
Abstract
Purpose
To identify outcome measurement tools used to evaluate communication, voice and speech intelligibility in the mechanically ventilated ICU population. Secondly, to evaluate, synthesise and compare the clinimetric properties of the tools identified.
Materials and methods
A systematic review of articles was undertaken via electronic databases in two parts. Eligibility criteria for selection: part one – quantitative or mixed methods studies which assessed communication, voice or speech intelligibility; part two – studies which evaluated a clinimetric property for one of the tools identified in part one. Two independent reviewers assessed articles for inclusion and used the consensus-based standards for health status measurement instruments (COSMIN) risk of bias checklist.
Results
The part one search yielded five included studies comprised of eight outcome measurement tools. The part two search yielded 22 included studies comprised of nine tools. Few studies had adequate reliability and measurement error properties. No studies established responsiveness. A notable proportion of studies utilised tools that have no clinimetric properties.
Conclusions
There is a relatively small number of studies which have established clinimetric properties for outcome measurement tools that evaluate communication, voice and/or speech intelligibility, and a fewer number which have done so in the mechanically ventilated ICU population.
Introduction
Critically ill patients experience impaired communication, usually due to the presence of an endotracheal tube or tracheostomy tube. About one-third of intensive care unit (ICU) patients experience difficulty communicating 1 and half of the mechanically ventilated patients in ICU meet minimum criteria for communication during sustained periods of wakefulness. 2 Communication interventions have the potential to enable patients to not only express their basic wants and needs, but also to engage in conversations with their loved ones and with health care professionals about their care, such as, consent for procedures and withdrawal of care which is an unfortunate reality of a proportion of ICU admissions. A range of communication interventions have been studied in this population, including communication board, electrolarynx, high-technology augmentative and alternative communication (AAC) device, one-way valve in-line with the ventilator and ventilator-adjusted leak speech (VALS).3–5 A recent systematic review of the feasibility, utility and safety of communication interventions with mechanically ventilated ICU patients found that while the level of evidence is generally low, there is a promising signal that communication interventions are feasible, have utility and are safe to perform in this population.3. However, of the 48 included studies, there was heterogeneity relating to the communication intervention and the outcome measurement tool used. The majority of studies measured outcomes using perceptual or subjective judgements. 3 Higher quality studies are required to establish how best to provide intervention with critically ill patients who are usually voiceless, and need speech pathology intervention to facilitate communication and participation in their healthcare.
Use of outcome measurement tools with established clinimetric properties, such as validity and reliability, is favourable over subjective clinical judgements. A reliable and valid tool facilitates accurate, reproducible and specific measurement of a desired outcome. The utilization of outcome measurement tools in healthcare is essential, for patients, clinicians and health services alike – to identify which interventions are beneficial, which are not, to improve clinical outcomes as well as service delivery and appropriate resource management. 6 For clinicians, an assessment of the quality of outcome measurement tools available provides guidance as to the most reliable and responsive to determine efficacy, progress and utility of given interventions. This is beneficial first and foremost for patients, and additionally for the demonstration of the value-add of speech pathology in the ICU setting.
The communication needs of ICU patients are subject to change in a high-acuity setting, associated with their medical instability and illness severity. Factors such as fluctuating alertness and requirement for sedation, ICU-acquired weakness, fatigue and cognitive profile influence the choice and timing of particular therapeutic interventions. In the absence of objective outcome measurement tools, currently, clinicians, researchers and patients have limited knowledge of which therapeutic interventions add value, minimise deterioration or restore function.
The aims of this systematic review were two-fold: (1) to identify the outcome measurement tools utilised in studies of critically ill mechanically ventilated adults which evaluated communication function and/or speech intelligibility and (2) to evaluate the clinimetric properties of the outcome measurement tools identified in part one.
