
Abstract
Background
Decision-making on end-of-life is an inevitable, yet highly complex, aspect of intensive care decision-making. End-of-life decisions can be challenging both in terms of clinical judgement and social interaction with families, and these two processes often become intertwined. This is especially apparent at times when clinicians are required to seek the views of surrogate decision makers (i.e., family members) when considering palliative care.
Methods
Using a vignette-based interview methodology, we explored how interactions with family members influence end-of-life decisions by intensive care unit clinicians (n = 24), and identified strategies for reaching consensus with families during this highly emotional phase of care.
Results
We found that the enactment of end-of-life decisions were reported as being affected by a form of loss aversion, whereby concerns over the consequences of not reaching a consensus with families weighed heavily in the minds of clinicians. Fear of conflict with families tended to arise from anticipated unrealistic family expectations of care, family normalization of patient incapacity, and belief systems that prohibit end-of-life decision-making.
Conclusions
To support decision makers in reaching consensus, various strategies for effective, coherent, and targeted communication (e.g., on patient deterioration and limits of clinical treatment) were suggested as ways to effectively consult with families on end-of-life decision-making.
Introduction
End-of-life (EOL) decisions relate to treatment strategies as death approaches or seems inevitable, 1 and in the intensive care unit (ICU), nearly 70% of deaths are associated with an explicit EOL plan. 2 Typically, clinicians and families reach decisions on a ‘best interests’ basis,3,4 and act as surrogate decision makers who make a ‘substituted decision’ for a patient based on assumptions about their needs and desires. EOL decisions are often framed by a legal context, for instance the UK’s Mental Capacity Act, 5 which mandates the seeking of views concerning values, goals, desires and cultural beliefs of an individual who lacks capacity. 6 Research on EOL in ICU has tended to focus on how next-of-kin and clinician factors influence decision-making.
First, studies show that despite families having an important role as surrogate decision makers or advisors, their involvement varies, 7 with discussions of patient preferences for end-of-life decisions sometimes being absent.8,9 The role of families can appear unclear and without guidance,8,10 resulting in poor communication and potentially poor patient and family outcomes. 11 Furthermore, and reflecting the genuine challenges of surrogate decision-making, 12 next-of-kin surrogates (68%) often misjudge the preferences of their loved ones 13 and are more likely to accept a life-saving treatment for a loved one than they would themselves. 14
Second, clinician expectations for survival are often used to explain EOL decisions.15,16 Physicians with greater critical care experience are less likely to recommend very invasive care for patients seemingly at the end of their lives. 17 Yet, the implementation of a decision, for example on adopting a palliative approach, is often determined by non-clinical factors: for instance institutional norms (e.g., on the goal of treatments, determination of ‘dying’), 18 clinical team interactions19,20 and family values and behaviours, in particular religion and its perceived involvement in a patient’s life. 21 This indicates that EOL decision-making can be a product of both clinical factors and wider social factors (e.g., ethics, norms, family wishes).
Improving EOL decision-making remains a priority, 22 and understanding of the intertwined role of clinicians and families is essential for achieving this. Of particular concern are cases where clinical staff believe an EOL decision is necessary, however next-of-kin do not, as this scenario can be highly upsetting for both families and staff, and costly in terms of time, resources and potentially litigation. Through qualitatively investigating how clinicians respond to an EOL scenario, the objective of the current study is to understand how interactions with families shape EOL decision-making, and identify the strategies used by clinicians to ensure effective consensus building on EOL.
Method
The study received institutional approval from local university and hospital research compliance offices. All participants provided written informed consent.
Design
End-of-life decision-making vignette scenario.
