
Abstract
Introduction
Although improvement in survival from haematological malignancies has been reported, a substantial number of these patients develop life threatening complications. Critical care outreach services (CCOS) aim to avert inappropriate ICU admissions, while ensuring timely patient review.
Methods
We retrospectively analysed patients with haematological malignancy reviewed by an outreach service between January 2014 and December 2015 at a single institution. The aim of our study was to describe the patient population assessed by a well-established outreach team, identify predictors of ICU admission, as well as ICU and hospital mortality.
Results
Sixty of 126 patients reviewed (47.6%) were admitted to ICU. ICU and hospital mortality were 25.3% and 45.2%, respectively. The odds of being admitted to ICU was 13 times higher (p = 0.013) if the patient was referred for hypoxia, 20 times higher (p = 0.006) if they were referred for sepsis or 14 times higher (p = 0.027) if they were referred to CCOS for hypotension, compared to when the team was automatically alerted. The odds of not surviving hospital admission increased 1.27 times for every extra day of CCOS review (p = 0.02). When a patient was referred having a refractory or progressive haematological condition, the odds of not surviving to hospital discharge increased by four or 12 times, respectively, compared to when the referred patient was in remission. Receiving high flow nasal cannula oxygen (HFNCO) was associated with a reduction in ICU admission (p = 0.03), irrespective of the underlying diagnosis, performance status or location of delivery. The CCOS participated in end-of-life discussions in 29% patients.
Conclusions
ICU and hospital mortality of patients with haemato-oncological malignancy continue to improve. CCOS are heavily involved in the recognition and management of these patients, as well as in the facilitation of end-of-life discussions. Sepsis was associated with increased risk of ICU admission and mortality. Initiation of HFNCO outside ICU appears to be feasible and safe and was not associated with increasing risk in this single centre study.
Introduction
In the last decade, an improvement in survival from haematological malignancies (HMs) has been reported both in Europe and the US.1,2 However, despite recent advances, a significant number of patients with HM develop life threatening complications, requiring different levels of organ support and/or admission in an intensive care unit (ICU). As the stigma of dismal prognosis still accompanies these admissions, the triage policies differ among institutions and the percentage of critically ill patients eventually accepted in ICU varies between < 3% and > 70%.3–6 Not surprisingly, outcomes post-ICU admission equally vary, ranging from a historic survival rate of 2.5% 7 to more than 60% in recent studies, 5 with patients who present in multiple organ failure, faring much worse.8,9
Early, targeted intervention before ICU admission in critically ill haematology-oncology patients has been linked with decreased in-hospital mortality. 10 Furthermore, delaying ICU admission has been associated with increased mortality, 11 leading experts to advocate a change of practice and timely admission pathways for this patient population. 12 Despite these data, prompt ICU admission cannot always be achieved especially in the United Kingdom (UK), due to the constant bed capacity pressures. The significant variability in the number of ICU beds between Europe and the US has been noted before,13,14 with the UK having fewer (6.6) beds per 100,000 capita of population than all other European countries.
Critical care outreach services (CCOS) have been introduced into the UK National Health Service with the aim, among others, to avert inappropriate and ensure timely admission to ICU. 15 However, very few studies have assessed the effect of CCOS on the management and outcomes of patients with HM.10,16–18 The aim of this project was to describe the patient population assessed by a well-established outreach team, identify predictors of ICU admission, as well as ICU and hospital mortality in an exploratory analysis. Our hypothesis was that CCOS would play a paramount role in the management of these patients and that the interventions of the outreach team would not adversely impact on patient outcome.
Methods
A retrospective analysis was performed in patients with HM who were reviewed by the CCOS between January 2014 and December 2015 at King’s College Hospital NHS Foundation Trust. King’s College Hospital is a tertiary haemato-oncology centre with 60 inpatient hospital beds, performing more than 100 allogeneic and 120 autologous transplants per year. The department is an international centre for research and the treatment of myeloid leukaemias, lymphomas and myeloma, and has the first immune gene therapy programme for leukaemia approved by the Gene Therapy Advisory Committee. The CCOS is a seven-day, 24-h service that comprises a team of two ICU-trained nurses and a senior ICU trainee. A dedicated consultant is available five days a week 8 a.m.–6 p.m., with the out-of-hours service being supported by the ICU consultants on call.