Materials and methods
Protocol
The review was registered on PROSPERO (CRD42019136852). The search for this systematic review was conducted in two parts. Part one involved the identification of outcome measurement tools which have been used to evaluate communication, voice or speech intelligibility in the mechanically ventilated ICU population. Part two involved a second search to identify studies that examined the clinimetric properties of the measurement tools identified in part one. The review design was consistent with earlier published work in the ICU setting. 7
Part one – Identification of measures
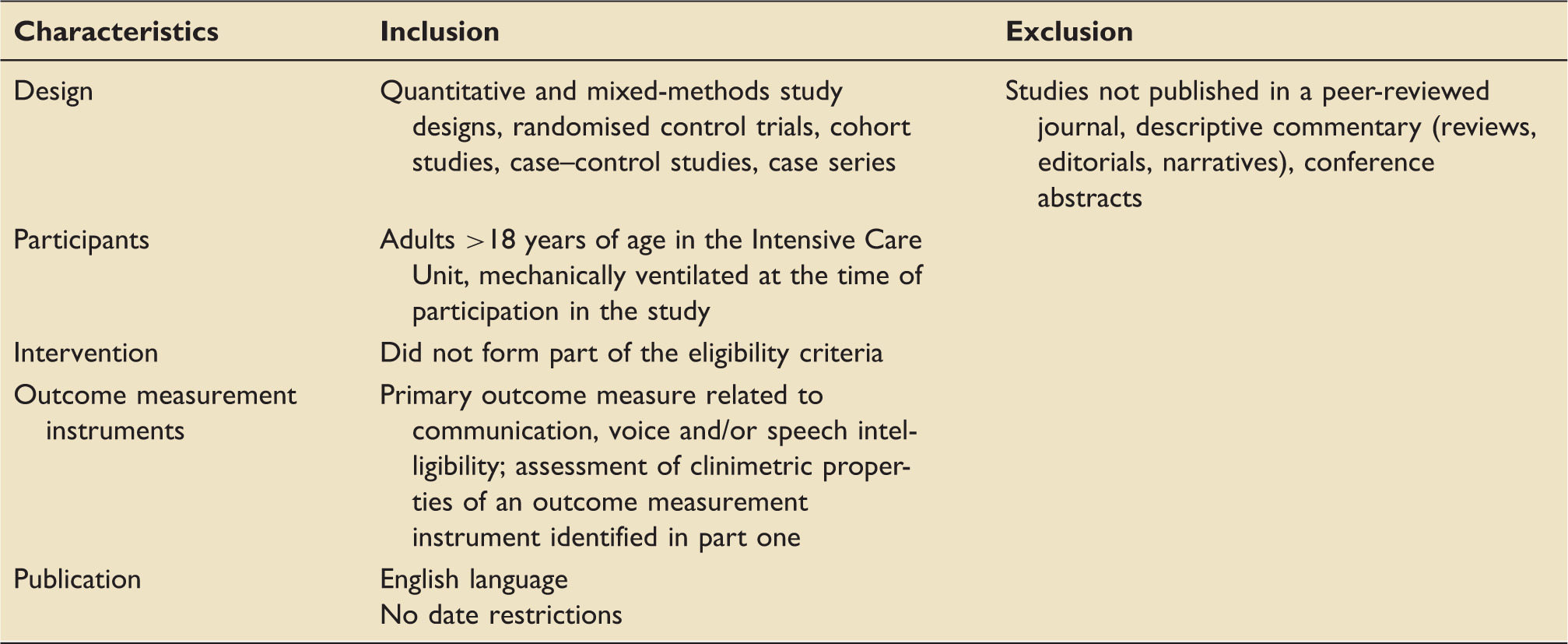
Part one: pre-determined inclusion and exclusion criteria.
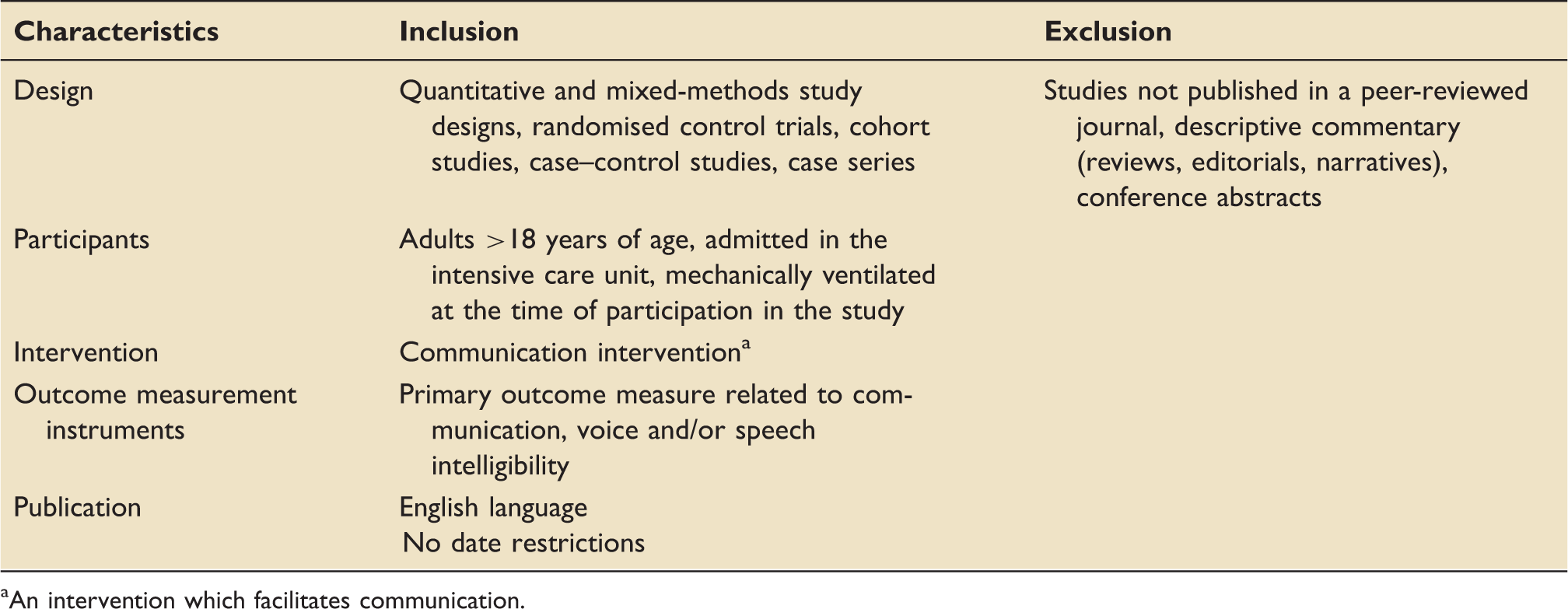
An intervention which facilitates communication.
