
Abstract
Introduction
Troponin elevation is central to the diagnosis of acute type 1 myocardial infarction. It is, however, elevated in a range of other conditions, including type 2 myocardial infarction, and this setting is increasingly associated with adverse clinical outcomes. Patients within intensive care frequently have at least one organ failure together with a range of co-morbidities. Interpretation of troponin assay results in this population is challenging. This clinical uncertainty is compounded by the introduction of ever more sensitive troponin assays.
Areas covered
The aims of this review are to (a) describe the currently available literature about the use of troponin assays in intensive care, (b) analyse the challenges presented by the introduction of increasingly sensitive troponin assays and (c) assess whether the role of troponin assays in intensive care may change in the future, dependent upon recent and ongoing research suggesting that they are predictive of outcome regardless of the underlying cause: the ‘never means nothing’ hypothesis.
Keywords
Introduction
The aims of this review are to (a) describe the currently available literature about the use of troponin assays in intensive care, (b) analyse the challenges presented by the introduction of increasingly sensitive troponin assays and (c) assess whether the role of troponin assays in intensive care may change in the future, dependent upon recent and ongoing research suggesting that they are predictive of outcome regardless of the underlying cause: the ‘never means nothing’ hypothesis.
Cardiac troponins (cTns) are considered the gold standard biomarker for the diagnosis of myocardial infarction (MI) and are required to rise above the 99th percentile of a reference population of ‘normal’ individuals, in association with relevant symptoms and/or ECG findings, to confirm this diagnosis. 1 There are three subtypes of cTn which form a regulatory complex that controls the contraction of striated muscle, two of these, cTnT and cTnI, are specific to the myocardium and as such are in clinical use today. 2 The cTn complex is bound to the thin filament via tropomysin and cTnT. CTnI acts by binding and inhibiting the interactions between the thick and thin filaments. Importantly, from a clinical perspective, the diagnostic performance of recent iterations of assays for both cTnI and cTnT is similar. 3
