
Abstract
Introduction
Combined antiretroviral therapy has led to significant decreases in morbidity and mortality in acquired immunodeficiency syndrome patients. Survival among these patients admitted to intensive care units has also improved in the last years. However, the prognostic predictors of human immunodeficiency vírus patients in intensive care units have not been adequately studied. The main objective of this study was to evaluate if non-adherence to antiretroviral therapy is a predictor of hospital mortality.
Methods
A unicentric, retrospective, cohort study composed of patients admitted to a 59-bed mixed intensive care unit including all patients with human immunodeficiency vírus infection. Patients were excluded if exclusive palliative care was established before completing 48 h of intensive care unit admission. Clinical and treatment data were obtained, including demographic records, underlying diseases, Simplified Acute Physiology III score at the time of intensive care unit admission, CD4 lymphocyte count, antiretroviral therapy adherence, admission diagnosis, human immunodeficiency vírus-related diseases, sepsis and use of mechanical ventilation and hemodialysis. The outcome analyzed was hospital mortality.
Results
Overall, 167 patients were included in the study, and intensive care unit mortality was 34.7%. Multivariate analysis indicated that antiretroviral therapy adherence and the Simplified Acute Physiology 3 score were independently related to hospital mortality. antiretroviral therapy adherence was a protective factor (OR 0.2; 95% CI 0.05–0.71; P = 0.01), and Simplified Acute Physiology 3 (OR 1.04; 95% CI 1.01–1.08; P < 0.01) was associated with increased hospital mortality.
Conclusion
Non-adherence to antiretroviral therapy is associated with hospital mortality in this population. Highly active antiretroviral therapy non-adherence may be associated with other comorbidities that may be associated with a worst prognosis in this scenario.
Introduction
It is estimated that 36.9 million people live with human immunodeficiency virus (HIV) infection worldwide, with approximately 2 million new cases and 1.2 million deaths per year. 1 Patients with HIV in the intensive care unit (ICU) form a special group with specific disease presentations, management and outcomes. 2 Admission of HIV-infected patients to the ICU has occurred since the beginning of the epidemic in the 1980s. 3 At that time, the reported mortality rates ranged from 86% to 100% among patients with mechanical ventilation, which was mainly caused by Pneumocystis jirovecii pneumonia.4,5 In recent years, the rates of hospitalization and mortality due to HIV infection have decreased with the discovery of new therapeutic options, especially after the advent of antiretroviral therapy (ART). 1 In fact, major progress has been made, such that these patients being treated in ICUs have decreasing mortality rates. 6 However, the prognostic predictors in this population are poorly described, including the previous or current use of ART and prior therapeutic adherence.7,8 The main objective of this study was to evaluate the main risk factors for ICU mortality in this population, specifically previous ART use, immunosuppression status and antiretroviral adherence.
Methods
A retrospective cohort study was conducted in the adult ICU of the Hospital Nossa Senhora da Conceição, an 800-bed tertiary hospital located in Porto Alegre, Brazil. The ICU has 59 beds and covers all medical and surgical cases. The study was approved by the local Ethics Committee (institutional review board number 60248716.3.0000.5530). Informed consent was waived because of the observational nature of the study. The study cohort included all patients with HIV infection that were admitted to the ICU in a “full code” status, that is, patients who do not have withholding or withdrawing of life-sustaining treatments, between January 2014 and December 2015. HIV diagnoses were confirmed by anti-HIV serology and HIV viral load, and at least one CD4+ (CD4) lymphocyte cell count was performed before or immediately after ICU admission. Patients were excluded if exclusive palliative care was established before completing 48 h of ICU admission. Clinical and treatment data were obtained retrospectively from the patient’s medical charts and electronic records, including demographic records, underlying diseases, Simplified Acute Physiology (SAPS) III score at the time of ICU admission, CD4 lymphocyte count, ART adherence, admission diagnosis, HIV-related diseases, sepsis and use of mechanical ventilation (MV), hemodialysis (HD) or vasopressor. Patients were defined as adherent to ART if they or their next-of-kin reported taking their medication ‘all of the time’ or ‘most of the time’ (month long adherence) or if they had not missed any medications in the past week/3-day period. 9 The outcome analyzed in this study was hospital mortality. Patients who were treatment-naïve were not included in the analysis that explored ART adherence.