Part two – Clinimetric properties of outcome measurement tools
Medline, Embase, CINAHL and Web of Science electronic databases were searched by one reviewer using a systematic, comprehensive and reproducible search strategy, devised with the assistance of a professional university librarian (see Supplementary Figure 2) with the last search run on 25 July 2019. The study selection and data extraction followed the same methodology described for part one. Two independent reviewers used relevant items of the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) risk of bias checklist to evaluate the methodological quality and risk of bias of the included studies. The COSMIN checklist is a standardised tool for assessing the individual studies on measurement properties of Patient Reported Outcome Measures (PROMs). 8 Since its original development, the COSMIN checklist was revised for use in systematic reviews of PROMs seeking to assess risk of bias of studies on measurement properties. 9 The COSMIN comprised a box for each measurement property which contains standards to assess the quality of a study on that specific measurement property, of which a score is derived. 8
Since this systematic review investigated clinician-reported outcome measures, not patient-reported outcome measures, reliability, measurement error, hypothesis testing, criterion validity and responsiveness were the relevant items of the checklist. An overall quality score for each item was obtained by using the lowest score recorded. 9 Agreement between the two reviewers was estimated using percentage agreement and the kappa statistic. 10
Results
Part one – Identification of outcome measurement tools
Studies which met inclusion criteria.
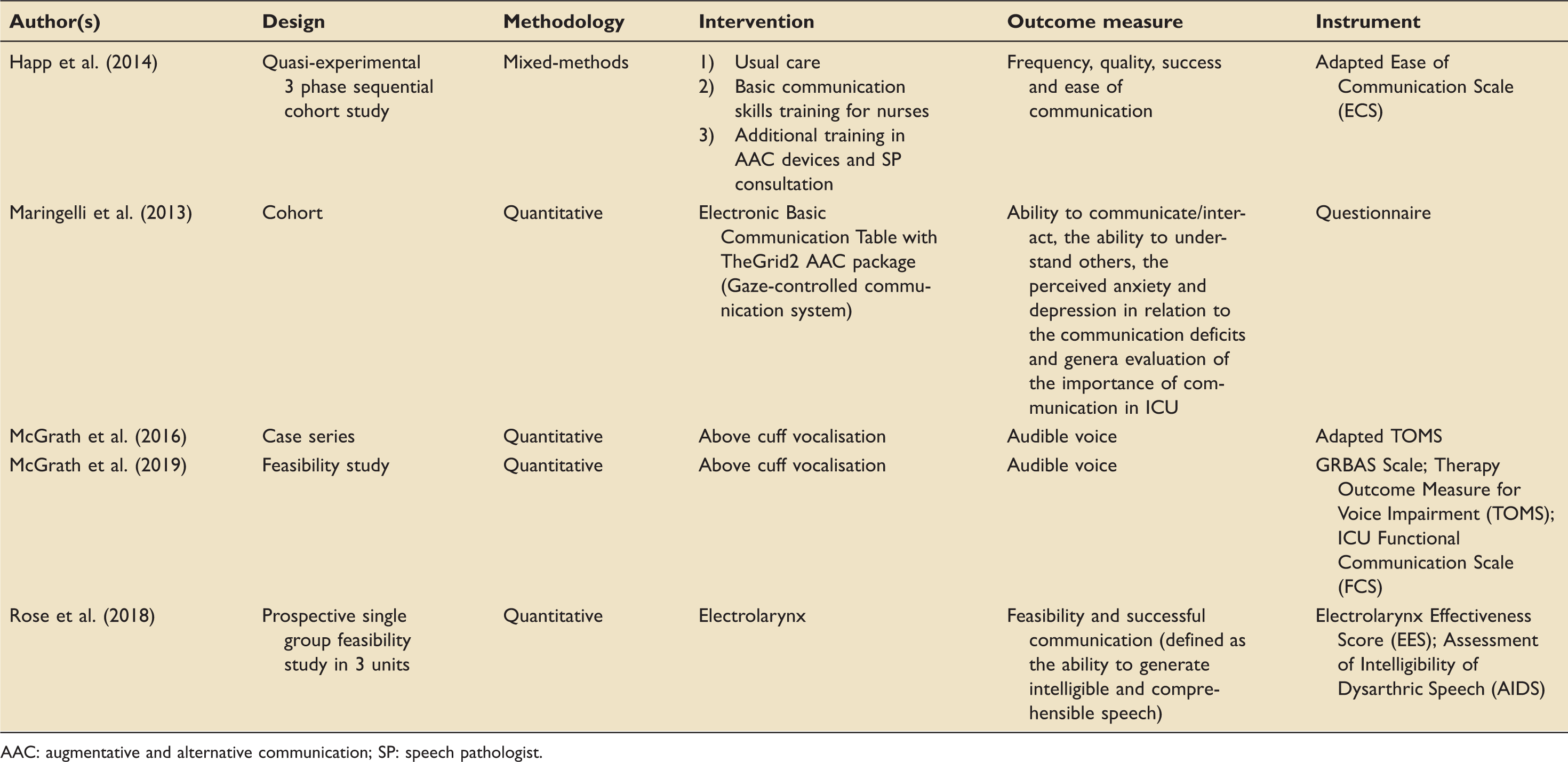
AAC: augmentative and alternative communication; SP: speech pathologist.
Part two – Clinimetric properties of outcome measurement tools
Study selection and study characteristics
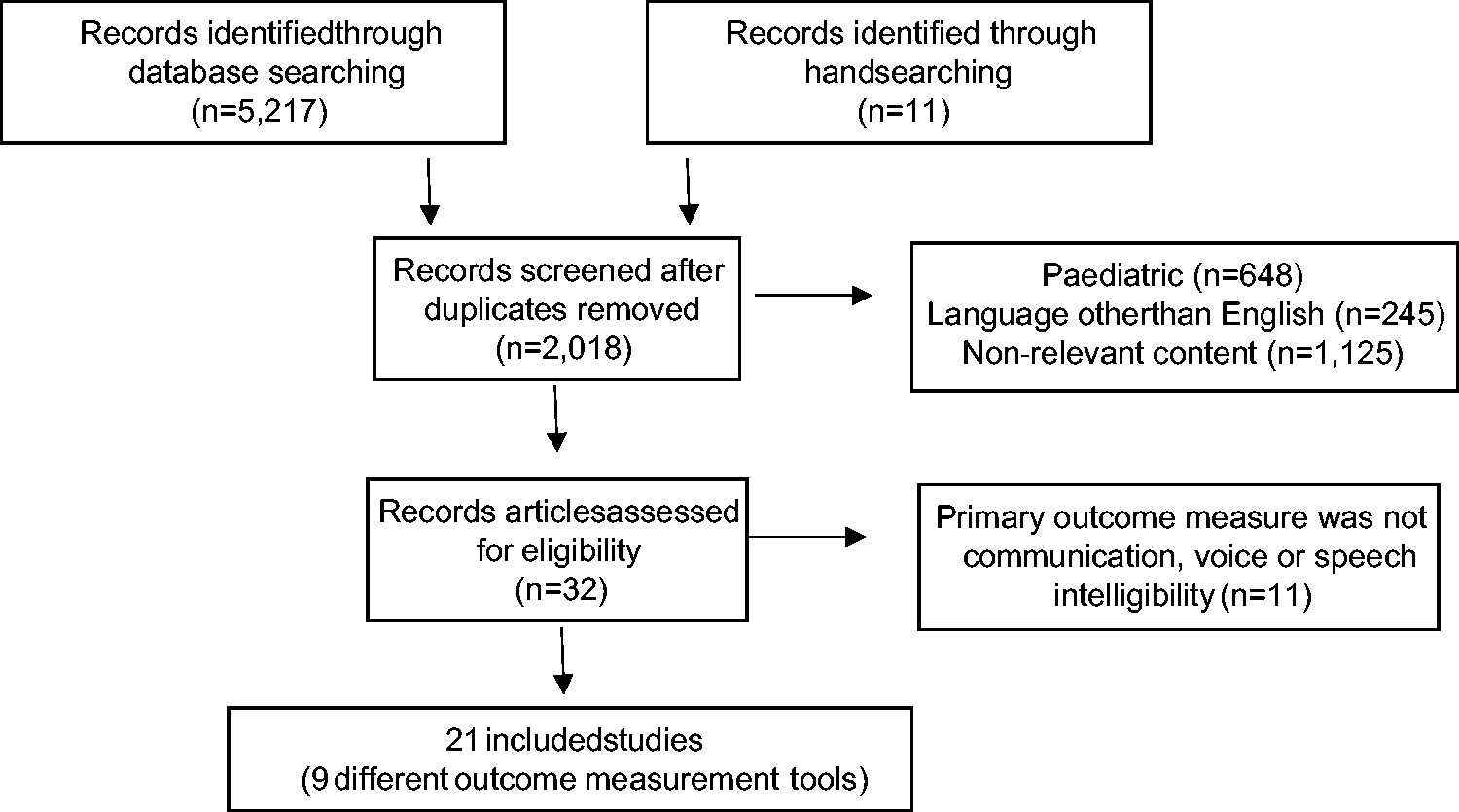
