
Abstract
More patients are discharged directly to home (DDH) after intensive care admission. This single-centre study compared admission characteristics, length of stay and discharge outcomes of DDH patients after mechanical ventilation, compared to patients discharged to wards (DW). Of 161 eligible patients, 32.9% were DDH and 68.1% were DW. DDH patients were significantly younger with lower APACHE II scores. They were ventilated for a shorter length of time, and overall length of stay was 7 days shorter. Physical function scores (CPAx) were significantly higher in DDH. There were no differences in re-admission or 90-day mortality. In certain patients, discharge direct to home may be a safe option.
Introduction
The practice of discharging patients directly to home (DDH) from intensive care units (ICU) is increasing worldwide. 1 There are a number of factors contributing to this, including increased demand for intensive care beds and decreased availability of ward beds across hospitals. 2
DDH has been suggested to be safe in selected patients, with low rates of mortality and hospital readmission.2 –4 Whilst satisfaction with DDH is high amongst patients and their families, there is still dissatisfaction amongst ICU clinicians. 1
The aim of this single-centre retrospective study was to identify the percentage of patients discharged directly home after mechanical ventilation, and to compare their admission characteristics, length of stay parameters and discharge outcomes, to patients discharged to the ward.
Methods
Fully anonymised data was provided from Warrington Hospital’s Digital Analytics Department after local approvals (reference WHHSE0242). Inclusion criteria were any mechanically ventilated patient admitted to Warrington Hospital’s intensive care unit, during an 18 month period from 1st January 2022 to 1st August 2023. Patients were placed into groups based on discharge status (see Figure 1). Patient admission characteristics (age, sex and APACHE II score), length of stay outcomes, mortality and re-admission status between DDH and DW patients were compared. In a smaller group of patients, physical function (Chelsea Critical Care Physical Assessment Tool, CPAx score) was also assessed. Between group comparisons were performed using Mann-Whitney U-tests, Chi-squared tests or Fisher’s exact test where appropriate, with a p-value <0.05 considered statistically significant.
