
Abstract
Introduction
Defining research priorities in intensive care is key to determining appropriate allocation of funding. Several topics were identified from the 2014 James Lind Alliance priority setting exercise conducted with the Intensive Care Society. The James Lind Alliance process included significant (and vital) patient/public contribution, but excluded professionals without a bedside role. As a result it may have failed to identify potential early-stage translational research topics, which are more likely identified by medical and/or academic members of relevant specialist basic science groups. The objective of the present project was to complement the James Lind Alliance project by generating an updated list of research priorities by facilitating academic research input.
Method
A survey was conducted by the National Institute for Health Research (NIHR) to identify the key research priorities from intensive care clinicians, including allied health professionals and academics, along with any evolving themes arising from translational research. Feasibility of all identified topics were then discussed and allocated to themes by a joint clinical academics/NIHR focus group.
Results
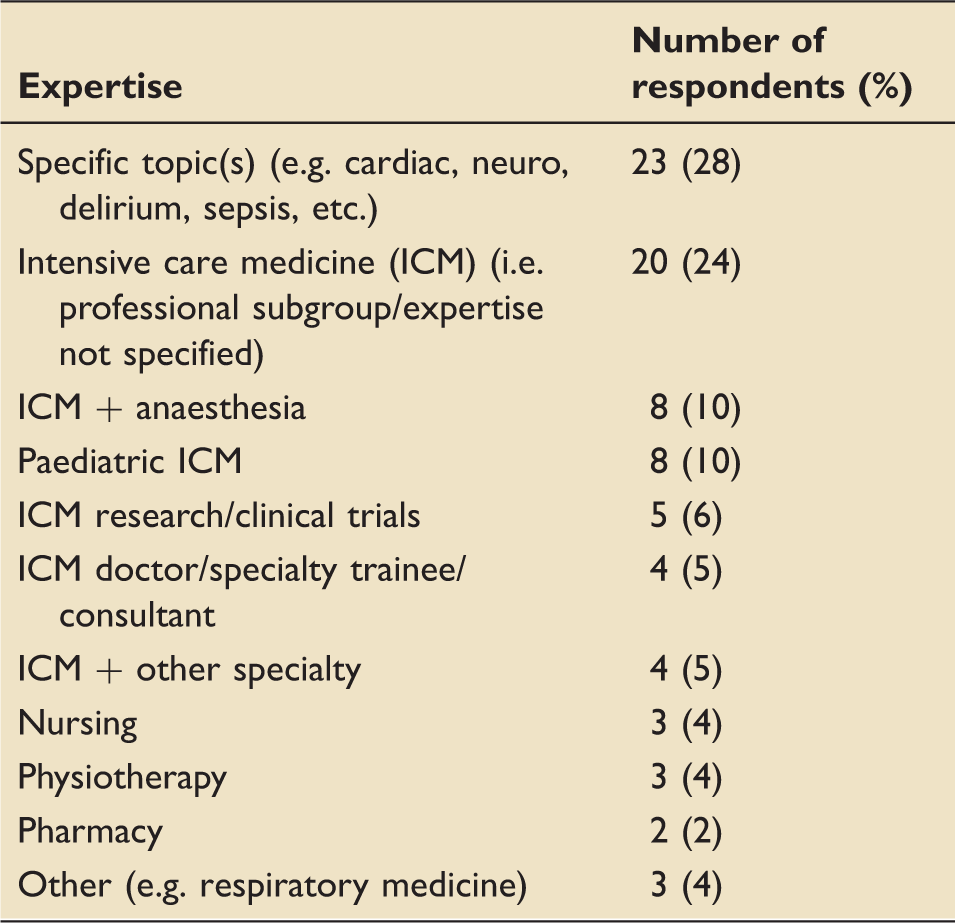
The survey was completed by 94 intensive care clinicians (including subspecialists), academics and allied health professions. In total, 203 research questions were identified, with the top five themes focusing on: appropriate case selection (e.g. who and when to treat; 24%), ventilation (7%), sepsis (6%), delirium (5%) and rehabilitation (5%).
