
Abstract
Purpose:
The aim of this study was to assess the determinants and prognostic value of high-sensitivity cardiac troponin T peak plasma concentration in intensive care unit patients with non-cardiogenic shock.
Material and methods:
A prospective observational cohort study was conducted in a single intensive care unit between November 2014 and December 2015.
Results:
During the study period, 206 patients were hospitalized in the intensive care unit for non-cardiogenic shock and the median peak high-sensitivity cardiac troponin T was 55.1 [24.5–136] pg/mL. A multivariate analysis combining all variables showed that higher body mass index (t = 2.52, P = 0.01), lower left ventricular systolic function (t = −2.73, P = 0.007), higher white blood cell count (t = 3.72, P = 0.0001), lower creatinine clearance (t = −2.84, P = 0.0005), higher lactate level (t = 2.62, P = 0.01) and ST-segment depression (t = 3.98, P = 0.0001) best correlated with log10-transformed high-sensitivity cardiac troponin T peak plasma concentration. After multivariate analysis, the high-sensitivity cardiac troponin T peak was not associated with a significant reduction of in-hospital mortality (adjusted odds ratio = 0.99 (95% confidence interval: 0.93–1.02)).
Conclusion:
High-sensitivity cardiac troponin T elevation was very common in patients hospitalized for non-cardiogenic shock. The factors significantly associated with high-sensitivity cardiac troponin T peak plasma concentration were higher body mass index, decreased left ventricular systolic ejection fraction, higher leucocyte count, decreased renal function, increased lactate level, and ST-segment depression. The high-sensitivity cardiac troponin T peak was not significantly associated with in-hospital mortality in this setting.
Introduction
Increased plasma concentration of cardiac troponin (cTn) is a very sensitive and specific marker of myocardial damage. 1 Studies have shown that increased plasma concentration of cTn is frequently encountered in intensive care unit (ICU) patients.1,2More widespread use of highly sensitive cTn assays has led to a substantial increase in the detection of elevated levels of cTn. 3 In patients hospitalized in ICU, myocardial damage is rarely caused by spontaneous coronary artery occlusion (i.e. type 1 acute myocardial infarction). 4 Many hypotheses have been put forward to explain cTn elevation in ICU patients: imbalance between oxygen supply and oxygen demand during shock or respiratory failure (i.e. type 2 acute myocardial infarction or ischaemic imbalance),5,6 direct damage caused by endotoxins, microvascular coagulation dysfunction; renal insufficiency;7,8 left ventricular diastolic dysfunction; and right ventricular dilatation. 9 Studies have evaluated determinants of cTn elevation in general population, 10 in acute ischaemic stroke, 11 in respiratory failure, 12 and in cardiology. 13 One study did evaluate determinants of high-sensitivity cardiac troponin T (hs-cTnT) elevation in ICU patients with shock, but the analysis focused strictly on septic patients and on echocardiographic data. 9 The aim of this study was to assess the determinants and prognostic value of hs-cTnT peak plasma concentration in ICU patients with non-cardiogenic shock (N-CS).
Material and methods
This observational study was approved by the local Ethics Committee of Félix Guyon University Hospital (R14008). Written informed consent was obtained from patients or from their legally authorized representative. Reporting of this study conforms to ‘the Strengthening the Reporting of Observational studies in Epidemiology’ recommendations statement for reporting. 14
Selection of the study sample
This prospective observational cohort study was conducted between November 2014 and December 2015 in a single 23-bed mixed medical/surgical ICU at a French university hospital. Established criteria for the diagnosis of N-CS were as follows:15,16 (1) vasopressors required despite adequate fluid loading to achieve a mean blood pressure >65 mmHg; (2) absence of elevated left ventricular filling pressures on transthoracic echocardiography assessed with the presence of 2 the 3 following criteria: E-wave velocity (E)/lateral early diastolic mitral annulus velocity >14, peak tricuspid regurgitation velocity >2.8 m/s, and left atrial maximal volume index >34 mL/m2; (3) signs of impaired organ perfusion; and (4) absence of positive inotropes agents like dobutamine, dopamine, adrenaline, levosimendan, phosphodiesterase-3 inhibitors, and isoprenaline. Non-inclusion criteria were as follows: inability to obtain informed consent; hospitalization for chest trauma, cardiac arrest, presence of extracorporeal membrane oxygenation; hospitalization after cardiac surgery and surgery with cardiopulmonary bypass.