The CCOS in the hospital gets involved in patient care either by direct referral from the ward teams or by responding to an increased National Early Warning Score (NEWS; supplied in the online Supplement). For scores > 4 the ward medical team is asked to review the patient, whereas if the score is > 6, the CCOS is alerted and a prompt review of the patient is carried out. Involvement of the team occurs either with a telephone call from the ward clinicians or with an electronic alert on the portable devices they are carrying (Ascom Myco™ Smartphone, Sweden). Depending on the initial assessment, the patient’s co-morbidities and the clinical trajectory, the team either gives advice to the ward staff or intervenes and gets directly involved in patient care. The latter consists of a range of actions, including advice on fluid and electrolyte management; diagnostic procedures; initiation of non-invasive respiratory support via application of high flow nasal cannula oxygen (HFNCO) or transfer to an ICU. HFNCO is delivered by the Fisher & Paykel Optiflow system, using the MR850 respiratory humidifier with MR290 chamber; RT241 heated delivery tubing, and RT033 or RT044 small or wide bore nasal cannulae (Fisher & Paykel Healthcare, Auckland, New Zealand). When the intervention is indicated, the initial standard settings are oxygen flow 60 L/min and adequate FiO2 to achieve SpO2 > 94%. In both situations, hourly monitoring and regular medical and nursing reviews are instituted until symptom resolution or decision to