
Abstract
Treatment in an intensive care unit can be life-saving but it can be distressing and not every patient can benefit. Decisions to admit a patient to an intensive care unit are complex. We wished to explore how the decision to refer or admit is experienced by those involved, and undertook a systematic review of the literature to answer the research question: What are the experiences of health care professionals, patients, and families, of the process of referral and admission to an intensive care unit? Twelve relevant studies were identified, and a thematic analysis was conducted. Most studies involved health care professionals, with only two considering patients' or families' experiences. Four themes were identified which influenced experiences of intensive care unit referral and review: the professional environment; communication; the allocation of limited resources; and acknowledging uncertainty. Patients' and families' experiences have been under-researched in this area.
Introduction/background
Treatment in an intensive care unit (ICU) is known to improve survival rates for critically ill patients,1,2 with timely admission associated with better outcomes. 3 Care provided in an ICU is expensive and resource-intensive, and pressure on ICU resources is a daily occurrence in the NHS. This has implications for care, and patients who would benefit from ICU care may not always receive it. However, many patients do not survive ICU, 4 and admission to ICU can be associated with significant morbidity, both during their admission and for many years after discharge. 5
The decision whether to refer/admit a patient to ICU can be a difficult clinical and ethical challenge, and the impact of making these decisions on health care providers (HCPs), patients, and families can be considerable. Currently in the UK, there is no nationally used guidance for HCPs regarding referral or admission of patients to ICU.
Numerous quantitative studies have investigated specific factors affecting the decision to refer or admit a patient to ICU.6–10 Our aim in this review was to explore what is currently known about how the process of decision-making for referral/admission to ICU is experienced by patients, families, and HCPs.
Methods
We conducted this review (PROSPERO 2015:CRD42015019714) concurrently with a review of the literature on factors affecting the decision to refer or admit a patient to intensive care (PROSPERO 2015:CRD42015019711), as part of a large mixed methods study, funded by the National Institute for Health Research, which explored the decision-making process around referral and admission to ICU. One search was used for both reviews. We sourced papers from Medline, Embase, and ASSIA, all sections of the Cochrane Library, CINAHL, PsychINFO, and Web of Science in addition to Dissertation abstracts online, Index to theses, Open Grey. The search strategy was informed by an initial scoping review of the literature, and used a combination of the following MeSH headings and keywords: 1. Critical and intensive care, intensive care units and critical illness; 2. Patient admission, transfer, triage, and refusal to treat; 3. Professional decision-making and judgement, professional–family relations, choice behavior, and medical futility (See appendix 1). We included papers published between 1980 and 2015 describing empirical research that focused on the process of decision-making for referral or admission of adult patients to ICU. Papers that referred to neonates or pediatrics were excluded. The initial searches were run on 11 May 2015.
In March 2018, we updated the review to identify any relevant studies published since our initial searches. We searched PubMed using the search terms critical care/CCU or intensive care/ICU AND decision making AND admissions OR referrals. We hand-searched the contents of the six journals that had provided more than one included paper in our original review, from 1 May 2015 to 1 January 2018, and conducted forward and backward citation tracking on all identified papers as well as papers listed in a published review. 11
In total, we identified 34,343 abstracts, which were double screened by a team of 13 reviewers. This yielded 552 papers for further consideration, of which 12 publications (10 studies) were included as being relevant for this review (see Figure 1). One of these publications was found in the March 2018 update.
12
Two independent reviewers (AS, SR) assessed the quality of the studies using May and Pope's criteria for appraising qualitative research.
13
Disagreements were resolved by reference to a third reviewer (FG). We extracted qualitative data relevant to our research question from each study and conducted a thematic analysis14–16 in NVivo on the collated data.