Whilst the introduction of the original cTn assays was a major advance, these had an important limitation; the sensitivity within the first few hours to rule out MI was poor, which meant that further samples were needed at 10–12 h to reach adequate diagnostic levels of sensitivity and specificity.4–6 This limitation not only resulted in potential delays in making the correct diagnosis but also had significant time and resource implications for hospital admission services. It is this issue that led to the development of highly sensitive cardiac troponins (hs-cTn). Hs-cTn can be detected in more than 50% of the general population. 6 The hs-cTn assays show improved diagnostic performance, in terms of exclusion of acute MI, within a few hours of admission, with reported areas under the receiver–operator curve of greater than 0.90 and up to 0.96.4,5,7 This does, however, raise another challenge in the clinical setting: the increased sensitivity of these assays has now resulted in hs-cTn being regularly detected in a variety of clinical situations not traditionally associated with MI.8,9 This is particularly pertinent to the intensive care population.
Type of MI and the causes of cTn elevation
Type of MI as defined by the Universal Definition. 1
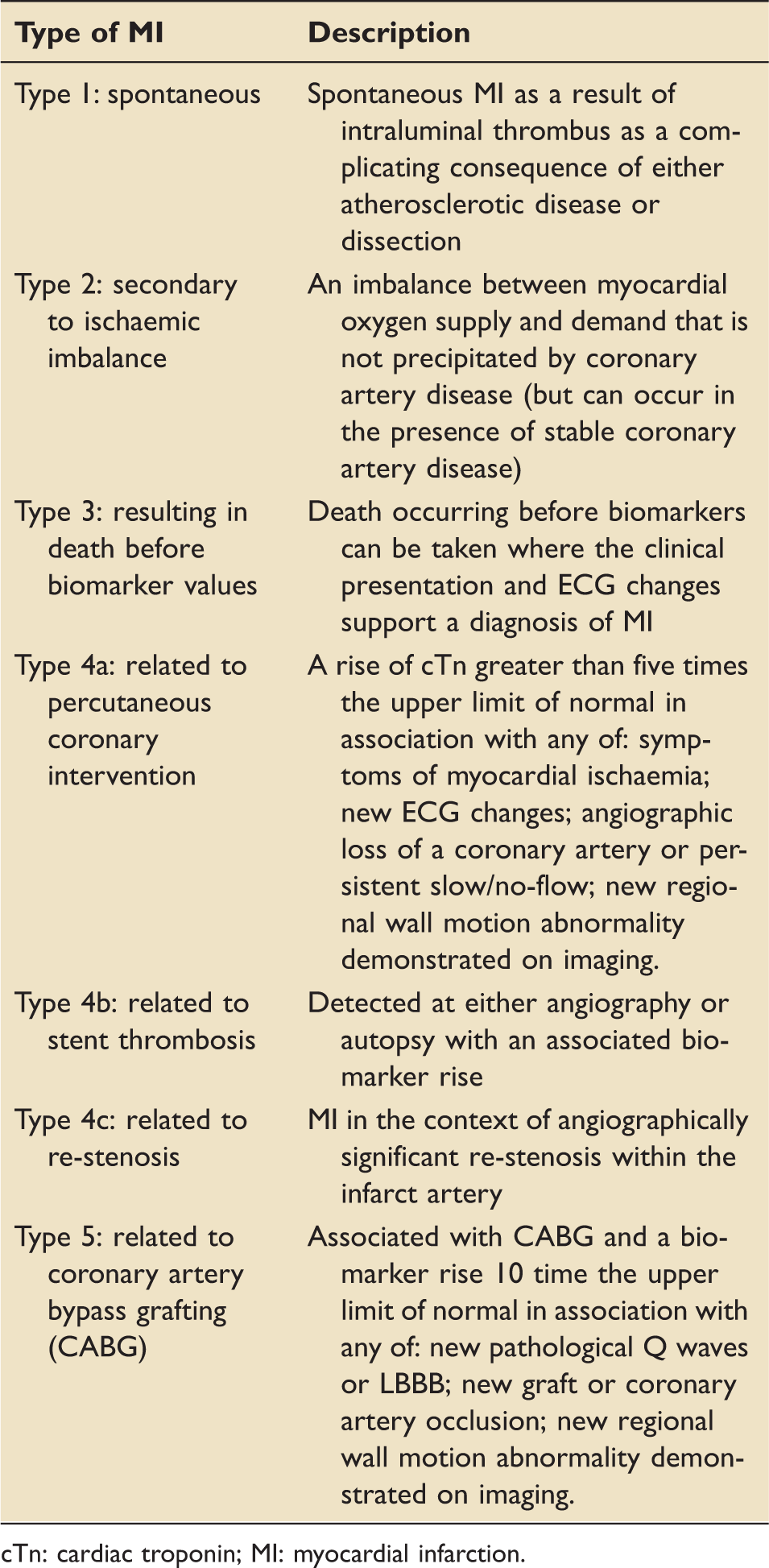
cTn: cardiac troponin; MI: myocardial infarction.
The commonest aim when hs-cTn is used in front line clinical practice is to rule out or detect T1MI because the evidence base clearly demonstrates that these patients benefit prognostically from a fast track combination of pharmacological and invasive interventions. 8 However, there is no evidence that patients with a T2MI, or other causes of troponin elevation, benefit from such interventions. This highlights the importance of interpreting the cTn result with a higher degree of sophistication than assuming it automatically indicates a T1MI.
Cardiac and non-cardiac causes of cTn elevation.