escalate treatment and ICU transfer. If the team believes that non-escalation of treatment is appropriate, then consideration of end-of-life (EoL) is offered to the parent team. All admission- and treatment limitation decisions are discussed with the on-duty consultant.
Data were collected by reviewing electronic and paper patient records and are presented in the online Supplement. Research Ethics Committee approval was not necessary and the study was endorsed by the Trust’s Service Evaluation Committee as an Audit Project. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
In the statistical analysis, the baseline characteristics of the patients who participated in the study were calculated. The Mann-Whitney U test was used to compare differences when the independent variable was continuous, whereas chi-square test was used for comparisons between the categorical variables. Logistic regression was performed to examine which variables influence ICU admission and hospital mortality using the backward elimination method. The variables were included in the multivariate analysis when a p value < 0.2 was observed in the univariate analysis. In the logistic regression model, the categories of independent variables with very low or no patient frequency joined the higher frequency categories, in order to assess the model. Survival analysis was applied between the patients who received HFNCO in ICU versus outside of ICU. Kaplan–Meier curve was used to visualize the results of the analysis. Relationships with a p value ≤ 0.05 were considered as statistically significant. All reported p values are two-sided. Data were analysed in the Statistical Package for the Social Sciences 23.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient demographics.
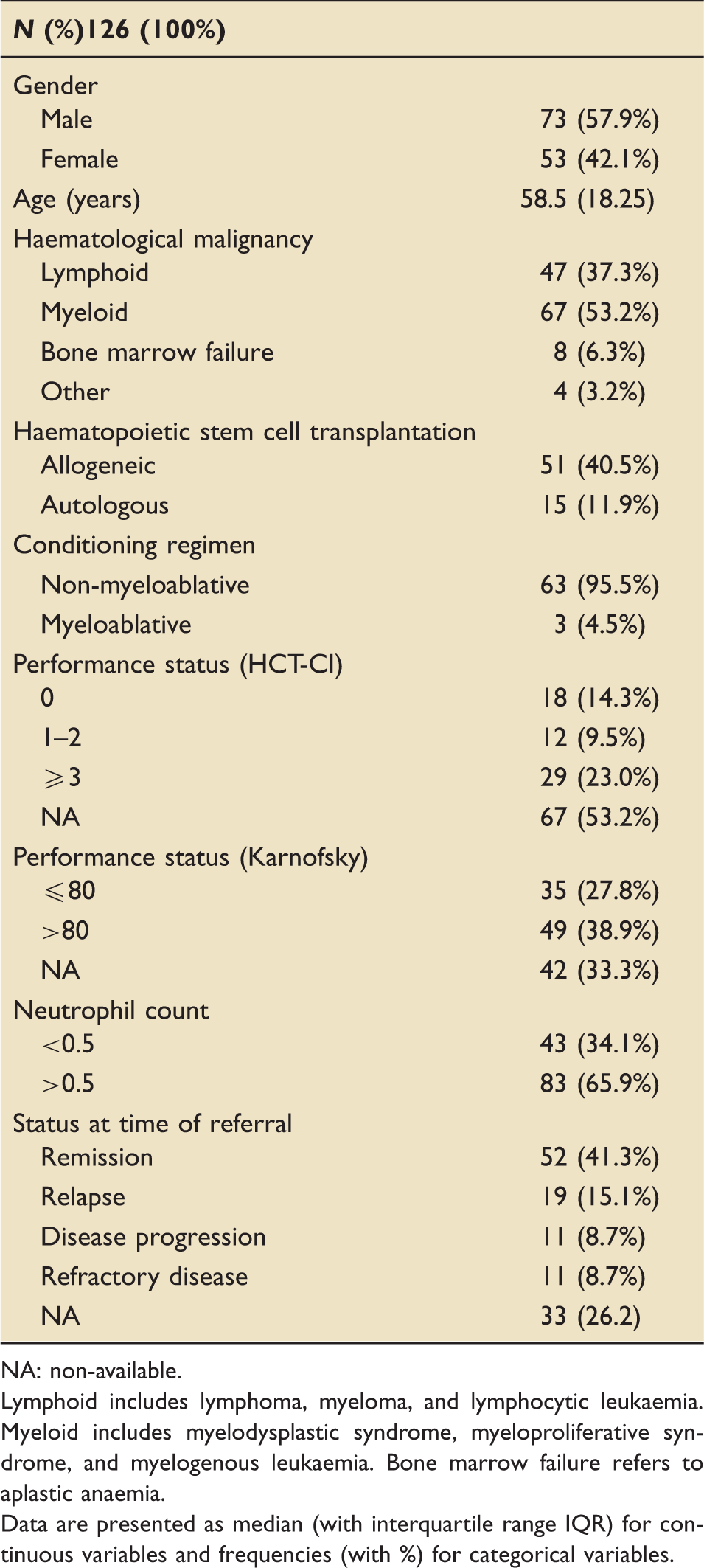
NA: non-available.
Lymphoid includes lymphoma, myeloma, and lymphocytic leukaemia. Myeloid includes myelodysplastic syndrome, myeloproliferative syndrome, and myelogenous leukaemia. Bone marrow failure refers to aplastic anaemia.
Data are presented as median (with interquartile range IQR) for continuous variables and frequencies (with %) for categorical variables.
Description of referrals to CCOS.
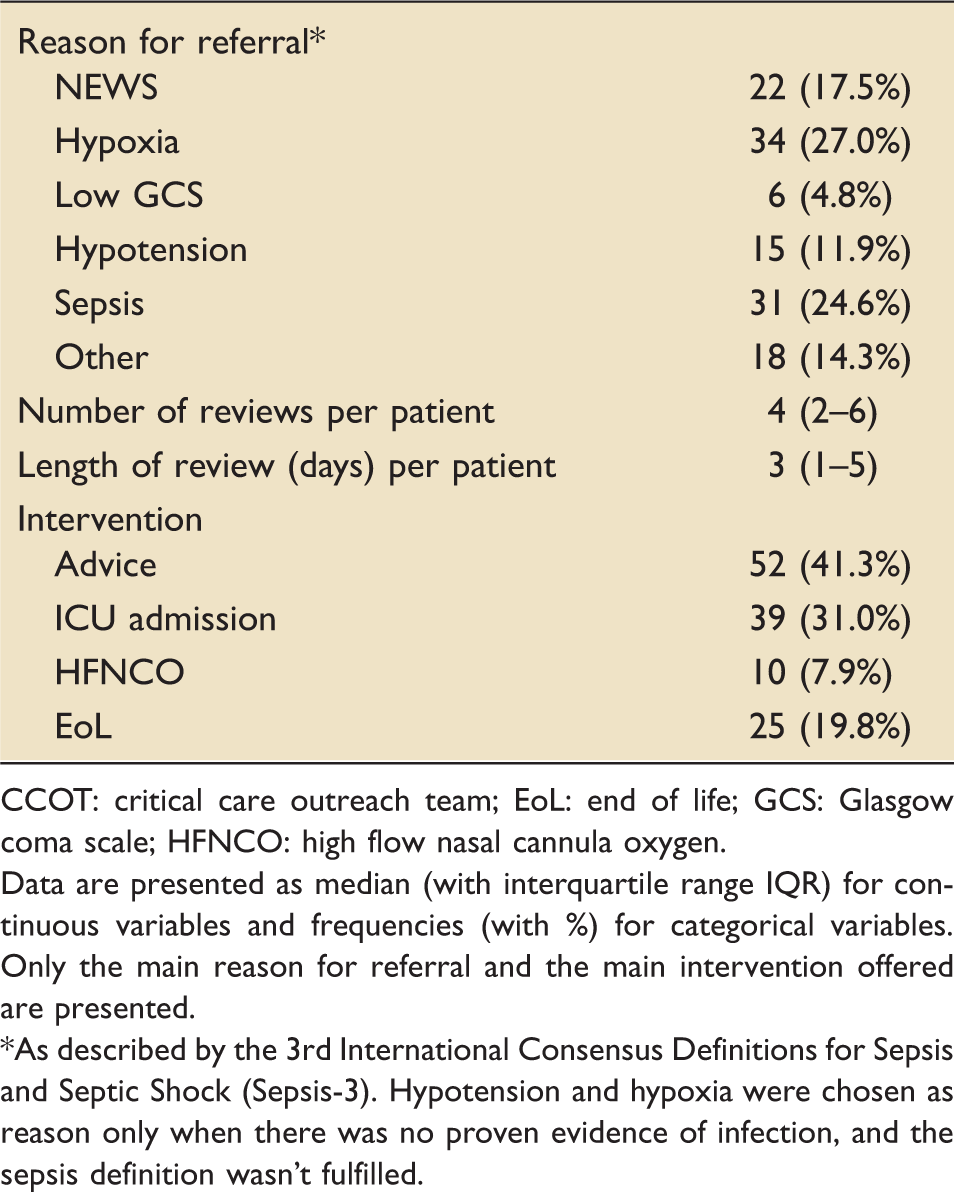
CCOT: critical care outreach team; EoL: end of life; GCS: Glasgow coma scale; HFNCO: high flow nasal cannula oxygen.
Data are presented as median (with interquartile range IQR) for continuous variables and frequencies (with %) for categorical variables. Only the main reason for referral and the main intervention offered are presented.
As described by the 3rd International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Hypotension and hypoxia were chosen as reason only when there was no proven evidence of infection, and the sepsis definition wasn’t fulfilled.
Predictors of ICU and hospital mortality
Analysis of variables influencing hospital mortality.
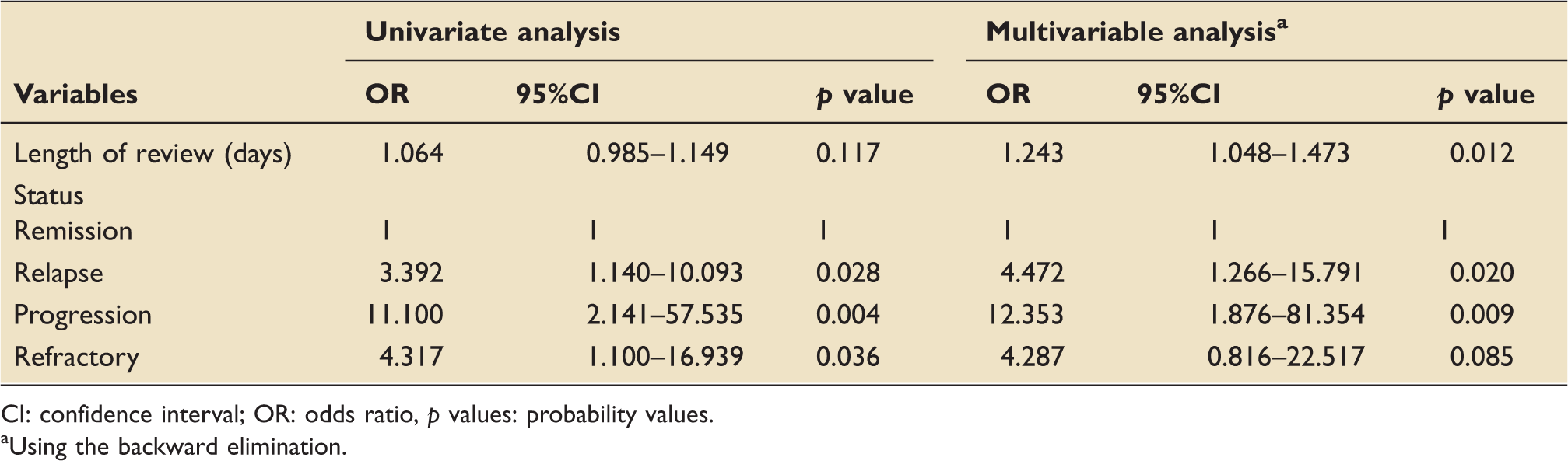
CI: confidence interval; OR: odds ratio, p values: probability values.
aUsing the backward elimination.
