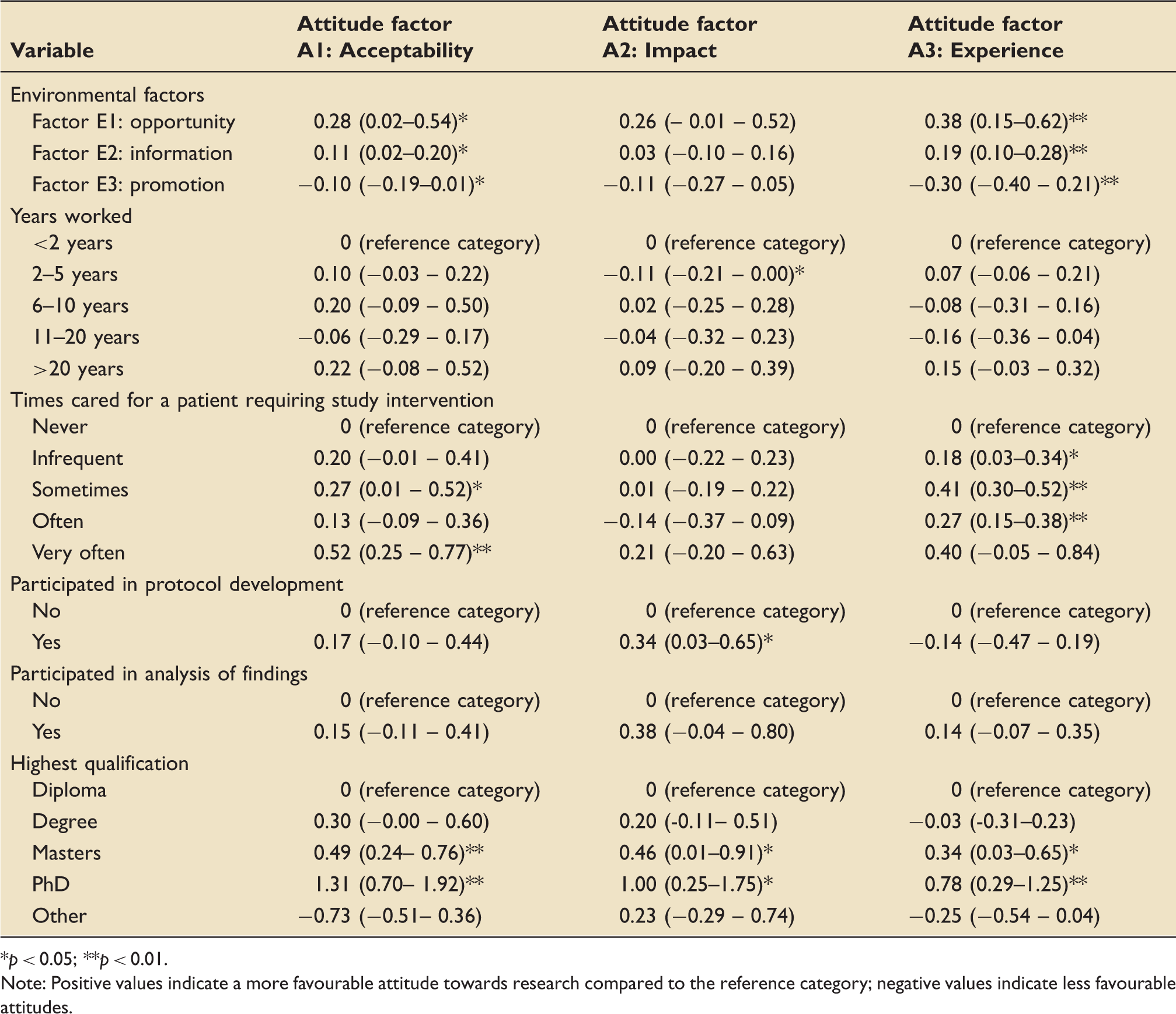
p < 0.05; **p < 0.01.
Note: Positive values indicate a more favourable attitude towards research compared to the reference category; negative values indicate less favourable attitudes.