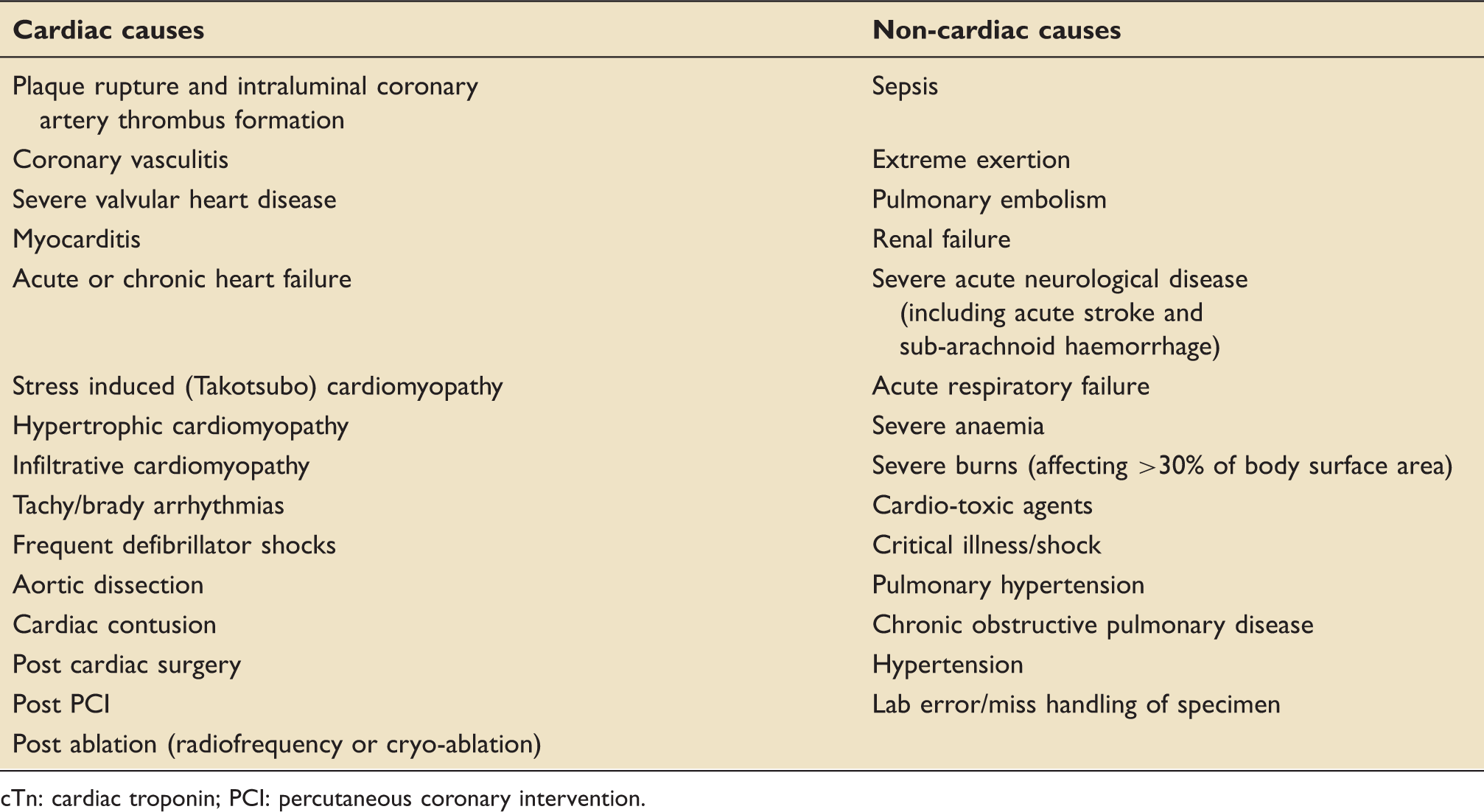
cTn: cardiac troponin; PCI: percutaneous coronary intervention.
It is therefore paramount that clinicians can distinguish between the patient who has had a T1MI, in whom optimal medical therapy and potential revascularisation provide benefit,14,15 and the cTn positive patient who has not had a T1MI in whom such therapies have no role and could be harmful. The commonly employed clinical algorithm that an elevated cTn, or even a rise in the cTn level, indicates a T1MI by default is clearly flawed: both T1 and T2 MIs are characterised in this way.8,12 In routine circumstances, cTns should therefore be interpreted in the light of the clinical history and, specifically, an absence of a history of cardiac-sounding chest pain automatically makes the diagnosis of T1MI questionable in most clinical circumstances.8,12,16 This makes interpretation in sedated and ventilated patients particularly challenging. As a result it is easy to miss MI in ICU, as demonstrated by the increased MI diagnoses during intensive ECG and cTn screening.17,18 Of some help to the clinician is the observation that the higher elevation in cTn the more likely that a T1MI has occurred, but as already indicated, even a very high cTn elevation should be interpreted in relation to the clinical context. 8 Further adding to the diagnostic challenge in ICU, there is variable agreement in 12 lead ECG interpretation. 19 It is important, however, that the significance of an elevated cTn level in a patient is understood, even when T1MI has been excluded, because there are consistent data across the literature that demonstrate, probably irrespective of the underlying cause, that this is a biomarker associated with a worse clinical outcome.8,10,12,16
cTn in general intensive care
Given that standard cTn (ScTn) assays were brought into clinical practice around 20 years ago there is a large body of evidence relating to their use in intensive care.