Predictors of ICU admission
Analysis of variables influencing ICU admission.
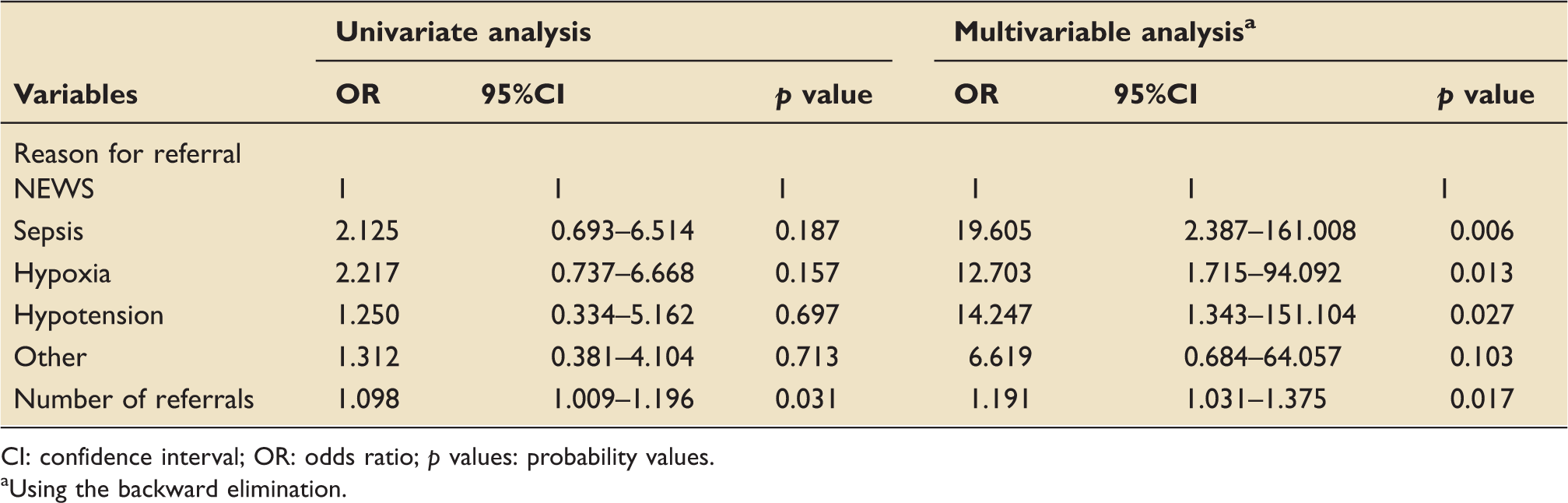
CI: confidence interval; OR: odds ratio; p values: probability values.
aUsing the backward elimination.
The CCOS was involved in the immediate ICU admission of 39 haemato-oncology patients, whereas further 21 patients entered the ICU later, after further reviews on the ward. When assessing the impact of this delayed admission on ICU and hospital mortality, no statistically significant difference was demonstrated between the two groups (p = 0.22 and p = 0.28 respectively).
Patients with HSCT
During the study period, 201 patients underwent allogeneic HSCT in the hospital with 51 of them being referred to the CCOS (25%); these 51 patients comprised the 40% of the total referral number. Two hundred and eleven patients underwent autologous HSCT in the same period in the hospital; 15 of them (7%) were reviewed by the CCOS, accounting for the 12% of the CCOS workload.
The most common reason for referral in the former group was respiratory failure (35%), with the second being sepsis (27%). Patients with an autologous transplant triggered predominantly (41%) an automatic review by the CCOS (i.e. the team were alerted by a high NEWS score but did not receive a ‘distressed’ telephone call by the ward team), whereas sepsis was also the second reason for referral (26%) in this group. ICU admission rates were higher in the allogeneic group, even after adjusting for type of malignancy and performance status, but this was found to be statistically non-significant (p = 0.073, 95%CI 0.016–1.20). Patients who underwent allogeneic HSCT also demonstrated a trend for higher ICU (33% vs. 12%) and hospital mortality (44% vs. 24%), p = 0.56 (95%CI 0.473–3.756) and p = 0.11, 95%CI 0.263–1.148) respectively. No statistically significant predictors were associated with the above outcomes.