PRISMA diagram.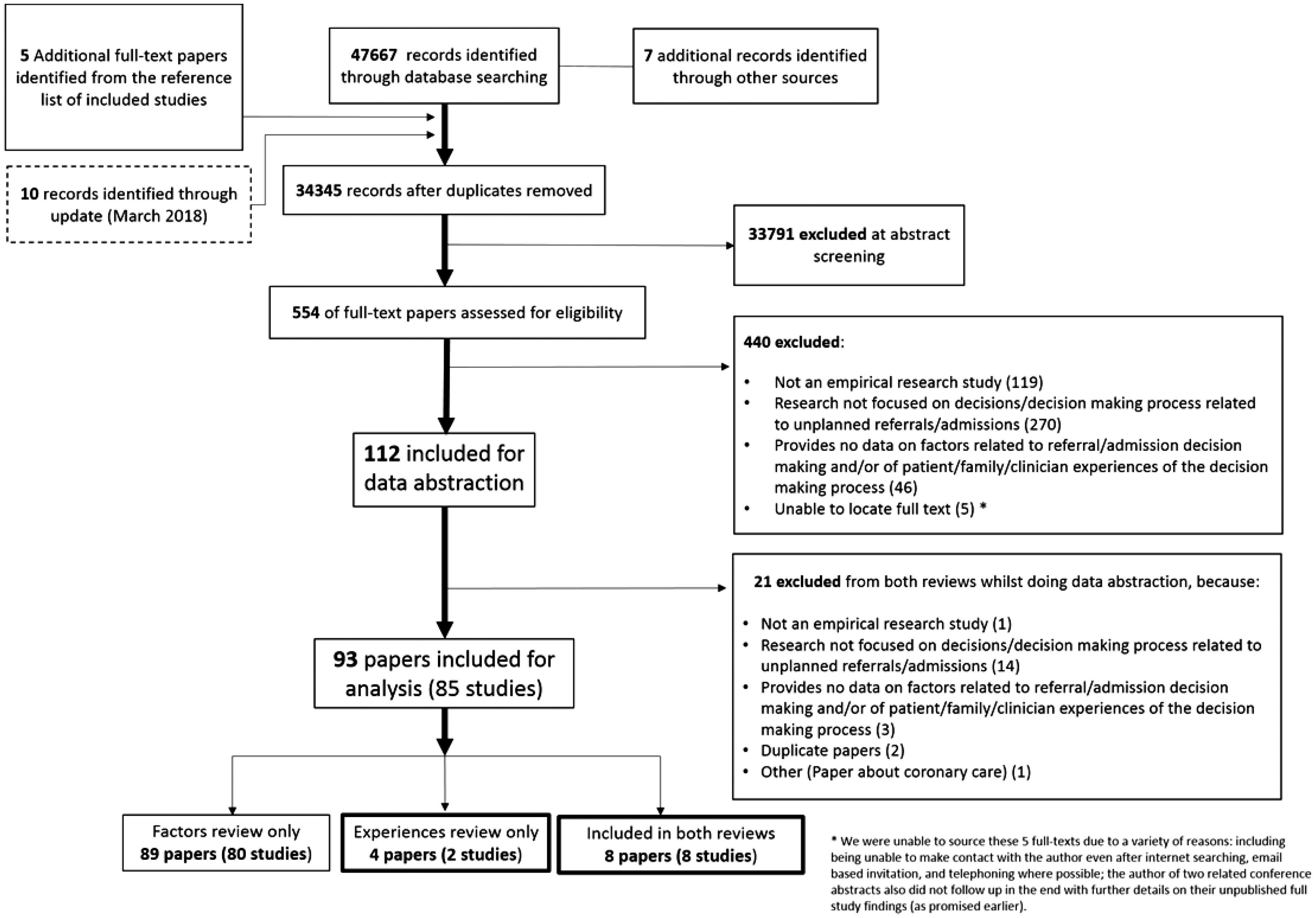
Results
Studies reviewed.