Discussion
Utilising a methodology distinct from that employed by the James Lind Alliance process, from a broad spectrum of intensive care clinicians/scientists, enabled identification of a variety of priority research areas. These topics can now inform not only the investigator-led research agenda, but will also be considered in due course by the NIHR for potential future funding calls.
Introduction
For research funders, understanding the relative importance of particular topics as perceived by the clinical and academic communities along with, increasingly, the patient and wider public, is a key element in determining decision making around the commissioning of medical research. This is particularly important for funders distributing public money such as the National Institute for Health Research (NIHR). In 2013/2014, the UK Intensive Care Society, along with the James Lind Alliance (JLA), conducted a research priority setting partnership exercise that produced a list of uncertainties around treatment decisions for critically ill patients.1,2 This process identified the top three priorities for research, alongside a further eight unranked priorities where there was uncertainty around treatment strategies. This important piece of work has been influential in developing and supporting the intensive care research agenda subsequently. In addition, anaesthesia and perioperative care, a clinical area which overlaps with critical care, have undertaken similar exercises. 3
A key element of the JLA approach is the encouragement and participation of patients and family members with personal experience of the disease area in question. This is particularly challenging for highly technical areas such as intensive care and anaesthesia, especially as the patient may not have any memories of the acute disease or condition from which they were suffering following their recovery. Thus, the contribution of family members has proved very important.
In brief, the critical care JLA project was a modified Delphi process involving two survey rounds, followed by a focus group. 1 The first survey generated over twelve hundred individual suggestions from nearly five hundred participants. These suggestions were subsequently collated into a reduced number of research topics, more closely resembling research questions, and these were re-presented in a second round survey which was intended to allow participants to rank the importance of the topics identified. The subsequent focus group consisting of professionals, patients and carers was used to generate the final list. The process itself, although extensive, did have some limitations to it. Firstly, contributing professionals had to have a bedside caring role, thus colleagues with a full-time academic role were excluded. Secondly, the proportions of individuals by professional background or patient and carer status were not controlled and there were a greater proportion of patients and carers at the final focus group. This is part of the JLA methodology, but as a result there is a risk that the process can become focused on current clinical issues, rather than identifying promising interventions at an early translational stage or opportunities to improve understanding of the mechanism of disease. While such a bedside clinician and patient-led approach is undoubtedly important, from a funder’s perspective this does leave a gap in terms of identifying potential opportunities that are at an earlier stage of the research continuum.
In May 2017, the NIHR ran a research prioritisation exercise in Trauma from which a number of intensive care questions emerged. This, alongside intensive care questions that had been emerging from other sources, prompted the NIHR to consider refreshing their understanding of what the current research priorities might be for the intensive care community. Thus, the objective of the project described in this paper was to generate an updated list of research priorities to complement the JLA project. The intention was not to repeat the JLA process. In addition, and recognising that the JLA project had some limitations, a secondary objective was also to explore whether there were any key emerging themes from translational research work which should be included.
Methods
The method adopted was a single round survey conducted by the National Institute for Health Research. Topics were screened and those that were considered to be within the scope of the exercise (i.e. those within the remit of the relevant funding programmes managed by the NIHR Evaluation, Trials and Studies Coordinating Centre (NETSCC): Efficacy & Mechanism Evaluation (EME), Health Technology Assessment (HTA) or Health Services & Delivery Research (HS&DR)) and a valid research question (specific to critical care), were batched into themes and indicative questions.
This was followed by a teleconference involving a small clinical academic group and members of the NETSCC team to discuss the feasibility of the ideas raised. The survey did not use National Health Service (NHS) mechanisms, nor seek the views of patients or family members, and thus there was no requirement for governance review. Consent to participate was assumed from participation.