No statistically significant difference was noted between patients who underwent HSCT and those who only received chemotherapy in any of the measured outcomes (ICU admission, mortality, hospital mortality).
Patients receiving HFNCO
From the 126 patients, 21 (17%) received HFNCO by the outreach services whilst still on the ward. From these, six had HFNCO as part of palliative care, and these data were not included in the analysis. Median time spent on HFNCO was two days (IQR 1–5), median PaO2/FiO2 on initiation was 220 mmHg and median PaO2/FiO2 while on HFNCO was 201 mmHg (IQR 99–254 mmHg), signifying mild to moderate acute respiratory failure. Having the intervention resulted in a reduction in ICU admission (p = 0.03, 95%CI 1.13–15.79), irrespective of the underlying diagnosis or performance status, with only three (20%) out of the 15 patients having to be admitted in ICU for escalation of support. ICU and hospital mortality did not differ between the patients receiving HFNCO and those who did not (p = 0.15 and p = 0.39), and neither did the length of review by the CCOS (p = 0.12). No statistically significant difference was found in hospital mortality between the patients who had the intervention on the ward and those who received it in ICU (Figure 1, p = 0.4). When looking whether the timing of the intervention in relation to HSCT (before/after) had an impact on ICU and hospital mortality, no statistically significant association was identified. Similarly, the number of days the patients spent on HFNCO did not appear to influence the need for ICU admission (p = 0.26).
Survival analysis of the patients who received HFNCO in ICU vs. outside of ICU. p = 0.4. r/v: review.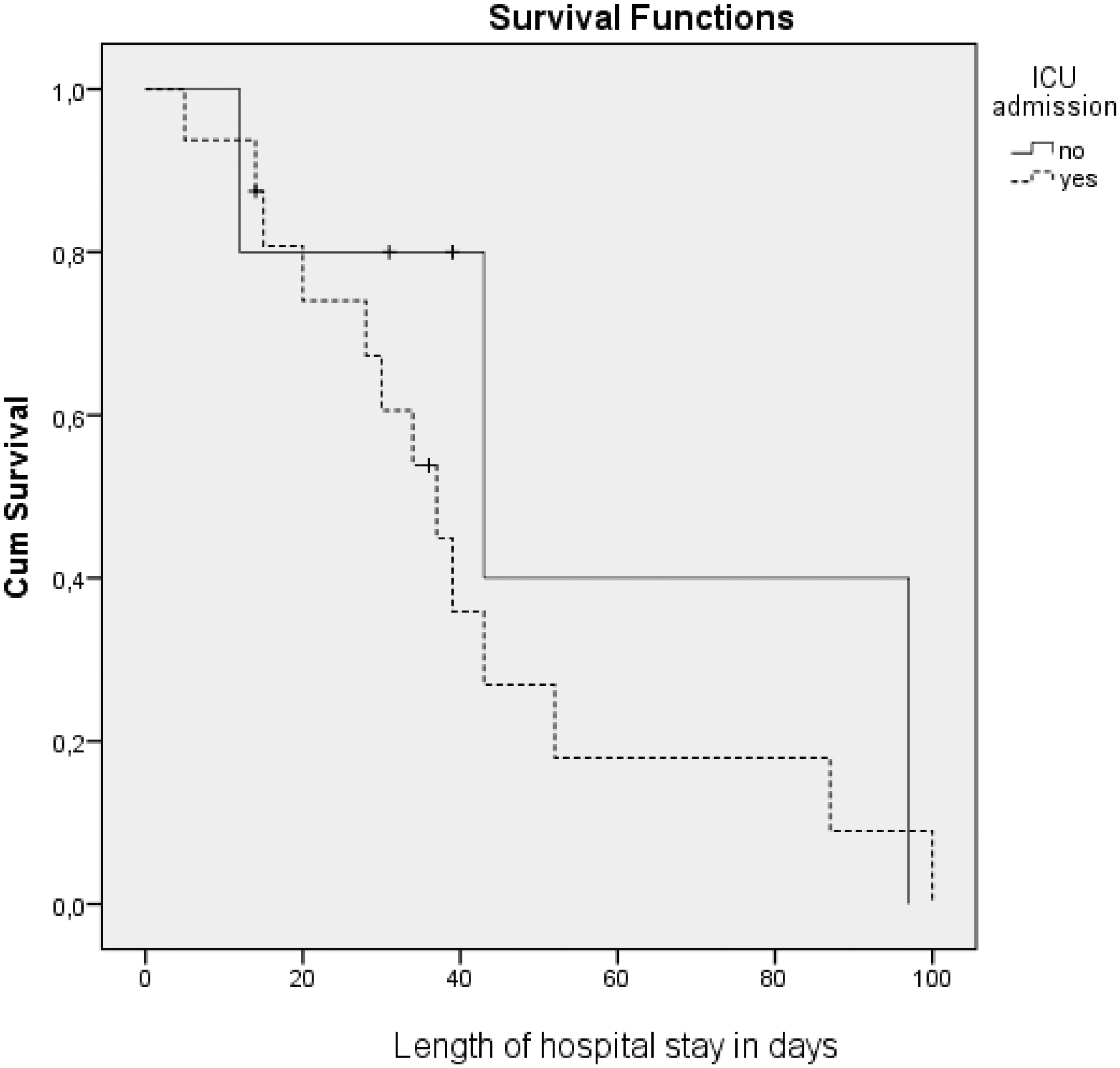
Patients identified for EoL care
The CCOS initiated or participated in EoL discussions in 37/126 patients (29%), and 43% of those (16/37) had a specialist palliative care team referral initiated also by the CCOS. Six patients (15%) had pre-recorded advance care planning discussions that could be easily identified by the team. Of the total length of time spent in reviewing patients with HM, 20% was devoted to EoL patients, a median of 5.5 days versus three days on non-palliative patients. The services provided by the CCOS were mainly facilitation of symptom control (67%) and/or support of ward teams in making decisions (78%). HFNCO was initiated in 6/37 (16%) EoL patients for symptom control; one of these patients was ultimately admitted in ICU for continuation of EoL care and HFNCO.
Discussion
The present study describes the experience of a medically-led CCOS in the assessment and management of patients with HM. Higher rates of ICU admission were reported when sepsis, hypoxia or hypotension was the reason for referral to CCOS. Receiving HFNCO was associated with a reduction in ICU admission, irrespective of the underlying diagnosis, performance status or location of delivery. The CCOS initiated or participated approximately 30% of the EoL discussions in this patient population.