Incidence of ScTn elevation in intensive care
Figure 1 demonstrates the wide variation in the reported incidence of ScTn elevation on admission to intensive care, with the highest reported rates of 90% in patients with sepsis.
20
This range includes data from retrospective, observational studies which have the advantage of larger sample sizes but also the disadvantage of uncontrolled selection (one retrospective study for example had a 97% male cohort,
21
whilst another demonstrated that ScTn was more likely to be tested with increasing age, severity of co-morbities and severity of illness).
22
The variation in incidence is also likely to be partly explained by heterogeneity of criteria for admission to ICU, variability of case-mix between cohorts and differences in ScTn assays between studies.
Scatter plot of the reported percentages of patients with an ScTn elevation above the 99th centile on admission to intensive care.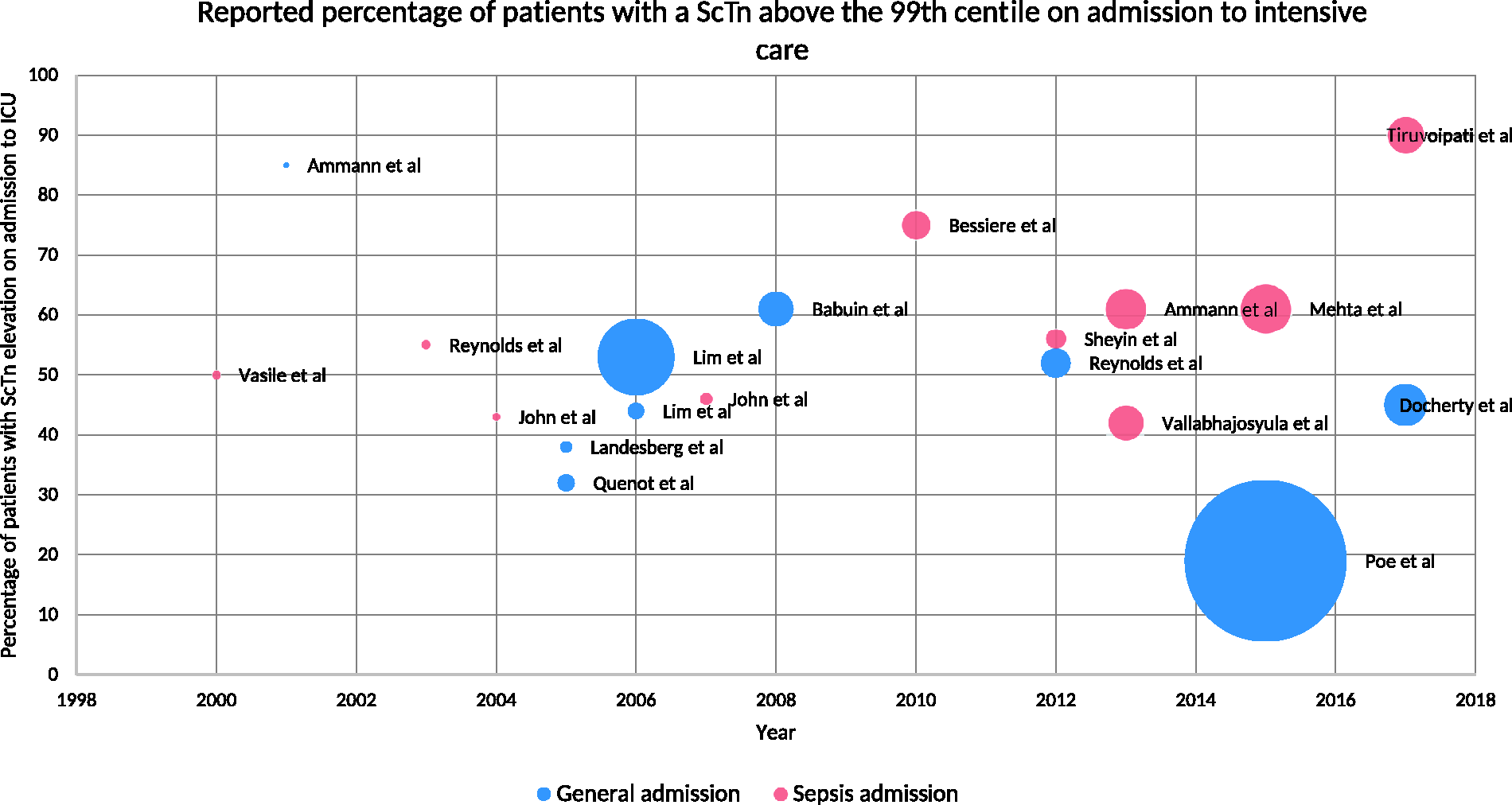
Interestingly, studies that looked for dynamic changes in ScTn throughout the admission demonstrated that there were some patients that developed elevated ScTn levels after admission and that levels were highest on average on day two of the admission.23,24 If cTn assays are found to represent a tool with which to help in the risk stratification of critical care patients, this observation highlights the importance of serial measurements and of interpreting abnormal values in the context of the timing and frequency of measurement.