The aim of this second search was to yield relevant articles which examined the clinimetric properties of the outcome measurement tools that were identified in the part one search. As such, the search terms for part two were only devised at the completion of the part one review. The first iteration of this search did not yield any relevant full-text articles. The search strategy was subsequently revised to specifically include the outcome measurement tools identified in part one, as keyword phrases. This second iteration of the search yielded 5217 records (see Figure 2). Twenty-two studies met the inclusion criteria (Table 3), including nine outcome measurement instruments which included the GRBAS13,18–28 (n = 12), TOM
29
(n = 1), TOM-AAC
30
(n = 1), The Clinician Interview-Based Impression (CIBI)
31
(n = 1), Loewenstein Communication Scale (LCS)
32
(n = 1), Questionnaire
17
(n = 1), AIDS15,33,34 (n = 3), ICU-FCS
13
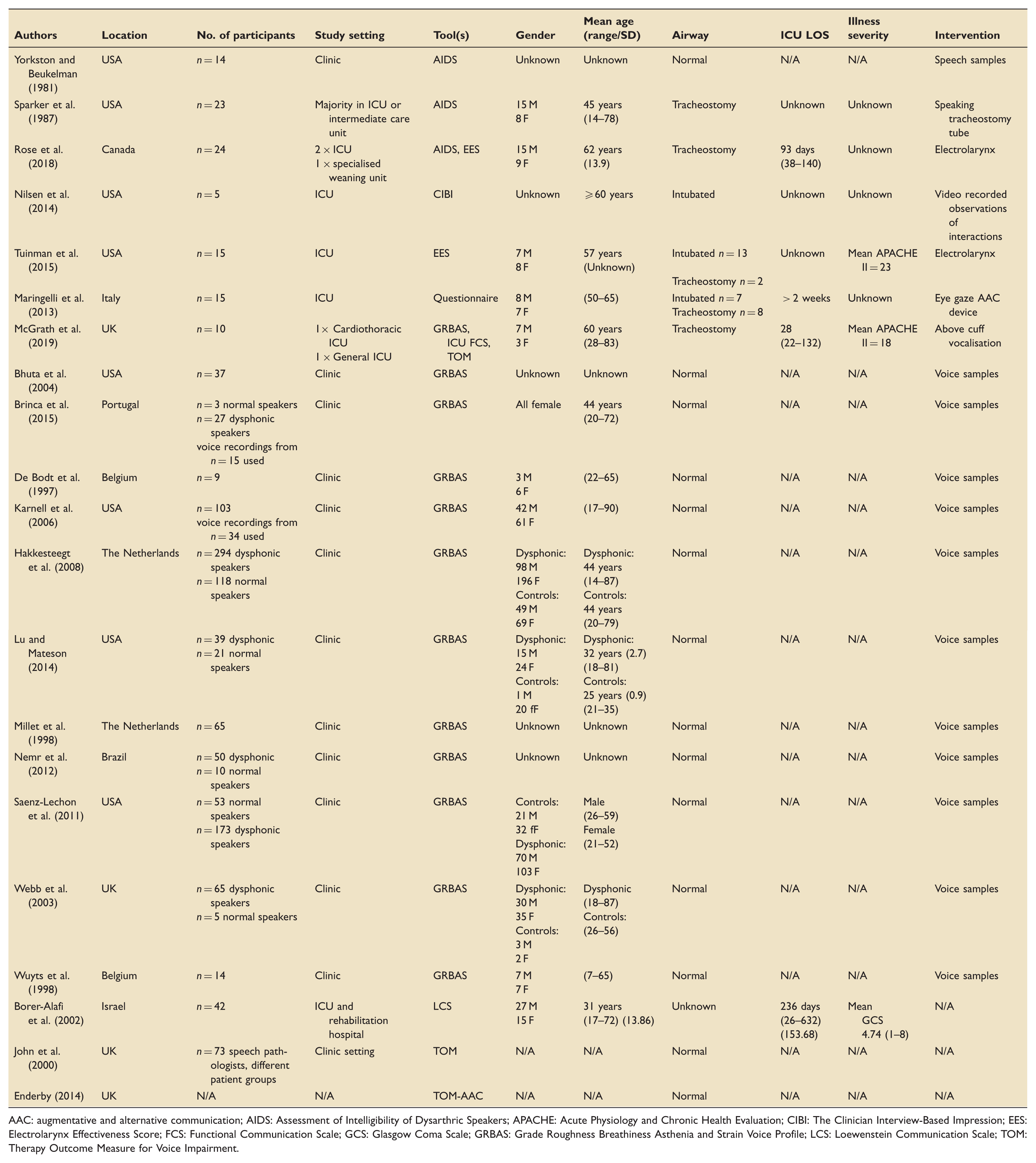
(n = 1) and EES15,16 (n = 2). Percentage agreement for title and abstracts 90% (κ = 0.78) and full-text 100% (κ = 1). The characteristics of the included studies are summarised in Table 4.