Upon admission, hs-cTnT was systematically measured every 8 h in all patients during 24 h. Blood samples were analysed using a Cobas Roche hs-cTnT assay (Basel, Switzerland).
Data collection
Patient characteristics and comorbidities were recorded on admission. Electrocardiography was systematically performed within 24 h of admission. The following elements were recorded: heart rate; rhythm; ST-segment depression or elevation >0.5 mm, prominent T-wave flattering or inversion >1 mm, and Q wave ≥0.03 s and ≥0.01 mV deep in at least two contiguous leads; and left bundle branch block.
Transthoracic echocardiography was also systematically performed within 24 h of admission. Transthoracic echocardiography examinations were performed by two experienced operators (J.A. and N.A. who already performed more than 2000 examinations) licensed in echocardiography and blinded to the context and clinical data. The following elements were recorded: left ventricular systolic ejection fraction using the monoplane modified Simpson’s rule; left ventricular end-diastolic diameter (mm/m2), interventricular septal thickness (mm) mitral, Doppler patterns with mitral inflow E-wave velocity (E), A-wave velocity (A), and lateral early diastolic mitral annulus velocity measured by tissue Doppler imaging (Ea); right ventricular dilatation assessed by a right ventricular end-diastolic area/left ventricular end-diastolic area ratio >0.6; 17 right ventricular systolic dysfunction assessed by tricuspid annular plane systolic excursion < 17 mm. 18
Outcome measures
The primary endpoint was hs-cTnT plasma peak in ICU patients with N-CS. The secondary endpoint was in-hospital mortality.
Statistical analysis
Results are expressed as total numbers (percentages) for categorical variables and median [25th–75th percentiles] for continuous variables, as appropriate. Continuous variables were compared using the unpaired Student’s t test or the nonparametric Mann–Whitney test, as appropriate. Categorical variables were compared using the Chi-square test or the Fisher’s exact test, as appropriate. Values of hs-cTnT with exponential distribution were log10-transformed for linear analyses. Pearson’s rank correlation coefficient analysis was performed to assess the correlation between log10 (hs-cTnT) plasma peak concentration and continuous variables. Second, the variables independently correlating with log10 (hs-cTnT) P < 0.1 were entered into a multivariate logistic regression analysis. Furthermore, risk factors of in-hospital mortality in bivariate analysis with P < 0.1 were entered into a multivariate logistic regression analysis using backward selection with P < 0.05. Colinearity between independent risk factors was tested; in cases of colinearity between risk factors, the most clinically relevant factor was selected to construct the multivariate models. The receiver operator characteristic curve was constructed to evaluate the capacity of hs-cTnT peak plasma concentration to predict in-hospital mortality. Analyses were performed using SAS statistical software (8.2, Cary, NC, USA).
Results
Patient characteristics
During the study period, 323 patients were admitted to the ICU for N-CS; 117 patients were excluded from the analysis; 12 for cardiac arrest, 39 for receiving extracorporeal membrane oxygenation, 2 for chest trauma, and 62 for hospitalization after cardiac surgery. The remaining 206 patients constituted the cohort (Figure 1).

Selection of the study sample.
The main characteristics of the patients are presented in Tables 1 and 2.
Characteristics of the 206 patients.