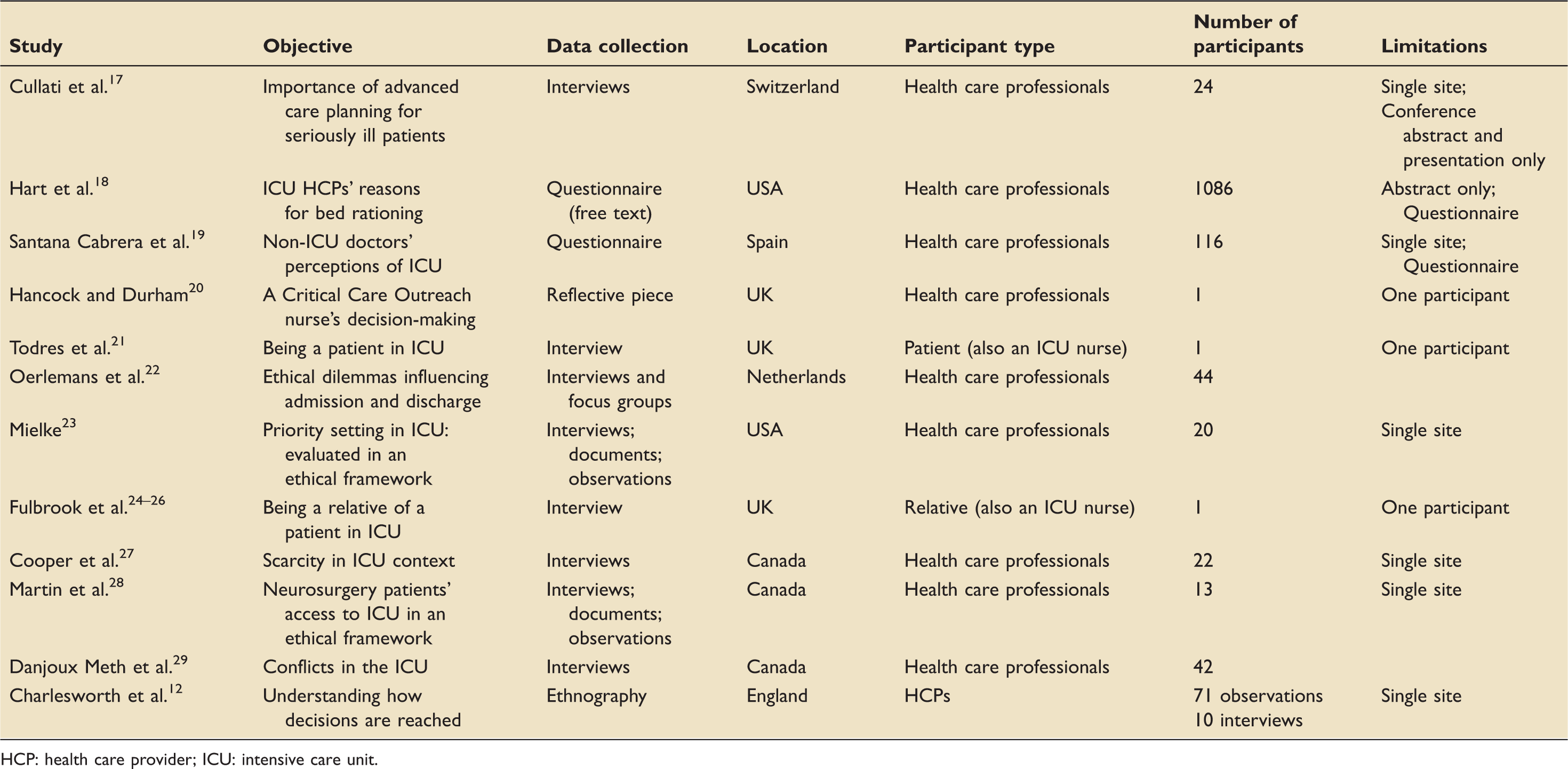
HCP: health care provider; ICU: intensive care unit.
Nine studies considered the experiences and perspectives of health care professionals and two described the experience of being a patient and relative respectively, each from a single person's perspective.
Two studies12,20 focused specifically on experiences of the process of referral and admission to ICU, but we were able to identify data relevant to our research question from each paper.
The quality of the literature reviewed was mixed (see Table 1 for limitations of the studies). Sampling and data collection methods were not explicitly described in some studies, but the iteration between data and analysis was generally considered good. Of the twelve identified studies, nine were single site.