In recent years, both the ICU and the hospital survival of patients with HM have improved significantly,19–21 as a result of combined technological and therapeutic advances in both medical fields. In the present study, the observed mortality was 25.3% and 45.2% for ICU and hospital respectively, which is comparable with the one noted in previous publications from the UK8,22 but also with what is described in the French literature.5,12 Conversely, it is markedly lower than that the reported in the related studies that assessed the impact of an outreach team in this patient cohort.16,17 These differences could be partly attributed to the variations in case-mix, the criteria for ICU referral and admission, as well as the treatment limitation decision-making in the disparate critical care climates, which pose limitations in the comparison of crude mortality rates. They could also be a result of an overall, temporal improvement in the outcomes of this patient population, as discussed above.
Even though ICU mortality was higher for patients who had undergone allogeneic HSCT, it was approximately half of that described in other, recent publications (33% vs. 64% 9 and 62% 23 ). Even though this is a high-risk population, their ICU and hospital mortality did not differ significantly from that of patients with autologous HSCT or those only receiving chemotherapy, a fact that could be due to the relatively small number of included patients. Approximately 25% of all allogeneic HSCT patients were referred to the CCOS, accounting for a significant part of their workload (40%) and highlighting the increased need for ICU input in this sub-population of HM.
The reported ICU admission rate was 47.6% which is significantly higher than the one described in some publications9,16,17 but lower than presented in others. 5 This discrepancy could be explained by the lower APACHE II score of the admitted patients in the present study (21.5 vs. 25.416 and 29.817), which probably reflects a more liberal admission policy in our institution. The number of referrals to the CCOS and having sepsis and respiratory failure as reason for these referrals were identified as independent prognostic factors not only for ICU admission, but also for ICU and hospital mortality. Even though disease-related predictors have been previously described,9,24,25 this is the first time that the intensity of the CCOS involvement is associated with higher subsequent need for ICU care, irrespective of the underlying diagnosis. This result can be attributed to an initial reluctance to admit the referred patients who has been previously described, 5 either because they were considered ‘too well’ to benefit from ICU or because of capacity restraints. However, and unlike reports in similar publications, 12 this potential delay did not result in increased ICU mortality, probably due to the overall lesser disease severity of the admitted patients and their regular review by a skilled critical care team.