Continuous variables were reported as the means with standard deviation (SD) when distributed normally or as the medians with interquartile range when skewed. Differences between mean values were tested via Student’s t-test, and differences between medians were assessed using the Mann–Whitney U-test. Categorical data were summarized as proportions, and a chi-square test or Fisher’s exact test was used to examine differences between groups. We developed a downward logistic regression for the primary outcome (hospital mortality). Variables were included in the model using a P-value < 0.1 as a cut-off. Covariates in the model included demographics, comorbidities, SOFA score, antibiotic therapy and time of antibiotic therapy. All tests were two-tailed, and a P-value < 0.05 was deemed a priori to represent statistical significance. All analyses were performed using SPSS 19.0 software (IBM SPSS, Armonk, NY, USA).
Results
Main clinical characteristics.
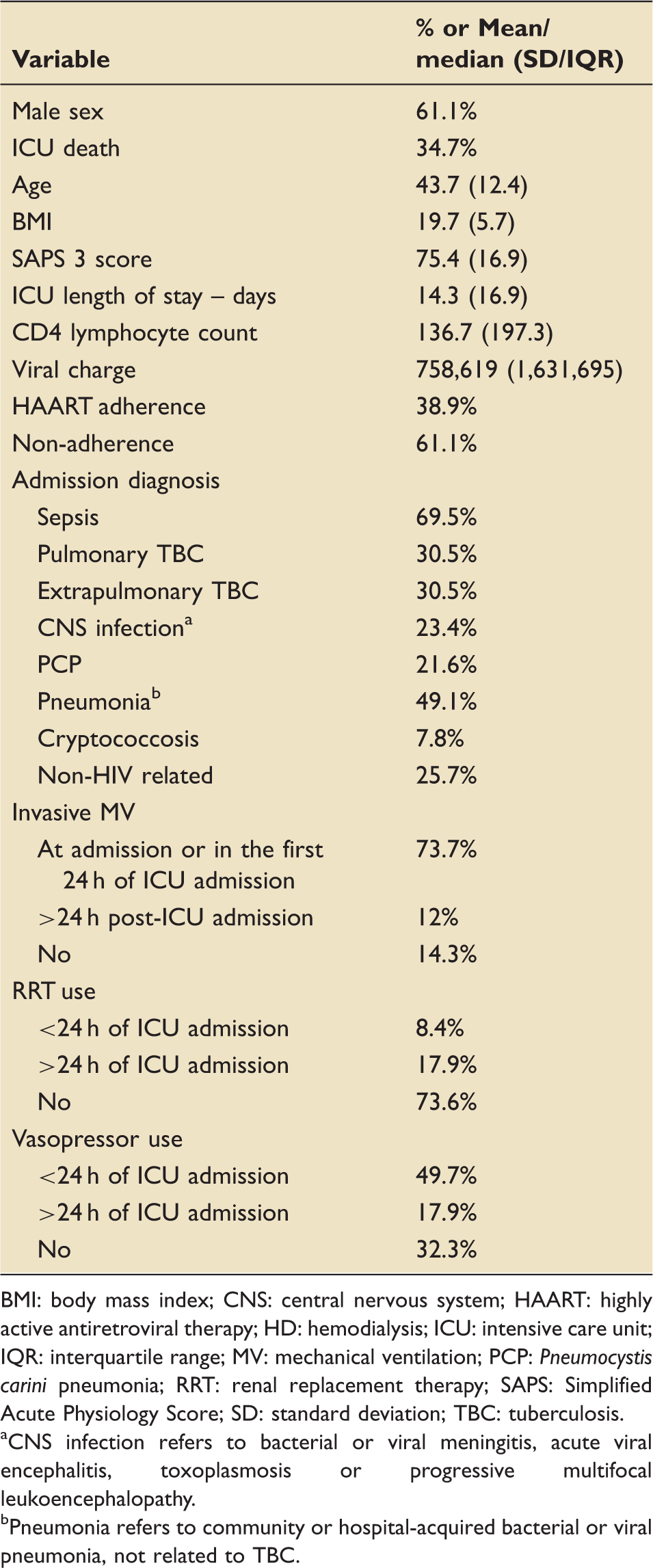
BMI: body mass index; CNS: central nervous system; HAART: highly active antiretroviral therapy; HD: hemodialysis; ICU: intensive care unit; IQR: interquartile range; MV: mechanical ventilation; PCP: Pneumocystis carini pneumonia; RRT: renal replacement therapy; SAPS: Simplified Acute Physiology Score; SD: standard deviation; TBC: tuberculosis.