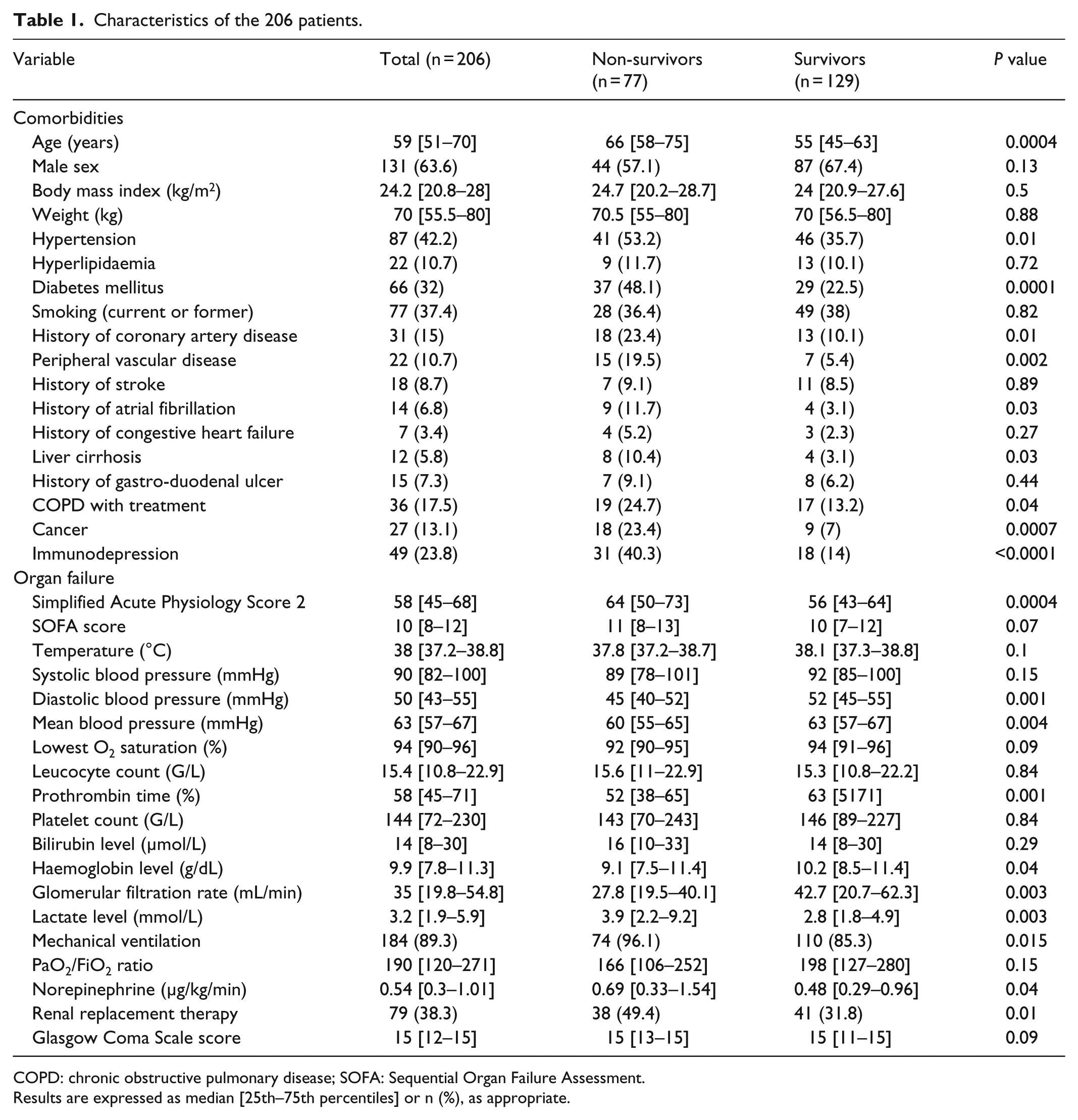
COPD: chronic obstructive pulmonary disease; SOFA: Sequential Organ Failure Assessment.
Results are expressed as median [25th–75th percentiles] or n (%), as appropriate.
Cardiologic features at inclusion.

Results are expressed as median [25th–75th percentiles] or n (%), as appropriate.
The median age of the patients was 59 [51–70] years old, with a mean Simplified Acute Physiology Score 2 of 58 [45–68]. The main aetiology of N-CS was septic shock in 148 cases (71.8%) and haemorrhagic shock in 15 cases (10.1%).