The survey instrument (SurveyMonkey Inc, San Mateo, California, USA, www.surveymonkey.com; online Appendix A) was generated after initial conversations with representatives from the intensive care community and was based around the generic question; ‘What is the most important unanswered clinical or service delivery question in critical care you think that needs to be answered?’ Participants were given the option of developing their question with the ‘PICO' format (Patient population, Intervention, Comparator, Outcomes) and to provide justification for the importance of their submitted topic. Individuals were allowed to make three suggestions on the initial survey form, but could, if they wished, generate further suggestions.
An invitation to participate in the survey was sent on behalf of the NIHR by The Intensive Care Society, The Faculty of Intensive Care, The Paediatric Intensive Care Society, The Intensive Care National Audit and Research Centre and the NIHR Clinical Research Network Critical Care National Specialty Group. Only topics relating to the adult critical care population are discussed in this paper.
The survey itself opened in mid-November 2017 with a planned closing date of 20 December 2017 which was subsequently extended to 15 January 2018 to allow for people to contribute who had been away over the holiday period.
Results
Expertise of respondents.
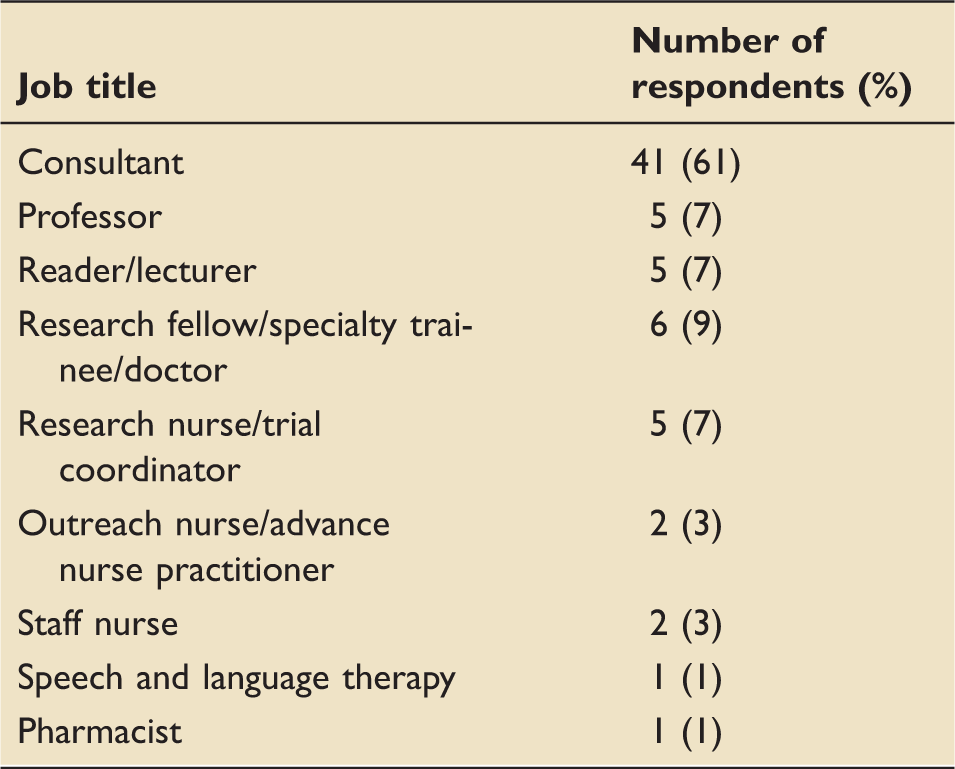
Job titles of respondents.
Themes and indicative questions raised.