CNS infection refers to bacterial or viral meningitis, acute viral encephalitis, toxoplasmosis or progressive multifocal leukoencephalopathy.
Pneumonia refers to community or hospital-acquired bacterial or viral pneumonia, not related to TBC.
Patients who were discharged from the hospital did not have a CD4 count higher than patients who died during hospitalization (91 ± 135 versus 69 ± 95; P = 0.69, respectively). Patients with CD4 counts below 50 cells/ml had a mortality rate of 34.9%, similar to the rate of those with CD4 counts between 50 and 200 cells/ml (34.2%) and above 200 cells/ml (35.3%); P = 0.994. There were no differences between patients discharged from the hospital and those that died in relation to age (44 ± 19 versus 42 ± 14; P = 0.11, respectively), BMI (19 ± 5.6 versus 18.5 ± 6; P = 0.3, respectively), previous ART use (OR 1.26, 95% CI 0.76–2.08; P = 0.374, respectively) or sepsis at admission (OR 1.68 95% CI 0.97–2.90; P = 0.04, respectively), and they were not associated with the outcome. The bivariate analysis showed that the factors related to hospital mortality were ART adherence (OR 0.48; 95% CI 0.29–0.8; P = 0.003); invasive MV (OR 1.68; 95% CI 1.46–1.92; P = 0.001), vasopressor use (OR 2.15; 95% CI 1.89–9.0; P = 0.001), hemodialysis (OR 2.11; 95% CI 1.43–3.1; P = 0.001), vasopressor use at admission (OR 6.8; 95% CI 2.7–17.21; P = 0.001) and the SAPS 3 score (70 ± 18 in patients with ICU discharge versus 84.5 ± 25 for ICU death; P = 0.001). Association between variables and the outcome (hospitalar mortality) are described in Table 2. Of the 119 patients who were on ART at admission to the ICU, 75 were discharged and 44 died. Patients with HAART adherence had higher CD4 count as compared with non-adherent patients: 151 (346–74) versus 57 (111–12), P < 0.001; but not different SAPS 3 score at ICU admission: 74 (±16) versus 77 (±18), P = 0.49; respectively.
A logistic regression was performed to ascertain the effects of age, hospital length-of-stay before ICU admission, undetectable viral charge, ART adherence, invasive MV, hemodialysis, sepsis at ICU admission and SAPS 3 score on hospital mortality. We did not include vasopressor use at admission because it is a variable included in the SAPS 3 score. The logistic regression model was statistically significant (χ2 = 46,417; P < 0.0001). The model explained 43.9% (Nagelkerke R2) of the variance in hospital mortality and correctly classified 72.5% of the cases. The only variables independently related to outcome (hospital death) were ART adherence and SAPS 3 score. ART adherence was a protective factor (OR 0.2; 95% CI 0.05–0.71; P = 0.01), and SAPS 3 (OR 1.04; 95% CI 1.01–1.08; P < 0.01) was associated with hospital mortality (Table 3). The need for MV could not be submitted to the model because there were no deaths among patients who were not submitted to MV; thus, it was impossible to apply the regression formula since a division would have occurred by zero.
Discussion
The mortality of HIV-infected patients admitted to the ICU in the study was in line with previous reports.10,11 It is likely that the improved prognosis of HIV-infected patients admitted to the ICU is related to a combination of ICU-related factors, such as patient selection, early diagnosis, ART and prophylaxis for PCP. In addition, important changes have been seen in intensive care management in the last two decades, such as the use of mechanical ventilation with low tidal volume in the treatment of pulmonary injury 12 and more aggressive measures in the treatment of sepsis. 13 The association between ART use and ICU survival in HIV-infected patients remains controversial.14,15 The administration of ART in the ICU is complicated by potential drug interactions, pharmacokinetics issues and the risk of provoking immune reconstitution inflammatory syndrome. 2 To our knowledge, this is the first study to evaluate the impact of previous ART adherence on ICU prognosis in HIV patients and could at least partially explain the controversial results regarding previous ART use and ICU outcomes. These data, however, are not free of potential biases. Because this was a retrospective study, we cannot rule out the fact that non-adherent patients are more likely to be withdrawn from life support interventions compared to treatment-naïve patients or those with good ART adherence. The allocation of patients after 48 h of ICU admission and the inclusion of only ‘full code status’ patients attempted to minimize this fact, which may still be an issue. Besides this, ART non-adherence may be associated with another comorbidities that may be associated with a worst prognosis, such as medical comorbidities, psychiatric disease and substance-use disorders. The true impact of this potential association cannot be measured in our work.