Determinants of hs-cTnT elevation
The median peak plasma concentration of hs-cTnT was 55.1 [24.5–136] pg/mL. After univariate analysis, hs-cTnT plasma peak concentration was associated with a P value <0.1 for older age, higher body mass index, hypertension, diabetes mellitus, higher Simplified Acute Physiology Score 2, higher Sequential Organ Failure Assessment score, lower diastolic blood pressure, lower mean blood pressure, higher leucocyte count, lower prothrombin time, lower platelet count, lower haemoglobin level, lower glomerular filtration rate, higher lactate level, renal replacement therapy, higher heart rate, ST-segment depression, lower left ventricular ejection fraction, and lower tricuspid annular plane systolic excursion (Tables 3 and 4).
Clinical characteristics correlated with log10 high-sensitivity cardiac troponin T.
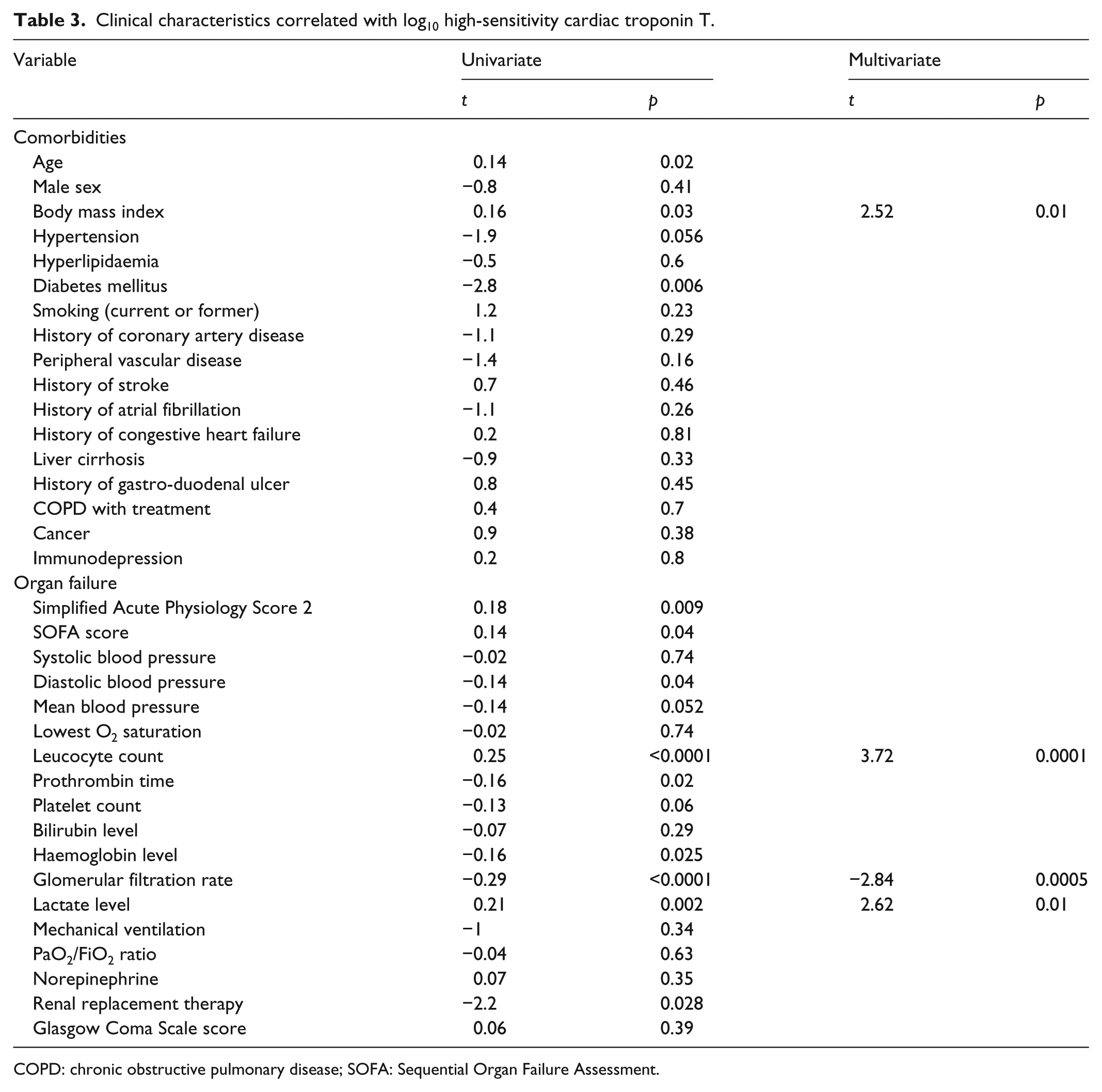
COPD: chronic obstructive pulmonary disease; SOFA: Sequential Organ Failure Assessment.