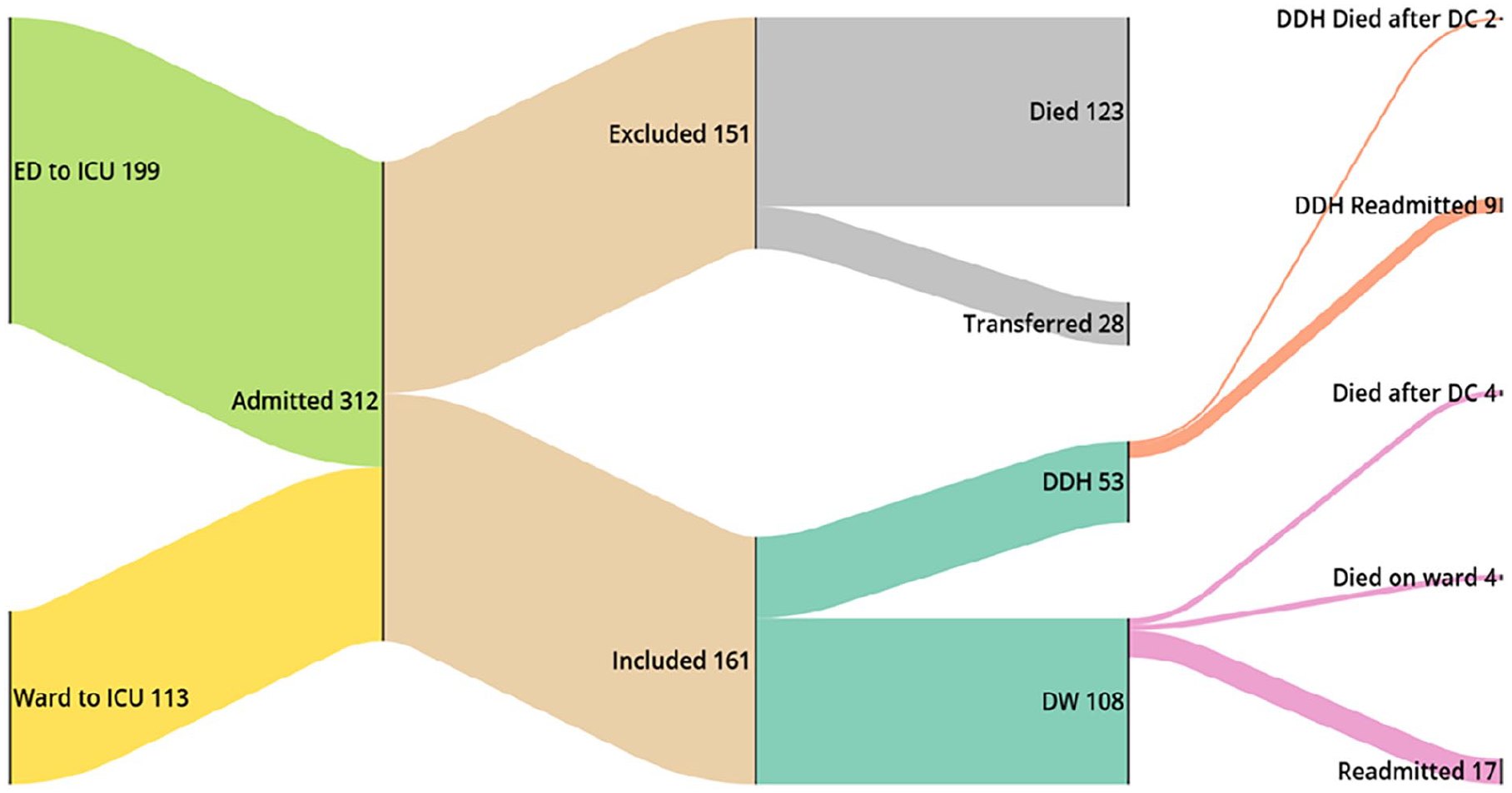
Sankey diagram of admission and discharge outcomes.
Results
312 patients were identified, of which 151 either died or were transferred to another hospital. Of 161 eligible patients, 53 (32.9%) were DDH and 108 (67.1%) were DW. In the DDH group, 40 patients (75.5%) were admitted from the emergency department, as were 54 (50.0%) of the DW group.
Table 1 summarises the data. At admission, patients in the DDH group were significantly younger, with lower APACHE II scores (p < 0.001). DDH patients were ventilated for fewer days (p < 0.001), and the time from extubation to discharge was shorter (p = 0.003). Once a decision to discharge was made, time to actual discharge was longer in the DDH group, though this was not significant. Overall length of stay was longer in the DW group (8 vs 15 days, p < 0.001).
Comparing admission characteristics, length of stay parameters and discharge outcomes in intensive care patients discharged direct to home, and patients discharged to ward.
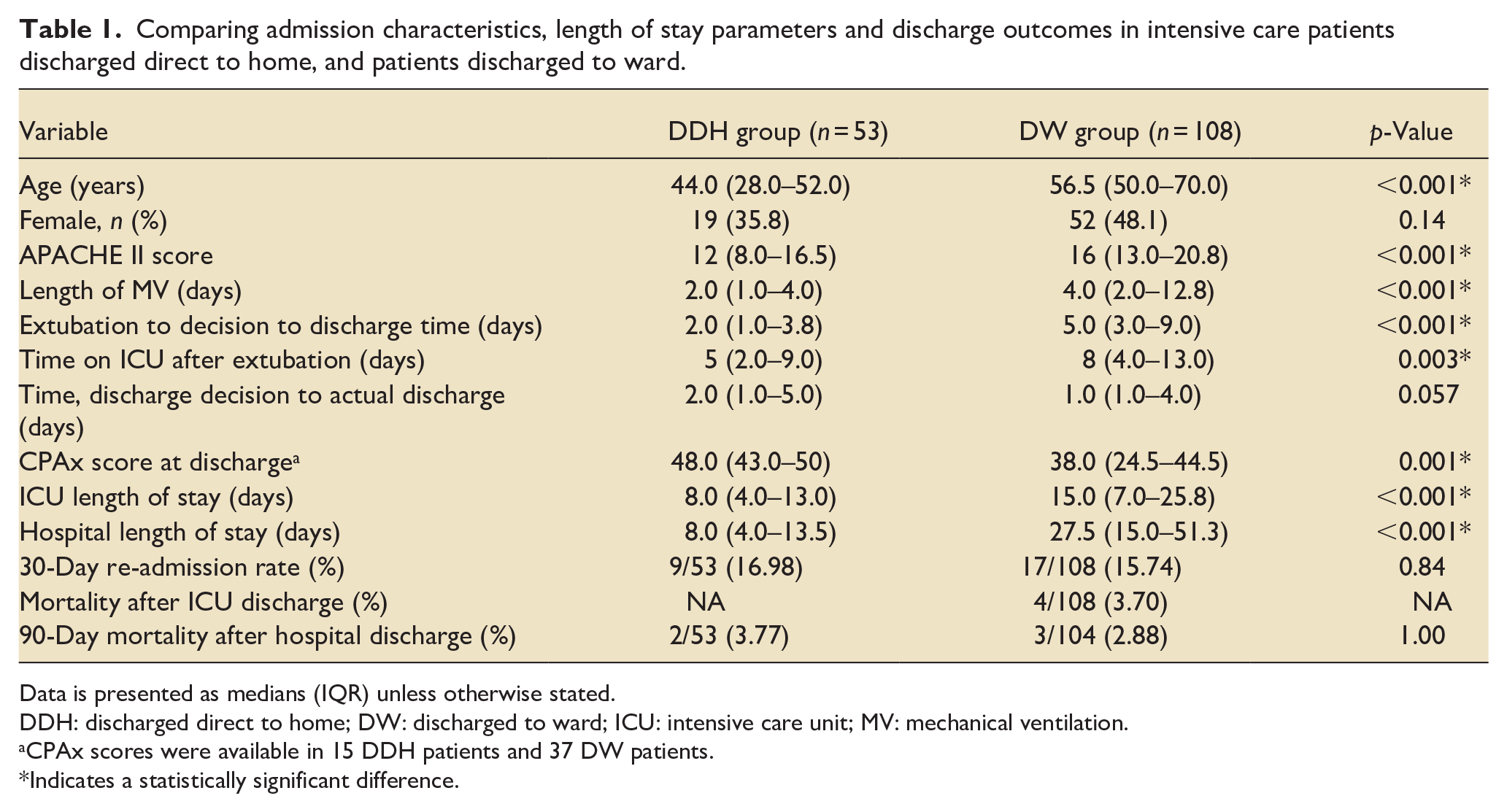
Data is presented as medians (IQR) unless otherwise stated.
DDH: discharged direct to home; DW: discharged to ward; ICU: intensive care unit; MV: mechanical ventilation.
CPAx scores were available in 15 DDH patients and 37 DW patients.
Indicates a statistically significant difference.
At discharge, CPAx scores were higher in the DDH group (48 vs 38, p = 0.001). There were no significant differences in 30-day inpatient re-admission, or 90-day mortality.
Discussion