The main diagnosis that led HIV patients to hospitalization in our ICU was sepsis (69.5%), and this diagnosis was related to increased mortality in the bivariate analysis, a finding similar to previous reports. 8 On the other hand, the diagnosis of sepsis lost statistical significance in the multivariate analysis. We believe that this phenomenon is because the severity of organ dysfunction and comorbidities – reflected by the SAPS 3 index – relates more to mortality than the diagnosis of sepsis. Several studies previously reported the same finding, and the intensity of organic dysfunction is a strong predictor of prognosis in this population.15–17 The present study did not find an association between CD4+ T-lymphocyte count or viral load and ICU death. Several authors have already reported that the CD4+ T-lymphocyte count is not associated with death in the short term7,18 but may be a long-term prognostic predictor. 17
We recognize that our study has several limitations. First, it was carried out at a single institution, which was an urban public hospital. Since clinical practice and demographics may differ between institutions, the external validity of our study may be limited. Second, we did not follow-up with patients after discharge from the hospital. Therefore, the predictors of long-term survival and any impact of ART on long-term survival remain unknown. Given the retrospective nature of our study, we chose to focus on survival until discharge from the hospital, where we had information on all patients, rather than on long-term survival. Third, patients were admitted with a broad spectrum of critical illnesses and received heterogeneous treatments, which limits our conclusions about the independent effects of any specific treatment or intervention. Studies examining subsets of specific patients (e.g., those with respiratory insufficiency and acute lung injury) are best suited to examine the impact of a specific intervention (e.g., ventilation with low tidal volume, noninvasive MV). Fourth, the definition of ART adherence used in this work is only qualitative, and is not free of bias. Despite the need for rigorous assessment of ART adherence, a ‘gold standard’ has not yet been found, but a quantitative measurement of adherence, if possible, could provide greater robustness to the results of this study. 19 Finally, the observational nature of our study limits any firm conclusions regarding the use of ART and mortality.
Conclusion
Association between clinical charts and outcome.
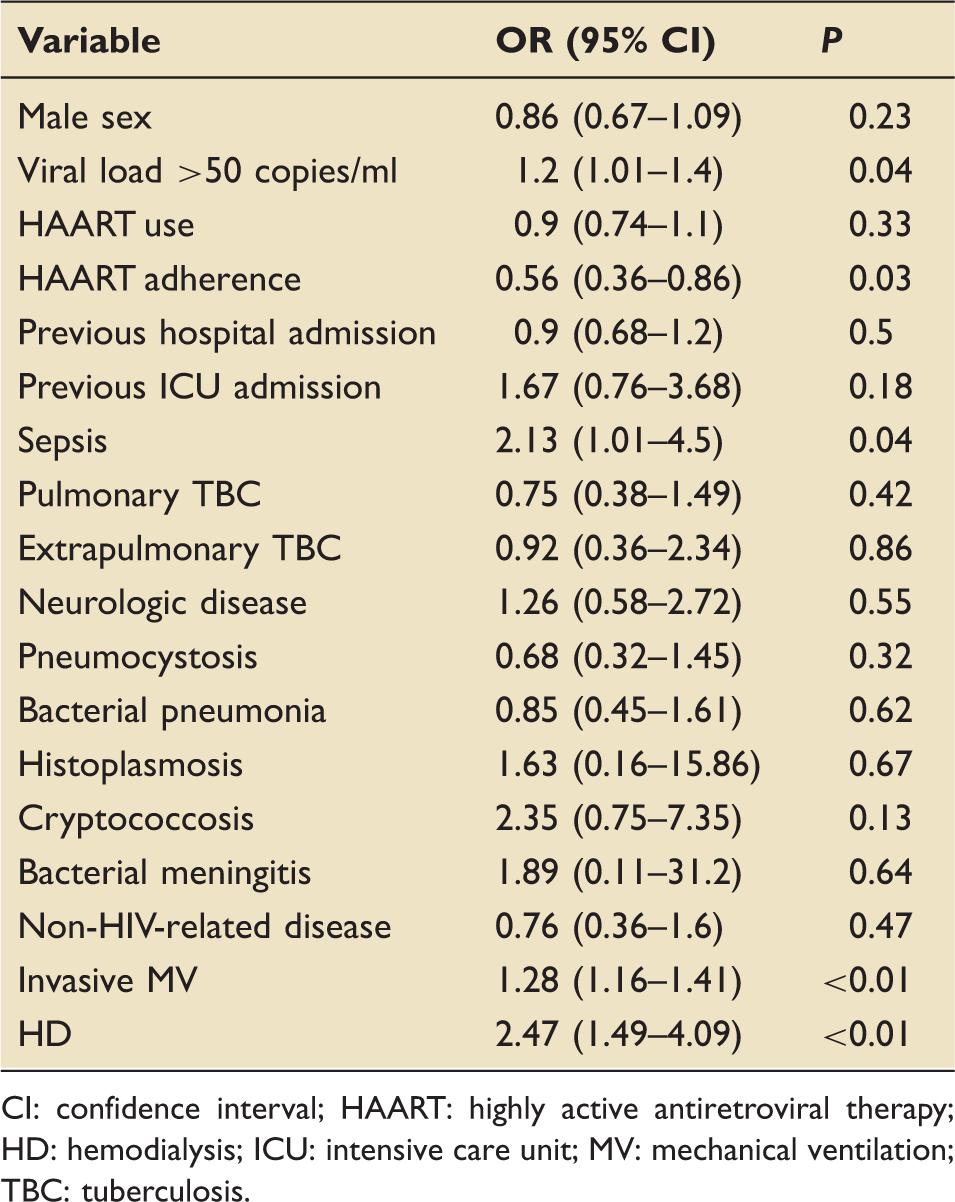
CI: confidence interval; HAART: highly active antiretroviral therapy; HD: hemodialysis; ICU: intensive care unit; MV: mechanical ventilation; TBC: tuberculosis.
Multivariate analysis of variables and hospital mortality.
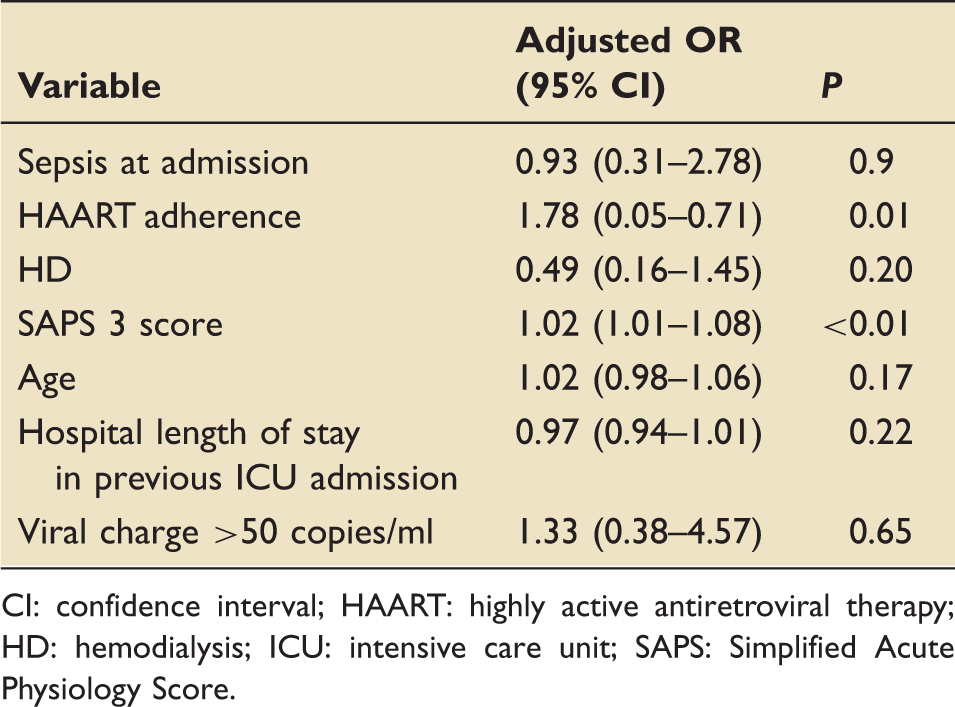
CI: confidence interval; HAART: highly active antiretroviral therapy; HD: hemodialysis; ICU: intensive care unit; SAPS: Simplified Acute Physiology Score.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.