Research acceptability (Attitude factor A1) was found to be associated with environmental factors opportunity (E1) (p = 0.035) and information (E2) (p = 0.026). It was negatively associated with environmental factor promotion (E3) (p = 0.039). Research acceptability (Attitude factor A1) was also associated with having cared for patients on study procedures (p = 0.044).
Impact of research findings (Attitude factor A2) was associated with two to five years working (p = 0.042), and having helped to develop a research protocol (p = 0.034).
Research experience (Attitude factor A3), was strongly positively associated with environment factors opportunity (E1) (p = 0.004), and information (E2) (p = 0.001), and strongly negatively associated with environmental factor promotion (E3) (p < 0.001). Research experience was also positively associated with caring for a patient needing study procedures; infrequently (p = 0.025), sometimes (p < 0.001), or Often (p < 0.001).
All three attitude factors were positively associated with having a Master’s degree (p(A1) = 0.001, p(A2) = 0.045, p(A3) = 0.034) or a PhD (p(A1) = 0.001, p(A2) = 0.013, p(A3) = 0.004).
Discussion
This is the first study that investigates the attitudes and experiences of both nurses and AHPs towards research, working in critical care. Previous studies have investigated one single profession.11,12 As in previous studies, the results demonstrate that critical care nurses and AHPs believe that research is an important part of patient care and leads to improved patient outcomes.11,12 They also demonstrate an understanding of the importance of research to their own professional role. The results support the findings of recent studies which demonstrated an enthusiasm and motivation of UK-based physiotherapists 11 and Canada-based nurses, 12 to participate in critical care research.
Our study demonstrated that low levels of research training had been undertaken by participants. Furthermore, only a third of respondents reported being actively encouraged to participate in research by their management, even though opportunities were available in their hospitals. These are two areas which could be addressed in order to improve involvement in critical care research in Wales.
A collaborative relationship between research teams and clinicians was reported in this study; however, communication regarding study progression and findings needs improvement. Therefore, one potential method of improving staff research engagement in critical care across Wales would be to improve communication. Previous studies have reported strategies that could be employed to address this, such as the use of research champions and attendance at local research meetings.15,16 A key aim of the Welsh Government’s Critically Ill Delivery Plan (2018) was to develop clinical leaders in research and support them with appropriate academic infrastructure. 7 Achieving this aim could improve communication on individual ICUs.
Linear regression models indicate that a higher level of formal education was associated with a more positive view of research across all attitude factors. This could be explained by the inclusion of research methods modules within postgraduate courses, undertaken by the respondents. The different proportion of nurse and AHP respondents, however, may have influenced the study findings, as the undergraduate course contents differ across the professions.
The recognition and opportunities for involvement and information environmental factors were positively associated with the acceptability of research and experience of caring attitude factors, and the attitude of other research staff environmental factor was negatively associated with them. The use of research champions on each unit and encouraging attendance at research meetings could address this on a national level.
A number of differences were found in this study, compared to the Canadian study, primarily related to the involvement and understanding in research procedures. The respondents in this study had participated markedly fewer times in the last 12 months in any research-related activity, compared to the Canadian study. 12 This suggests that at present, there is less opportunity to participate in critical care research in Wales. This was evident when comparing the mean number of active research studies at each site, which was 12 in the Canadian study, compared to two active research studies per site in Wales. The difference could also be explained by the fact that in Wales most research-related activities are currently undertaken by the dedicated research nurses. The number of dedicated research nurses in the largest hospital in Wales was seven, as compared to 1.75 in the Canadian study, and almost one-third of respondents in this study were employed at that hospital.
Twice as many respondents in the Canadian study, had completed a course in research design, compared to this study, even though understanding of research-related activities was similar. 12 Furthermore, twice as many respondents reported being actively encouraged by their managers to participate in research in the Canadian study as in this study, which may suggest a change in culture, or education of managerial staff is required in Wales. Physicians were most frequently reported to lead research activity, so it may be necessary to target nurses and AHPs, when developing strategies for promoting new principal investigators. This could include releasing nursing and AHP staff from clinical duties, in order to work alongside the research-active physicians for a period of time, prior to becoming independent leads of studies. Similarly, attendance at research-related meetings was very low, so making meetings more accessible to clinical staff could be a straightforward strategy, to improve knowledge of research and communication regarding studies.