A significant proportion of admissions to ICU follow surgical procedures. Interestingly a large international cohort study of postoperative patients (not necessarily within ICU) demonstrated that a ScTn level above the 99th centile in conjunction with either ischaemic symptoms or ECG changes was an independent predictor of 30-day mortality. 25 Whilst this observation provides helpful prognostic data, there are not as yet any robust data to support a change in the clinical management of these patients. 26
Factors associated with ScTn elevation in intensive care
There is a clear association between ScTn elevation and both age and the co-morbid state of a patient (cardiovascular (CV) risk factors, previous CV disease and chronic kidney disease).20,22,23,27–30 The magnitude of these associations is, however, inconsistent between studies.
There is also variation in the incidence of ScTn elevation depending on the type of admission to ICU, whether that be medical (76%), unplanned surgical (54%) or planned surgical (32%). 23 This is perhaps intuitive as it could be postulated that patients with planned admissions are frequently admitted in anticipation of the possibility of adverse events, which may not in fact occur, whereas unplanned admissions typically occur following a period of clinical deterioration before admission, often characterised by haemodynamic compromise that could result in ScTn elevation. In support of this notion, the Acute Physiology and Chronic Health Evaluation score which combines indicators of acute physiological disturbance with long-term health inputs has been shown to be closely associated with ScTn elevation in a number of studies.20,22,27–34
Myocardial infarction in intensive care
Left ventricular systolic dysfunction is seen more frequently in patients with ScTn elevation, particularly in the context of sepsis, but this observation does not, however, help to differentiate between a T1 and T2MI.27,31,35,36 Whilst the observation that regional wall motion abnormalities are around 10 times more common in patients with elevated ScTn levels, clinical uncertainty remains given that this finding could be a reflection of a previous history of IHD which as described is clearly associated with ScTn elevation in intensive care. 31 Two small studies contained cohorts that underwent further investigation (stress echo, coronary angiography or autopsy) to ascertain whether there was significant coronary artery disease in those patients with elevated ScTn levels. Both studies demonstrated that the overwhelming majority (10/11 and 23/25) had no significant underlying coronary artery disease.35,37 These observations highlight the difficulties of interpreting ScTn results in the context of critical illness and demonstrate that the incidence of important coronary disease is low; suggesting that in the majority of patients elevated ScTn indicates a T2MI.
Outcome and level of support associations with ScTn elevation in general intensive care
Two studies, one small prospective and one larger retrospective study have demonstrated that ScTn concentration does not predict the need for mechanical ventilation20,31 There is, however, discordance between studies as to whether an elevated ScTn level on admission is associated with (a) the use and (b) level of CV support.20,27,31 One highly cited meta-analysis reported that ScTn elevation was associated with increased length of ICU stay (3 days extra, p = 0.004) but not length of hospital stay (2.2 days extra, p = 0.12). 38
ScTn elevation incidence and association with outcome in general intensive care.