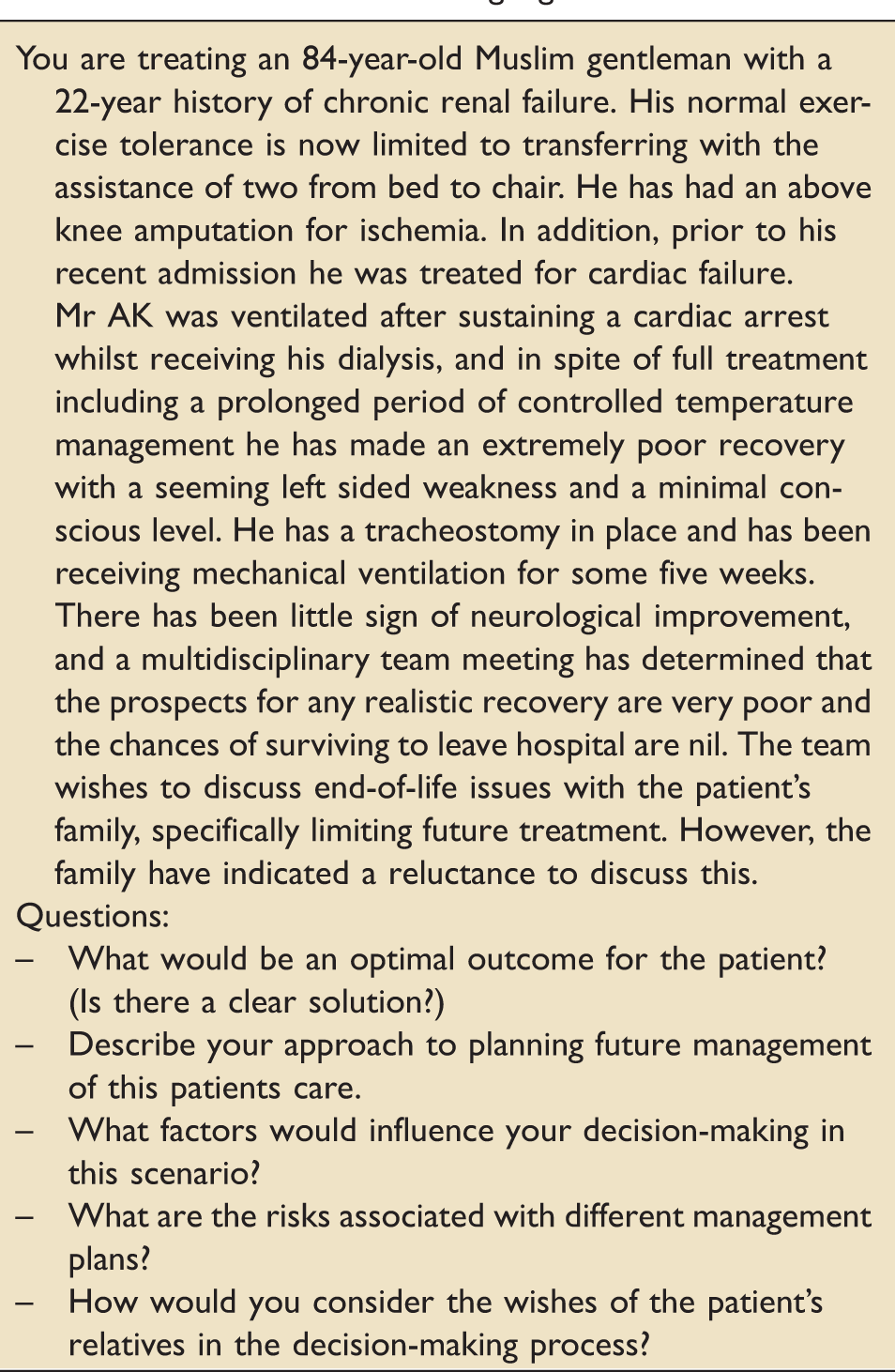
On reading the scenario, the participants discussed, through a semi-structured interview (15–20 min), their thoughts on how to handle the clinical scenario. The interview was recorded and questions (see box 1) were used as initial prompts after which a wider discussion was encouraged. The interviews were undertaken by a psychologist with no pre-existing relationship with the participants, and independent from the institutions in which research was being conducted.