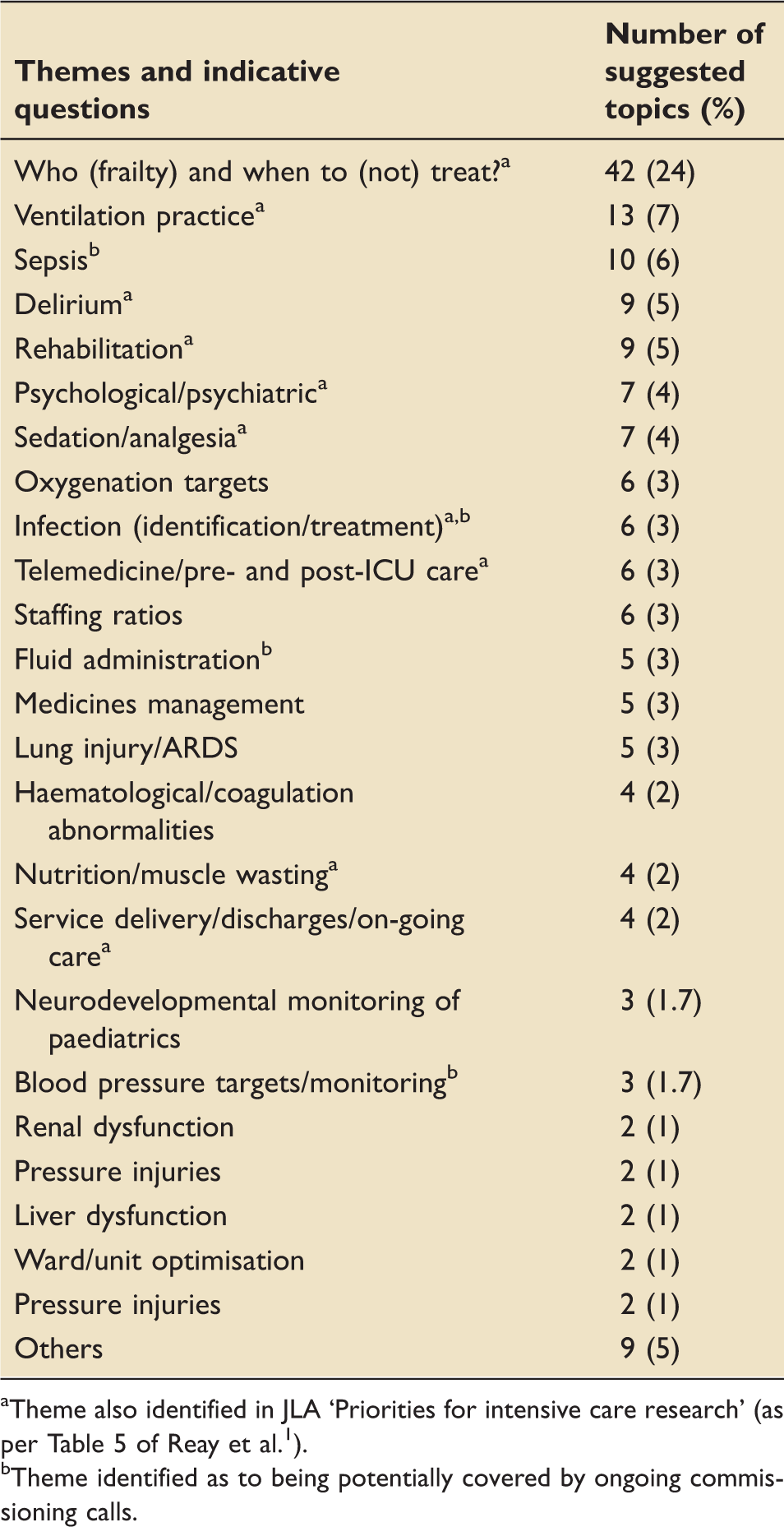
Theme also identified in JLA ‘Priorities for intensive care research' (as per Table 5 of Reay et al. 1 ).
Theme identified as to being potentially covered by ongoing commissioning calls.
The subsequent teleconference identified areas with potential overlap with current NIHR commissioned calls (marked with ‘b’ in Table 3). In addition, the most appropriate NIHR funding programme for a given topic was discussed. Areas where the topics might be challenging to deliver, and where an evidence synthesis, a pilot clinical trial or a definitive clinical trial might be most appropriate to commission were also discussed. No topic was removed from consideration on the basis of the focus group discussion.