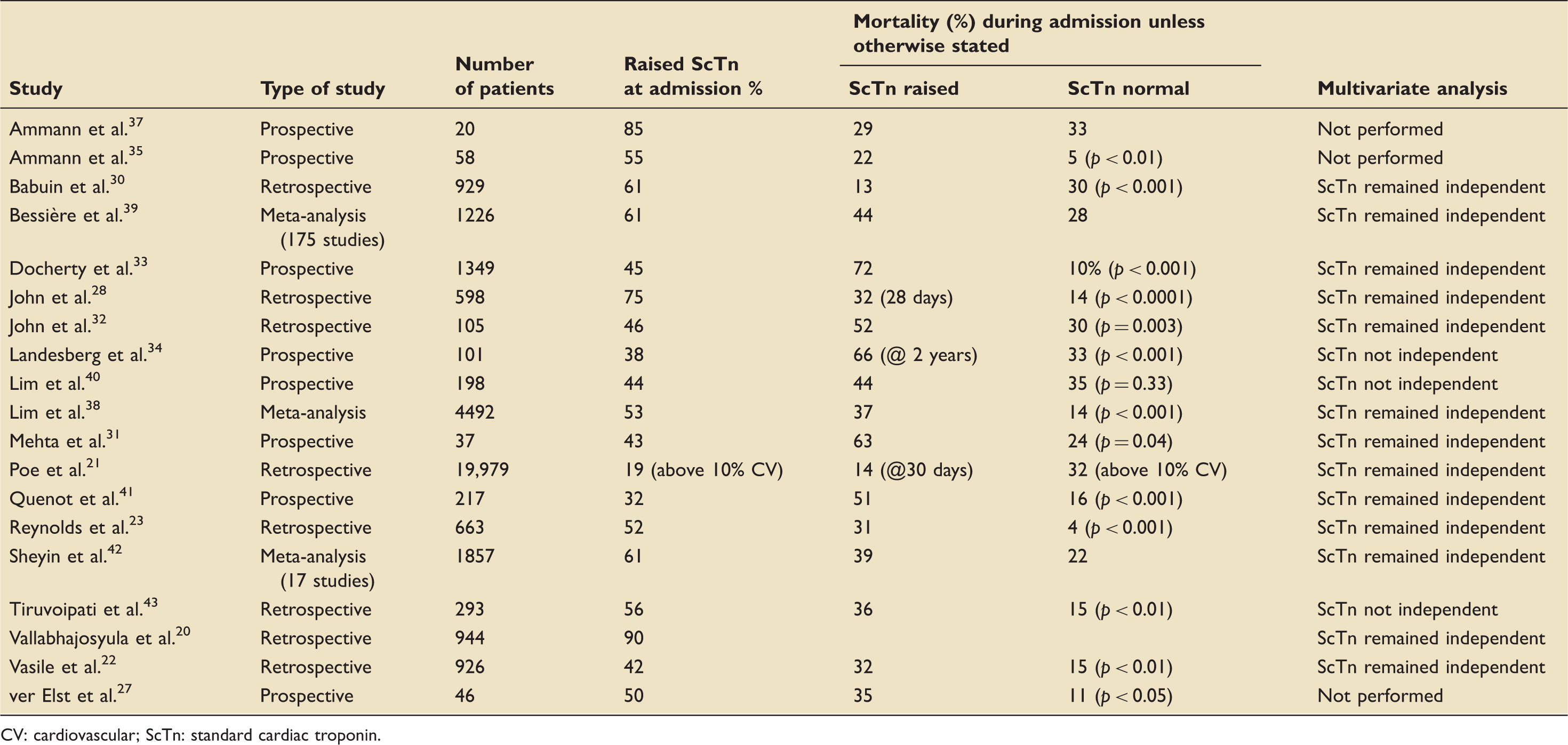
CV: cardiovascular; ScTn: standard cardiac troponin.