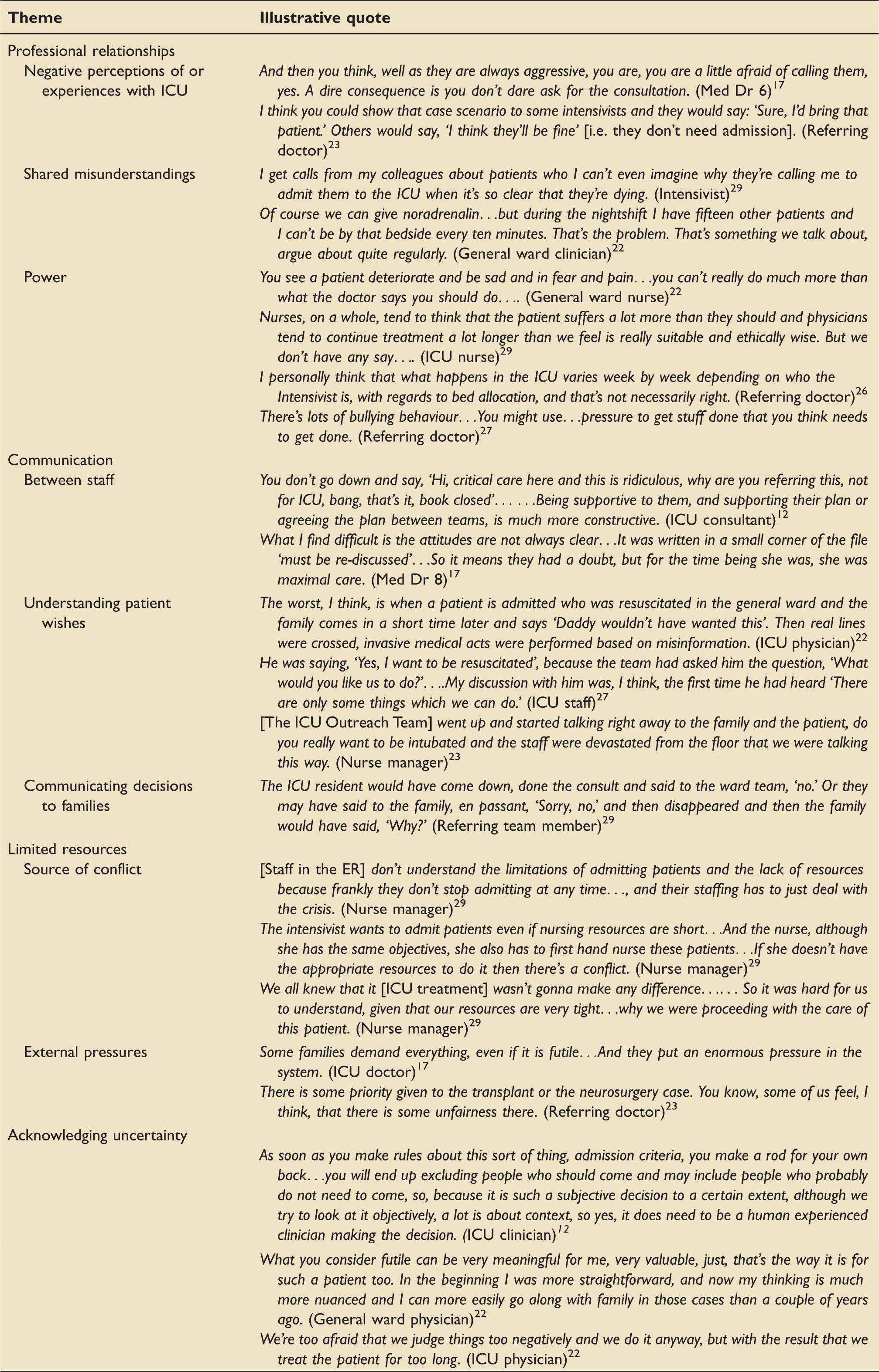
Illustrative data.
Professional relationships
Several studies described tensions between referring staff and ICU staff with referring staff regarding ICU as unapproachable, a perception that in some instances influenced their decision whether to refer a patient.
Terms such as “arrogant”, “ivory tower”, and “island” were used often. 22
In a survey 19 of referring doctors (116 senior doctors and 41 juniors), 44% of each group reported instances where they had decided not to refer a patient who they believed would benefit because they thought that they would be refused admission. This was reflected in the qualitative data 17 (see Table 2).
Referring doctors expressed frustration about inconsistency of decision-making between ICU doctors,23,27 and reported dissatisfaction with reasons given for nonadmission. 19 A key source of tension appeared to be a shared misunderstanding of each others perspectives. ICU doctors thought ward staff did not understand what ICU could offer and complained about inappropriate referrals, while non-ICU staff felt that ICU clinicians did not understand the challenges of caring for a very unwell patient on a ward with many patients and limited nursing staff.22,29 Some non-ICU clinicians incorrectly thought ICU had hard criteria for who should be admitted. 23
Participants in several studies described the ideal approach as collaborative and involving all clinicians working together to reach the best outcome for this patient. 22 However, the extent to which ICU doctors felt a duty to patients for whom they were not directly responsible for varied.