Discussion
This exercise has highlighted a number of potential priority areas, which funders such as the NIHR and the Medical Research Council may choose to adopt, using a distinct methodology to that utilised by the recent JLA Intensive Care Priority Setting Partnership. Moreover, information was gathered from a broad cross section of the intensive care medical, research and allied health professional communities, in addition to the variety of personal subspecialty expertise. Including patients and the public in this process, in a meaningful way, was therefore not possible.
A large proportion of questions proposed related to ascertaining likely futility of treatment, the validity of using frailty as a proxy measure for this and thus guiding when initiation of palliative care might be appropriate. Ventilation practice questions were also frequent, relating to ventilator-associated pneumonia prevention, to airway pressure release ventilation use and weaning strategies as well as the use of mucolytic agents. Delirium was again a common theme, with calls to develop novel interventions to reduce its incidence and improve management and thus associated long-term outcomes. Other themes, namely sepsis, identification/treatment of infection and fluid management topics are likely to be covered by the recent NIHR broad briefs for sepsis and antimicrobial resistance themed calls. Fewer than half of the themes identified by this process, overlapped with those identified in the JLA process (marked with ‘a’ in Table 3)
This project has limitations; the response was modest in spite of the effort to disseminate widely, and the responses remain dominated by clinical issues, similar to the earlier JLA project. It was noted that a significant proportion of the responses came from senior clinicians, which may be representative of the membership of the intensive care networks through which it was distributed. This was in contrast to the JLA process where 31% of professional respondents were doctors (of which 68% were consultant-grade). 2 Early phase translational opportunities did not seem to emerge. It is possible efforts to reach all groups (especially basic science colleagues) did not work, the community felt it had little further to contribute or that early translational work had not yet reached the consciousness of the community in a way that lent itself to representation in projects such as this. The project did deliver as a ‘sense-check' for identifying current clinical concerns; a thorough identification of early translation opportunities is clearly challenging and does not seem to lend itself to this type of approach.
All of the topics resulting from this survey will be considered in due course and may be taken forward by one of the NIHR funding programmes as commissioned funding calls. This process would involve further development and prioritisation of the topics by NIHR Prioritisation Committees with input from both the Intensive Care community and patient and public contributors through a process of peer review.
Undoubtedly, regardless of potential future NIHR calls, many of the topics raised would still benefit from investigator-led research.
Teleconference focus group
Stephen Brett (Imperial College): Intensivist, JLA PSP Daniele Bryden (Sheffield): Intensivist, HTA Prioritisation Committee member Peter Watkinson (Oxford): Intensivist, HTA Prioritisation Committee member Barney Scholefield (Birmingham): Paediatric intensivist Danny McAuley (Belfast): Intensivist, HTA Funding Committee member Mark Borthwick (Oxford): Critical Care Pharmacist
Supplemental Material
Supplemental Material1 - Supplemental material for The National Institute for Health Research Critical Care Research Priority Setting Survey 2018
Supplemental material, Supplemental Material1 for The National Institute for Health Research Critical Care Research Priority Setting Survey 2018 by Kate C Tatham, Daniel F McAuley, Mark Borthwick, Neil G Henderson, Gemma Bashevoy and Stephen J Brett in Journal of the Intensive Care Society
Supplemental Material
Supplemental Material2 - Supplemental material for The National Institute for Health Research Critical Care Research Priority Setting Survey 2018
Supplemental material, Supplemental Material2 for The National Institute for Health Research Critical Care Research Priority Setting Survey 2018 by Kate C Tatham, Daniel F McAuley, Mark Borthwick, Neil G Henderson, Gemma Bashevoy and Stephen J Brett in Journal of the Intensive Care Society
Supplemental Material
Supplemental Material3 - Supplemental material for The National Institute for Health Research Critical Care Research Priority Setting Survey 2018
Supplemental material, Supplemental Material3 for The National Institute for Health Research Critical Care Research Priority Setting Survey 2018 by Kate C Tatham, Daniel F McAuley, Mark Borthwick, Neil G Henderson, Gemma Bashevoy and Stephen J Brett in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.