Strengths of our study include the inclusion of 13 of the 14 ICUs in Wales, the response rate achieved and the inclusion of nursing and all AHP professions. The inclusion of all ICUs ensured that the views of both research-active and non-research active sites were considered, thus facilitating more generalisable strategies for improved engagement. The questionnaire used in the study had been previously designed and implemented and was specific to the research question we were attempting to address. Our results are not generalisable to specialty-specific units, however, as we only included general ICUs and excluded paediatric, burns and cardiothoracic units. Finally, as with any self-reported questionnaire study, the results may be influenced by a number of forms of bias and this should be considered when interpreting the study findings. Another limitation was the lack of involvement of one of the units in Wales due to lack of Principal Investigator engagement. As this site is less research active, the omission of their clinicians’ survey responses will have impacted the results of our study.
Our study demonstrates that nurses and AHPs in Wales are generally supportive of critical care research, and there is a need for improved research-related education at undergraduate level for these professions. Communication between research teams and clinicians is a key area of potential improvement in engagement, and the development of local strategies such as the introduction of research champions and attendance at research meetings could prove beneficial. Critical care managers in Wales should actively encourage nurse and AHP participation in research activity.
Supplemental Material
sj-pdf-1-inc-10.1177_1751143720968659 - Supplemental material for Nurse and allied health professional experiences and attitudes toward critical care research: A national questionnaire study
Supplemental material, sj-pdf-1-inc-10.1177_1751143720968659 for Nurse and allied health professional experiences and attitudes toward critical care research: A national questionnaire study by Ceri Battle, Ceri Lynch, Timothy Discroll, Chris Thorpe, Bryony Hatchley, Sara Biggs, Rebecca Phillips, Alice Roberts, Sian Roberts, Jade Cole, Rhys Davies, Maria Hobrok, David Canning, Christopher Littler, Anwen Williams and Richard Pugh in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-2-inc-10.1177_1751143720968659 - Supplemental material for Nurse and allied health professional experiences and attitudes toward critical care research: A national questionnaire study
Supplemental material, sj-pdf-2-inc-10.1177_1751143720968659 for Nurse and allied health professional experiences and attitudes toward critical care research: A national questionnaire study by Ceri Battle, Ceri Lynch, Timothy Discroll, Chris Thorpe, Bryony Hatchley, Sara Biggs, Rebecca Phillips, Alice Roberts, Sian Roberts, Jade Cole, Rhys Davies, Maria Hobrok, David Canning, Christopher Littler, Anwen Williams and Richard Pugh in Journal of the Intensive Care Society
Footnotes
Acknowledgments
Individual members of WICSARG Chris Thorpe, Department of Anaesthetics and Intensive Care Medicine, Ysbyty Gwynedd, Bangor, UK; Bryony Hatchley, Physiotherapy Dept, Royal Gwent Hospital, Newport, UK; Sara Biggs, Physiotherapy Dept, Royal Gwent Hospital, Newport, UK; Rebecca Phillips, Physiotherapy Dept, Nevill Hall Hospital, Abergavenny, UK; Alice Roberts, Physiotherapy Dept, Glangwili General Hospital, Carmarthen, UK; Sian Roberts, Physiotherapy Dept, Princess of Wales Hospital, Bridgend, UK; Jade Cole, Intensive Care Unit, University Hospital Wales, Cardiff, UK; Rhys Davies, Intensive Care Unit, University Hospital Wales, Cardiff, UK; Maria Hobrok, Intensive Care Unit, Bronglais General Hospital, Aberystwyth, UK; David Canning, Physiotherapy Dept, Withybush General Hospital, Haverfordwest, Wales, UK; Chris Littler, Department of Anaesthetics, Wrexham Maelor Hospital, Wrexham, Wales, UK; Anwen Williams, Wrexham Maelor Hospital, Wrexham, Wales, UK.
Availability of data statement
Research data are available from the corresponding author on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
{kind=link}
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.