Our findings are consistent with other studies, showing that DDH patients are younger, have lower illness severity scores on admission and are liberated earlier from mechanical ventilation.5 –7 In addition, we have demonstrated that not only is overall ICU length of stay longer in patients who are discharged to the ward, but the individual stages from admission to discharge (e.g. time to extubation, time to discharge after extubation) are longer in the DW group. This could be due to DW patients having other therapeutic needs, such as ongoing vasopressor use, which was not obtained from our data. We did however find that the time between declaring a patient ready for discharge and actually leaving ICU was longer in DDH, and may reflect a willingness on the part of clinicians to continue to wait for a ward bed.
We found in a small number of patients that physical function at ICU discharge was higher in DDH patients. Few studies have looked at physical function scores, although it has been found that the ability to stand within five days of admission, and pre-admission physical independence, were related to successful discharge home. 7 A previous study found that when patients were screened 3 months after discharge from ICU, their CPAx score increased from 31 at discharge to 47 at follow-up. 8 This is in contrast to our study, which found that the patients in the DDH group had median physical function scores of 48 points at ICU discharge. The differences in CPAx score could be explained by the shorter duration of mechanical ventilation. A larger study matching patients for illness severity and duration of mechanical ventilation would allow us to assess differences in physical function.
This study is limited as a single-centre evaluation, with physical function scores available in a small number of patients. The dataset did not provide reasons for admission and the use of calendar days for length of stay measures limits the accuracy of estimates. 9
Further multicentre prospective work, including randomised studies, are required to further elucidate the effect of DDH, and may lead to standardised protocols for safe discharge.
Footnotes
Acknowledgements
The authors would like to acknowledge the help of Susan Collingwood of Warrington Intensive Care Unit, and Lyndsey Williams of the Digital Analytics Department.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.