Cardiac intensive care
A substantial proportion of patients admitted to a specialist cardiac intensive care would be expected to have an elevated cTn. In common with data presented thus far, patients with a greater burden of CV risk factors (including hypertension and diabetes) had higher ScTn levels following mitral valve surgery. 46 More complex surgical disease and longer cross clamp times are also associated with higher ScTn levels (in patients undergoing either mitral valve surgery or coronary artery bypass grafting (CABG)).46,47 Furthermore, patients with higher ScTn levels post operatively have a longer length of stay and worse outcomes.46–49 Given the potential for confounding factors, it is interesting to note that the highest ScTn levels were independently associated with both increased length of stay and worse outcomes both in hospital and at one year following mitral valve surgery or CABG.46,47
Neurosciences intensive care unit
ScTn elevation has also been described in the context of brain injury, possibly as a result of an adverse response to the catecholamine surge occurring as a consequence of the injury.50–53 In the context of intracerebral haemorrhage, managed within neurosciences intensive care, ScTn elevation was an independent predictor of outcome whether on admission or following surgery. 51 However, in the context of subarachnoid haemorrhage (SAH), Deibert et al. found no association between ScTn elevation and prior co-morbidity, clinical and radiological severity of SAH or outcome. 52 This study, which excluded patients with previous cardiac disease or abnormal echocardiograms, found that over half of patients with ScTn elevations had evidence of left ventricular dysfunction compared to none of the patients with normal ScTn levels. 52 Of interest, this response was also transient: in all cases, the LV dysfunction subsequently returned to normal during follow-up. 52 These data suggest that myocardial injury in such cases is transient and unlikely to be due to a T1MI. Of further reassurance that ScTn elevation in critical care does not necessarily mean a T1MI, six (50%) of the patients with ScTn elevation went on to have clinically driven investigations which excluded significant coronary disease or myocardial ischaemia in all of them. 52 Furthermore even in the presence of ischaemic ECG, studies have consistently demonstrated no evidence of T1MI, thus providing reassurance that these findings should be considered in the context of SAH. 54 ScTn, therefore cannot differentiate between T1MI and T2MI/myocardial injury in these patients.
Hs-cTn in intensive care: A modern dilemma
Given the increased sensitivity of the Hs-cTn assays, the proportion of ICU patients with cTn elevation will inevitably expand further. However, a growing body of evidence suggests that cTn measurement may have an alternative value in terms of risk stratification and possibly prognostication. The question is whether hs-cTn measurement will translate into improved prognostication or just add confusion and further inappropriate testing when acute coronary syndrome is suspected in a cohort of patients who cannot provide a history.
Hs-cTn in general intensive care
The majority of studies using hs-cTn were performed in patients presenting to intensive care with sepsis. A single study of all patients in general intensive care found detectable levels in the vast majority (98%) with 75% above the 99th centile. 55 Three studies to date have reported the incidence of Hs-cTn elevation in sepsis presenting to intensive care to be above the 99th centile in 60% to 88%.56–58 Importantly one study demonstrated that an additional 7% of patients developed elevated hs-cTn levels within four days. 58
There was an association between Hs-cTn and increasing age, co-morbid state and severity of illness score.56–58 A discordant relationship between hs-cTn and outcome is apparent in these studies. The larger study by Frencken et al. demonstrated a steady increase in hazard ratio of 14-day mortality with increasing levels of hs-cTn up to 100 ng/L (hs-cTnI Abbott ARCHITECT STAT assay, upper reference limit 26 ng/L) at which point the risk plateaued. 58 On multivariate analysis the moderate (100–500 ng/L) and high (>500 ng/L) hs-cTn levels were independently associated with 14-day mortality (HR 1.72 (95% confidence interval 1.14–2.59) and HR 1.70 (95% confidence interval 1.11 to 2.6) respectively). 58 There was, however, no association between hs-cTn and one year mortality. 58 Further, both the smaller studies and another study did not demonstrate that Hs-cTn was an independent predictor of mortality.56,57,59
Landesberg et al. performed echocardiography, and, unlike a number of the ScTn studies, found no link between Hs-cTn and left ventricular ejection fraction. It is notable, however, that there was an association between Hs-cTn and indexed right ventricular end diastolic volume. 56 Of further interest, Røsjø et al. performed ScTn alongside hs-cTn to allow a comparison between these two cTns in 204 patients. The prevalence of hs-cTn elevation on admission was predictably higher than ScTn (80% compared to 42%) and, interestingly, hs-cTn did differentiate between survivors and non-survivors whilst ScTn did not. 57 However, neither were significant predictors of outcome on multivariate analysis. 57
In an attempt to assess whether hs-cTn elevation was associated with longer term CV morbidity, Frencken et al. reviewed usage of CV medications in a smaller subset of the patients after one year (122 with elevated hs-cTn and 78 with normal hs-cTn). This demonstrated that patients with hs-cTn elevation during their ICU stay increased the number of CV medications in the following year (median increase of 1 medication p = 0.002), whereas the hs-cTn negative patients did not have an increase in CV medications. 58 Interpreting these results is challenging as it is uncertain whether the hs-cTn positive group started the CV medications as a result of a genuine development of CV morbidity or as a potential result of misinterpretation of the hs-cTn result. Surprisingly, however, the use of antithrombotic medications increased in both the hs-cTn positive and negative groups (42% to 54% (p = 0.007) and 28% to 40% (p = 0.03) respectively). 58
Hs-cTn in cardiac ICU
A single study assessed the use of Hs-cTn post aortic valve replacement in 79 patients. Unsurprisingly, it demonstrated that the Hs-cTn level rose post procedure. 60 Higher Hs-cTn values were associated with longer cross clamp times, longer time on bypass and longer surgical procedures as demonstrated in the ScTn studies. 60 Hs-cTn was, however, not independently associated with inotrope requirement or length of stay. 60
Future roles for hs-cTn: The ‘never means nothing’ hypothesis?