Cardiologic features correlate of log10 high-sensitivity cardiac troponin T.

After univariate analysis, patients with hs-cTnT plasma peak concentration >14 pg/mL were older (P = 0.0045), had higher Sequential Organ Failure Assessment score (P = 0.048), lower left ventricular ejection fraction (P = 0.016), and lower glomerular filtration rate (P < 0.0001) than patients with hs-cTnT plasma peak concentration <14 pg/mL.
A multiple multivariate analysis showed that hs-cTnT plasma peak concentration was independently associated with higher body mass index, higher leucocyte count, lower glomerular filtration rate, higher lactate level ST-segment depression and lower left ventricular ejection fraction (Tables 3 and 4).
In-hospital mortality
The in-hospital mortality rate was 37.4%. A univariate analysis revealed that the peak plasma concentration of hs-cTnT was associated with a higher in-hospital mortality rate (the peak plasma concentration of hs-cTnT was 50.1 [20.9–121.3] ng/L in survivors and 67.4 [32.4–167] ng/L in non-survivors, P = 0.03). The other risk factors found to be predictive of in-hospital mortality (based on a bivariate analysis with P < 0.1) are presented in Tables 1 and 2. The receiver–operator characteristic curve did not show an optimal threshold value of hs-cTnT peak plasma concentration for the prediction of in-hospital mortality (area under the receiver operator characteristic curve was 0.592, 95% confidence interval (CI): 0.514–0.670) (Figure 2).

Receiver operator characteristic curve of hs-cTnT for the prediction of in-hospital mortality.
After multivariate analysis, the peak plasma concentration of hs-cTnT was not associated with a higher in-hospital mortality rate (P = 0.085). In-hospital mortality was independently associated with older age (per year increment) (////odds ratio (OR): 1.075; 95% CI: 1.041–1.109, P < 0.0001), higher lactate level (OR: 1.135; 95% CI: 1.027–1.255, P = 0.001), mechanical ventilation (OR: 5.247; 95% CI: 1.224–22.499, P = 0.03), and lower left ventricular ejection fraction (OR: 0.966; 95% CI: 0.936–0.936, P = 0.03) (Table 5). The Hosmer–Lemeshow goodness-of-fit test showed good calibration of the model (P = 0.977). The Nagelkerke and Cox/Snell R squares were 0.306 and 0.224, respectively.
Multivariate analysis of risk factors associated with in-hospital mortality.