Part one: PRISMA diagram. PRISMA: preferred reporting items for systematic reviews and meta-analyses. Part two: PRISMA diagram. PRISMA: preferred reporting items for systematic reviews and meta-analyses. Part two: pre-determined inclusion and exclusion criteria. Part two: characteristics of included studies. AAC: augmentative and alternative communication; AIDS: Assessment of Intelligibility of Dysarthric Speakers; APACHE: Acute Physiology and Chronic Health Evaluation; CIBI: The Clinician Interview-Based Impression; EES: Electrolarynx Effectiveness Score; FCS: Functional Communication Scale; GCS: Glasgow Coma Scale; GRBAS: Grade Roughness Breathiness Asthenia and Strain Voice Profile; LCS: Loewenstein Communication Scale; TOM: Therapy Outcome Measure for Voice Impairment.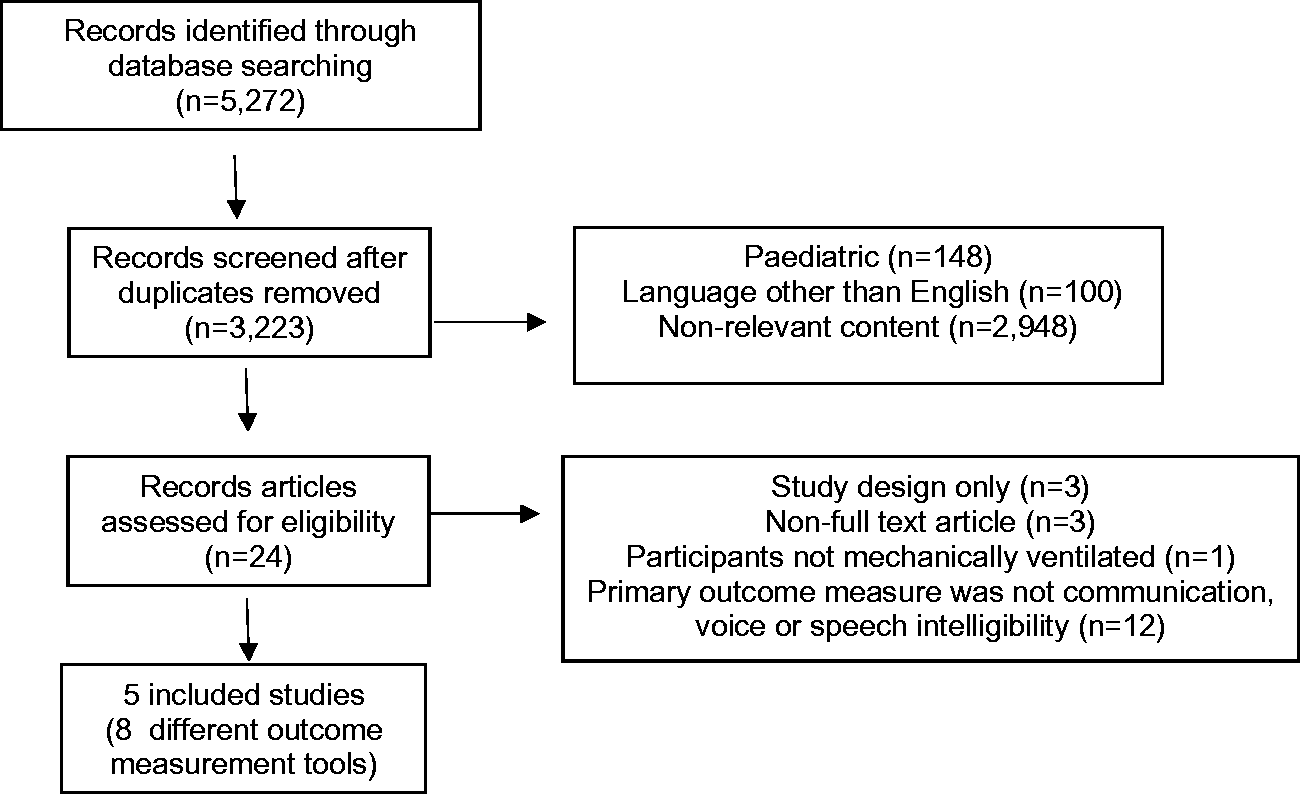
Risk of bias results
Percentage agreement for risk of bias assessment of included studies was 98% (κ = 0.823).