Referring doctors, ICU doctors, and nurses described sometimes experiencing a lack of power or urgency in these situations. Referring doctors saw ICU doctors as setting the rules (criteria) for admission but also described exerting pressure themselves to force an admission decision. 27 ICU doctors described pressure from patients' families and organizational constraints limiting their freedom to make what they considered the best decision for their patient. 19 Both ICU and ward nurses experienced frustration that they had little influence on decisions (or nondecisions), which they saw as adversely affecting their patients.22,29 However, the study exploring the experience of a single critical care outreach nurse 18 suggested that in this role the nurse had more authority to make decisions and have her views respected.
Communication
The need for open discussion between the ICU and ward teams was viewed as crucial for a good referral process but this was not always the experience of participants in the studies. 22 One study also reported a lack of discussion between ICU doctors with decisions being made in isolation. 23 In contrast, the authors of an ethnographic study observed few cases of solitary decision-making among ICU clinicians in a single hospital. 12 The ICU doctors participating in this study suggested that a more collegial approach to decision-making had developed at their hospital in recent years following an initiative to encourage this.
Lack of communication with patients and their family prior to a referral to ICU was seen as making the decision whether to admit to ICU more difficult,19,22,27 and examples were given where discovery of a patient's wishes or views after they had been admitted to ICU caused distress for the ICU team because treatment had been given that the patient would not have wanted.22,27
Different perspectives on discussing with patients and families the options for and potential outcomes of ICU treatment were described within the studies. In one study, an ICU doctor described frustration that ward staff often give patients and families false hope about the benefits of ICU treatment for patients, 27 while another study described the ward staff's discomfort when the ICU outreach team described interventions in explicit detail to patients. 29
In the paper exploring a patient's experience of being critically unwell she described feeling excluded from the decision-making process. A registrar arrived together with a number of other doctors and nurses and Anne [patient] began to wonder what was going on…. no one was talking to her at this stage. They were talking to one another and appeared worried about her.
21
Limited resources
Resources were seen as a common source of stress and conflict around ICU admission decisions.19,29 Delayed or canceled elective surgery due to a shortage of post-surgery ICU beds led to frustration for patients and families, as well as nurses and physicians on the general ward.19,22,29 There was a sense that some departments were not sympathetic to the problem of ICU bed shortages. Some specialties or types of patient, were perceived as receiving priority for ICU admission when beds were limited, for example if the hospital had a large transplant programme this might result in prioritization of transplant patients as an organizational policy. ICU doctors experienced this as unfair to other patients.23,27 A further pressure to admit in the face of limited beds came from referring doctors and patients' families. 19
ICU doctors sometimes admitted patients whom ICU nurses subsequently felt unable to care for properly because of limited resources creating inter-professional conflict.19,29 These conflicts were exacerbated when nursing staff felt that the ICU treatment they were struggling to deliver was inappropriate or futile, leading to frustration and distress.22,29
One study noted that availability of ICU beds influenced how decisions were made regarding admission such that the clinical threshold for admission would change. This was acknowledged as potentially unfair but a pragmatic response to make the best use of resources. 12
Acknowledging uncertainty
Doctors were not in favor of strict criteria for ICU admission, as they felt that this would exclude important contextual information which could influence the decision, and did not recognize the inherent uncertainty in these decisions. 12 Senior doctors described how over time they came to realize the difficulty of predicting a person's chances of recovering, and to understand that individual patient's values and perception of quality of life varied greatly. 22 When there was doubt about futility of treatment or the quality of life after treatment, doctors reported that they tended to admit a patient.19,22 However, they recognized that this could mean extra burden for patient for little or no benefit.