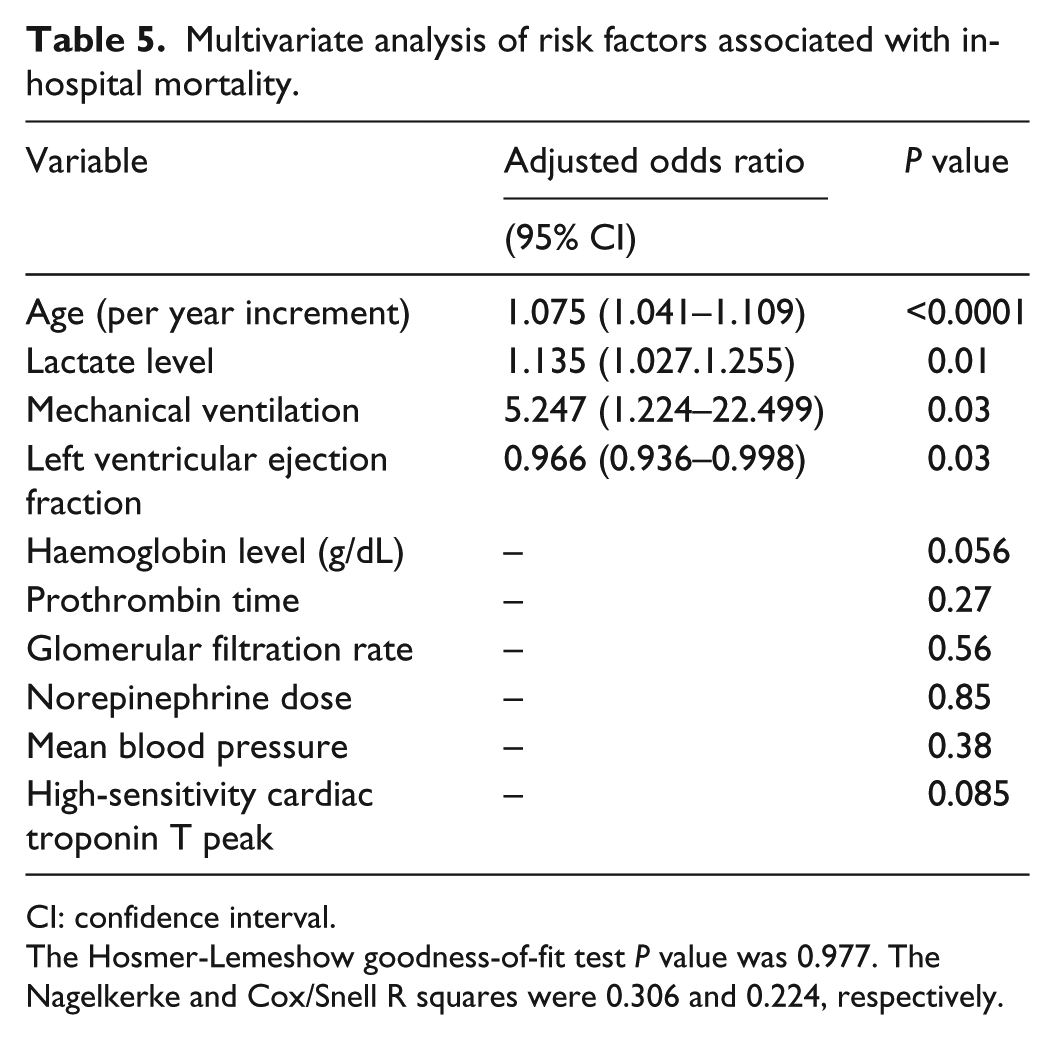
CI: confidence interval.
The Hosmer-Lemeshow goodness-of-fit test P value was 0.977. The Nagelkerke and Cox/Snell R squares were 0.306 and 0.224, respectively.
Discussion
The main results of this study were as follows: (1) hs-cTnT elevation was very common in patients hospitalized in ICU for N-CS; (2) in this context, the factors significantly associated with hs-cTnT peak plasma concentration after multivariate analysis were higher body mass index, decreased left ventricular systolic ejection fraction, higher leucocyte count, decreased renal function, increased lactate level, and ST-segment depression on the electrocardiogram; (3) the peak plasma concentration of hs-cTnT was not associated with an increase in in-hospital mortality after multivariate analysis.