Whilst cTn remains the gold standard tool for the exclusion/diagnosis of an ‘MI’, this role is often oversimplified in acute medicine/emergency departments due to (a) low awareness of the frequency of T2MI, and (b) uncertainty about the validity of the manufacturer's quoted 99th centile value as an ‘upper limit of normal’. These factors limit the attempt to use cTn assays as a binary arbiter of T1MI. The clear strength of the test, particularly true of the newer hs-cTn assays, is the ability to robustly rule out T1MI early in the assessment period. By contrast, interpretation of a positive test is becoming increasingly complex, especially in patients without a classical history of cardiac pain. Misdiagnosis of a patient with T2MI or some other reason for myocardial injury exclusive of T1MI can lead to inappropriate investigations and treatment. In intensive care, in particular, the inflammatory and co-morbid status of patients compounds the likelihood that a cTn elevation is due to multifactorial myocardial injury. Thus, the conventional use of cTn to diagnose T1MI is increasingly compromised outside the context of a patient with a classical history, but the clinical value of a negative result to rule out this diagnosis remains high. However, the data are clear that T2MI does not have a benign outcome either, so this diagnosis has value in its own right. Increasingly evidence is accumulating that in the general population an elevated hs-cTn is a biomarker for the risk of acute CV events. Furthermore, in intensive care, there is a body of data to suggest that hs-cTn assays may also provide some risk stratification and even prognostication. More data are now required, but this early data suggest that cTn elevation, in whatever context, may always be indicative of increased risk of events.
Conclusion
cTn assays facilitate the rapid exclusion of MI in patients presenting to acute medical services with chest pain. However as the assays have become more sensitive, cTn values above the ULN are frequently being seen in clinical scenarios not usually associated with MI. This often occurs as a result of a significant physiological insult and as such is particularly pertinent to the ICU environment. The interpretation of cTn results in ICU is particularly challenging because patients are frequently unable to communicate their symptoms and also because the manufacturers reference range is based on a healthy reference population. Clinicians within ICU should therefore carefully consider the clinical scenario and ECG findings when evaluating an elevated cTn level. In particular it should not be assumed that an abnormal result means T1MI. Whilst the data demonstrate that the majority of these patients have suffered a T2MI or myocardial injury, the data also increasingly suggest that these diagnoses are associated with adverse outcomes. It is therefore possible that cTn could provide clinicians with useful prognostic data during each ICU admission. However at this stage further research is required to: (a) more clearly define the expected cTn levels within ICU and (b) assess whether hs-cTn assays will provide a marker of prognosis.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JH: Travel sponsorship: Bayer. MM: no disclosures. MPWG: Serves on the medical advisory board of Sphere Medical Ltd. and is a director of Oxygen Control Systems Ltd. He has received honoraria for speaking for and/or travel expenses from BOC Medical (Linde Group), Edwards Lifesciences and Cortex GmBH. NC: unrestricted research grants from: Boston Scientific; Haemonetics; Heartflow; Beckmann Coulter. Speaker fees/consultancy from: Haemonetics, Abbot Vascular; Heartflow; Boston Scientific. Travel sponsorship – Biosensors, Abbot, Lilly/D-S; St Jude Medical, Medtronic.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.