Synthesised evaluation of clinimetric properties of outcome measurement tools.
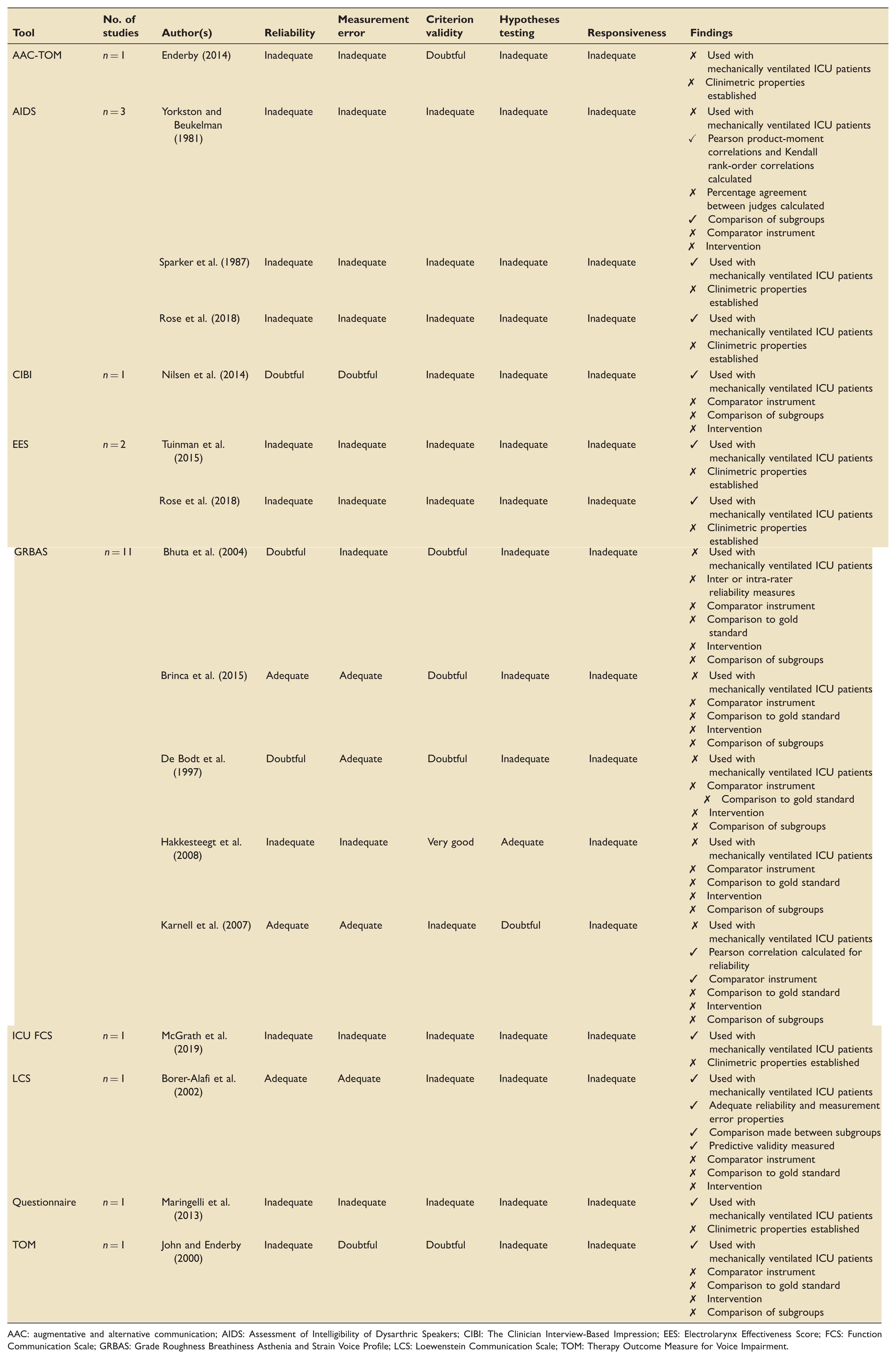
AAC: augmentative and alternative communication; AIDS: Assessment of Intelligibility of Dysarthric Speakers; CIBI: The Clinician Interview-Based Impression; EES: Electrolarynx Effectiveness Score; FCS: Functional Communication Scale; GRBAS: Grade Roughness Breathiness Asthenia and Strain Voice Profile; LCS: Loewenstein Communication Scale; TOM: Therapy Outcome Measure for Voice Impairment.