The incidence of hs-cTnT elevation (88.9%) was high in our study, as was that reported by Landesberg et al. 9 in patients hospitalized for septic shock (73%). Detection of myocardial necrosis is more frequent with biological methods that measure hs-cTnT than with older methods. 3 Thus, the reported incidence of myocardial necrosis is below 50% in studies that use more conventional methods of cTn measurement.1,15,17,19 We noted a significant correlation between hs-cTnT elevation and a decrease in the glomerular filtration rate – which is a well-established association.9,10,20 We also found a significant correlation between rise in body mass index and hs-cTnT elevation that might be explained by the fact that cardiac mass increases with body mass. This association was already observed in the study by Wallace et al., 10 who also evaluated the factors linked to cTn elevation, but in a general population. The correlation between leucocyte increase and hs-cTnT elevation may have been related to an inflammatory response secondary to myocardial necrosis with an elevation of circulating plasma cytokines. 21 Similarly, we found a significant association between decreased systolic left ventricular function and elevated hs-cTnT. In cases of septic shock, which concerned a large proportion of patients in our study, systolic left ventricular dysfunction is often present; it is generally reversible and associated with cTn elevation, whose pathophysiological mechanisms are multiple. 22 Likewise, the association between ST-segment depression on the ECG and hs-cTnT elevation, already observed in the study by Faiz et al., 11 may be a marker of type 2 myocardial infarction. We found a positive correlation between hs-cTnT elevation and plasma lactate level that may have been related to myocardial necrosis secondary to an imbalance between oxygen supply and oxygen demand during shock, bleeding, or acute respiratory failure (type 2 myocardial infarction). Unlike Landesberg et al., 9 we did not find a significant relationship between hs-cTnT elevation and right ventricular dilatation or diastolic dysfunction after multivariate analysis. This may be due to a lack of power in our study, to differences in the two study populations, or to the fact that Landesberg et al. 9 primarily examined the correlation between echocardiographic parameters and hs-cTnT elevation, and that they analysed fewer clinical and biological parameters than we did.
The peak plasma concentration of hs-cTnT was associated with in-hospital mortality after univariate analysis, but not after multivariate analysis (P = 0.085). It is possible that the study is underpowered while only 206 patients were prospectively evaluated and the lack of difference in mortality could be due to a type II statistical error. Previous studies found that level of peak plasma concentration of cTn was associated with in-ICU mortality.1,6,23 In the study by Landesberg et al., 9 who focused on hs-cTnT elevation in septic shock patients, hs-cTnT was associated with in-hospital mortality after univariate analysis, but not after multivariate analysis.
This study has several limitations. It is a single-centre observational study, and no direct causal relationship can be established between isolated variables and hs-cTnT elevation. We collected data from only one transthoracic echocardiography per patient, we did not have access to echocardiographic parameters before ICU admission and we could not collect all data on echocardiography. We did not find significant relationship between hs-cTnT elevation and E/Ea ratio or diastolic dysfunction, and this could be related to the fact that we have excluded patients with elevated left ventricular filling pressures. As a result, the clinical implications of our findings remain uncertain.
Conclusion
hs-cTnT elevation is very common in patients hospitalized for N-CS. The causes for this elevation are multiple (decreased renal elimination of hs-cTnT, inflammation, myocardial necrosis due to inflammation, etc.) and in this context, hs-cTnT elevation does not appear to have any prognostic value.
Footnotes
Acknowledgements
Drs Allou, Caujolle had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Allou, Allyn, Caujolle, Vandroux, Martinet, Brulliard. Acquisition of data: Caujolle, Allou, Allyn, Valance. Analysis and interpretation of data: Allou, Allyn, Caujolle, Vandroux, Martinet, Brulliard, Jabot, Valance. Drafting of the manuscript: Allou, Allyn, Vandroux, Martinet, Brulliard. Critical revision of the manuscript for important intellectual content: Allou, Allyn, Caujolle, Vandroux, Martinet, Brulliard. Statistical analysis: Allyn, Allou. Administrative, technical, or material support: Vandroux, Martinet, Brulliard. Study supervision: Allou, Allyn, Vandroux, Martinet, Brulliard.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the local Ethics Committee of Félix Guyon University Hospital (R14008).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was internally funded. Support was provided solely from institutional and/or departmental sources.
Informed consent
Written informed consent was obtained from patients or from their legally authorized representative.