Discussion
There is very little published research exploring the experience of the process of referral and admission to ICU. Our review found only two studies where this was the primary focus: an ethnographic study 12 and an individual nurse's personal reflection on a single case. 18 Most studies did not include the perspective of patients or their families. This may reflect the ethical and methodological challenges involved in conducting studies in this context. Patients are likely to be too ill to take part and family members are focussed on the survival of their loved one rather than being interviewed. Clinical staff wish to protect patients and families from any unnecessary burden or distress, which may affect recruitment. However, given that involving patients and/or their families in decisions about their care is both a legal and moral requirement, 30 and that doctors in these studies described the clinical importance of good communication with patients and families, it is important that future research in this area considers how best to capture their perspectives.
From the limited data in the studies identified, the overall experience of health care professionals of this decision-making process appears to be shaped by professional relationships and attitudes, the quality of communication both between professionals and with patients and their families, the pressure created by limited resources, and the inherent uncertainty in the decision itself.
Our findings reflect research in other areas of medical decision-making. For example, team-working is viewed as a way of improving patient outcomes but team structure and team processes may facilitate or hinder its achievement in primary care. 31 Differential access to power within teams may cause nurses to feel unable to voice their opinion and contribute to decision-making in multidisciplinary teams. 32 Elsewhere, deficits in communication between GPs to secondary care negatively affected patient care. 33 Involving patients and relatives in care decisions is considered a standard of good practice 34 but this is not always achievable. A study of 51 doctor–family conferences about end-of-life treatment decisions in ICUs found that only one (2%) of the decisions met all 10 criteria for shared decision-making, highlighting how difficult it may be to include families in clinical decisions in ICU. In the same study, greater levels of shared decision-making were associated with better family satisfaction. 35
We identified power (or lack of it) as a cause of conflict and frustration in the process of decision-making around ICU referral and admission. For example, referring doctors perceived an unequal power balance in their interactions with ICU doctors. Organizational and resource constraints also caused ICU doctors to sometimes feel powerless to provide the right care for their patients. The concept of agency refers to the sense of control and autonomy, which an individual experiences in their everyday life, and which is mediated (and can be restricted) by social and institutional forces.36,37 When HCPs have to make ethically and emotionally difficult and complex decisions in the context of restricted agency, they can experience moral distress: feelings of guilt, anger, frustration, and distress engendered by the sense of being unable to practice in accordance with one's ethical standards. 38 The data here indicated that a number of HCPs participating in the studies had experienced moral distress in relation to ICU referral or admission decisions. High levels of moral distress correlate with high burnout rates and rapid job turnover, increasingly recognized in ICU professionals, 39 which in turn affects patient care and results in increasing costs.40,41 Nurses are particularly at risk of moral distress because they have little agency over a patient's treatment, and yet are very close to patient and witness their physical and emotional suffering.38,40,42,43 Improving the experience of HCPs involved in the process of referral and admission to ICU will involve understanding, preventing, and reducing moral distress.
One study 12 presented a more positive picture of the experience of the process than the other studies, particularly around communication and professional relationships. The authors comment that collegiate decision-making and improved communication had been the focus of an active strategy in the hospital studied. It is not clear whether this represents a broader change within ICU practice or is a specific feature in this site. However, it may reflect the increased focus on shared decision-making and multidisciplinary approaches to patient care that has taken place in health care more generally in recent years.
Strengths and weaknesses
A strength of our review is its systematic and inclusive approach so we can be confident that we have identified the key studies in this area. The studies identified include a range of health care settings and countries. The quality of the studies identified was mixed and none focussed specifically on our research question so relevant data were limited. A particular weakness is the paucity of studies considering the experience of this process from the perspective of patients or their family.
Future research
Our review has suggested that the process of decision-making around referral and admission to ICU could be improved and that attention to professional relationships, communication, and support for HCPs making decisions within a context of limited resources is required. However, further research is needed to explore the experience of this decision-making process more explicitly to explore these issues in more depth. There is a particular need for research to explore the experience of patients and families, their involvement in these decisions, and how communication and consultation with patients and families can be improved.
Supplemental Material
INC832185 Supplementary Appendix - Supplemental material for The experiences of health care professionals, patients, and families of the process of referral and admission to intensive care: A systematic literature review
Supplemental material, INC832185 Supplementary Appendix for The experiences of health care professionals, patients, and families of the process of referral and admission to intensive care: A systematic literature review by Sophie Rees, Frances Griffiths, Christopher Bassford, Mike Brooke, Zoe Fritz, Huayi Huang, Karen Rees, Jake Turner and Anne-Marie Slowther in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.