One of the most valuable findings of the present study was the impact of HFNCO when delivered on the haematology wards under the supervision on the CCOS. Emerging research in the field of acute hypoxemic respiratory failure in immunocompromised patients has proved the feasibility of this relatively new non-invasive oxygenation modality.26–32 However, the results around its efficacy appear quite discrepant, mainly because of a lack of standardization in the included patients and their disease severity.27,28,33 The majority of these studies assessed the impact of the intervention when delivered in the ICU, whereas our results suggest that its administration is also safe on a ward level, provided it is supervised by skilled personnel, with clearly defined application and escalation criteria. The reported success rate of HFNCO, demonstrated by ICU admission avoidance, was 80% and no statistically significant difference was found in hospital mortality between the patients who received the intervention on the ward and those who went to the ICU. Unfortunately, our sample size was too small to adjust for any confounders, so this result needs to be interpreted with caution. The lack of a harm signal reported elsewhere 34 is probably attributable to the early initiation of the intervention, its delivery under the supervision of a critical care-trained team and the short duration of administration. 35 It is possible that the need for HFNCO highlighted deteriorating patients who benefited from early CCOS input. Furthermore, the short time spent on HFNCO (2 days) emphasizes the importance of the early recognition of non-response to treatment and the appropriate escalation to ICU admission.
A significant amount of CCOS time was devoted to the participation in EoL decision-making, in accordance with other research. 36 Despite the high risk of mortality and morbidity especially in the subgroup of patients undergoing HSCT, only 15% had clearly documented Advanced Care Planning discussions, a fact that has been previously highlighted. 37 The involvement of CCOS in EoL care provided an element of support to the ward staff, who welcomed their input in the final decision-making (78%) and utilized their critical care skills in the implementation of good quality EoL care. However, it raises the question of appropriateness in the engagement of a non-parent team (such as the outreach team) in difficult treatment limitation discussions, especially when they occur mainly out-of-hours and in acute situations. 38 Even though no conflicts or complaints were recorded, the present study demonstrates a lack of timely engagement in the Advanced Care Planning process, as the CCOS involvement occurred only when the patient became critically unwell.
The main limitations of this study are the relatively small number of patients included in some of the subgroups, as well as its retrospective nature. The former precludes the drawing of definitive conclusions and this may limit the positive results demonstrated in the HFNCO group. However, the concordance of our results with published data, point to their validity. Another limitation is the difficulty in extrapolating the reported results in other health care systems that endorse CCOS, as there is a lack of consensus around the models in use. The discrepancy that characterizes the composition of the outreach teams, their remits of intervention, their working timetable and the trigger systems used prohibit the generalizability of the results. Nonetheless, the described doctor-led model is common not only in the UK but also in Australia, 39 allowing for widespread, meaningful comparisons. Last, this retrospective, observational study precludes any inferred causality, especially as an outreach team constitutes a complex intervention, with potential confounding factors that have not been explored fully.
Conclusion
CCOS are heavily involved in the pre-ICU management of patients with HM both by intervening acutely on the wards and by facilitating EoL discussions. Survival of immunocompromised patients continues to show improvement, with allogeneic HSCT and referral to the CCOS for sepsis, hypotension or hypoxia being associated with a higher mortality. Initiation of HFNCO outside ICU appears to be feasible and safe, and no adverse consequences were found in this study. However, caution is warranted as the present model incorporates a skilled, consultant-led team, able to monitor and assess the success of the intervention, and effectively triage patients to identify those most likely to benefit from ICU admission. More research is needed in order to ascertain whether these results are applicable to other models of CCOS.
Supplemental Material
Supplemental material for The role of a critical care outreach service in the management of patients with haematological malignancy
Supplemental Material for The role of a critical care outreach service in the management of patients with haematological malignancy by Leila Taheri, Rathai Anandanadesan, Hugues de Lavallade, Eirini Pagkalidou, Antonio Pagliuca, Ghulam Mufti, Georg Auzinger and Victoria Metaxa in Journal of the Intensive Care Society
Footnotes
Acknowledgements
The authors would like to thank the Critical Care Outreach Team of King’s College Hospital for the assistance in data collection and their ongoing hard work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.