Discussion
Part one of this systematic review identified just five studies in which communication was a primary outcome. The main finding of part two was that the majority of the identified outcome measurement tools either do not have established clinimetric properties or have not been examined in the critical ill population who have an artificial airway. To the authors knowledge, this is the first systematic review which has examined the clinimetric properties of outcome measurement tools used to measure communication, voice and speech intelligibility in the ICU. As such, comparison with earlier work is not possible.
While currently without the examination of clinimetric properties, the ICU-FCS appears promising as an outcome measurement instrument for the verbal ICU patient, whether phonation be achieved by above cuff vocalisation,13,14 VALS35,36 or one-way valve in-line with the ventilator.37,38 The LCS was studied in patients who suffered traumatic brain injury in order to differentiate minimally responsive patients from those in a vegetative state. The LCS was found to have ‘adequate’ reliability and measurement error according to the risk of bias assessment, and the LCS scores generated were found to predict individual communication rehabilitation potential (p = 0.002) which indicates a strong signal. The generalisability of this tool in conscious patients without traumatic brain injury or neurological impairment is currently unknown. The included studies identified outcome measurement tools with sound clinical bases; however, very little is known about their properties and this suggests questionable accuracy of their use in this population overall. Establishing clinimetric properties of an outcome measurement tool are essential, to ensure that the results of measurement are accurate, reproducible and consistent.
The strength of this review was the systematic and reproducible search strategy which was devised in conjunction with a senior academic librarian from the University of Melbourne. No limits were applied to the publication date within the search which enabled relevant articles to be included as early as 1981. The data extraction process and the utilisation of a high-quality risk of bias assessment tool which have been applied to other reviews of tools in the ICU setting. 7 While every effort was taken to maintain the scientific rigour of this systematic review, search strategy was limited to English only and as a result some articles may have been missed. The COSMIN risk of bias checklist dictates users to rate the overall quality based on the lowest score and, there may be instances where tools were underrated as a result. Lastly, the authors did not attempt to contact authors of the included studies for missing data or clarification thereof, which may have contributed to the risk of bias checklist scoring.
Recommended future directions are three-fold: (1) to establish clinimetric properties for outcome measurement tools that currently lack these, e.g. ICU-FCS (2) to adapt and examine outcome measurement tools in the ICU population, e.g. GRBAS or (3) develop an outcome measurement tool that has robust clinimetric properties and considers the ICU environment and critically ill population. A reliable and sensitive tool would facilitate accurate measurement of the efficacy of speech pathology interventions in the critically ill and drive improvement in clinical outcomes in this highly vulnerable population.
Conclusion
This systematic review found few outcome measurement tools that have been used to assess communication outcomes with mechanically ventilated patients in ICU. Furthermore, the quality of these tools in the ICU setting has not been widely established. The adaptation and examination of existing tools in the ICU setting or the development and testing of a comprehensive outcome measurement tool evaluating communication, speech intelligibility or voice of critically ill patients would be beneficial for patients, clinicians and researchers.
Supplemental Material
sj-pdf-1-inc-10.1177_1751143720963757 - Supplemental material for Outcome measurement tools for communication, voice and speech intelligibility in the ICU and their clinimetric properties: A systematic review
Supplemental material, sj-pdf-1-inc-10.1177_1751143720963757 for Outcome measurement tools for communication, voice and speech intelligibility in the ICU and their clinimetric properties: A systematic review by Charissa J Zaga, Bridie Cigognini, Adam P Vogel and Sue Berney in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-2-inc-10.1177_1751143720963757 - Supplemental material for Outcome measurement tools for communication, voice and speech intelligibility in the ICU and their clinimetric properties: A systematic review
Supplemental material, sj-pdf-2-inc-10.1177_1751143720963757 for Outcome measurement tools for communication, voice and speech intelligibility in the ICU and their clinimetric properties: A systematic review by Charissa J Zaga, Bridie Cigognini, Adam P Vogel and Sue Berney in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for the article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.