Analysis
The data were collected, transcribed and coded. First, and drawing on the decision-making literature, 26 an overview of how the clinicians interpreted and responded to the scenario was made. Each transcript was analysed in terms of the decision-making for Mr AK, focusing on the key factors reported by clinicians as influencing decisions on EOL. Then, using thematic analysis, 27 we focussed on statements related to strategies for building a consensus with families, understanding their perspective and ensuring effective communication. Statements were grouped together in order to form themes. The purpose was to identify recurring issues, relating to each topic, on the factors that facilitated, or inhibited, decision-making with families. To illustrate these themes, quotes were extracted from a sample of diverse interviews. An MSc-level psychologist undertook initial coding and this was then elaborated and sense-checked by a senior psychologist and intensive care clinician.
Participants
Participants (n = 24) comprised of eight junior trainee doctors (JT; core trainees), eight senior trainee doctors (ST; registrars) and eight senior doctors (SD: consultants or attending physicians) practicing in three university hospitals in London. All participants had experienced and been part of teams that had been involved in EOL episodes.
Results
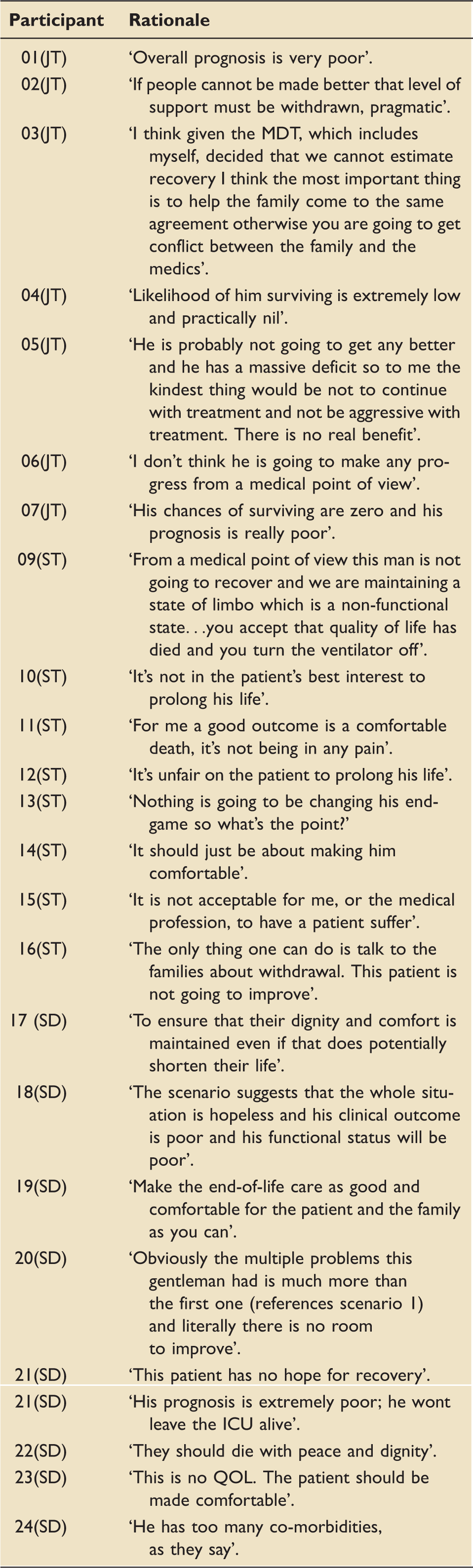
Clinician decision-making: Overview
Participant rationales for end-of-life decision.
Consensus building with families on EOL
Participants discussed five strategies that, based on their experiences, they judged essential for building consensus with families on EOL.
Building trust and understanding
Building trust and understanding with Mr AK’s family was recognized as paramount. Clinicians argued: ‘The key issue here is understanding why the family is reluctant to discuss this (end-of-life care)’. The law was widely considered a factor in building a relationship and brought into mind legal considerations. To clinicians, the law was ambiguous in terms of who had ultimate decision-making power in Mr AK’s scenario, and building a relationship with the family was key to avoiding any conflict. One of the clinicians said ‘we cannot estimate recovery. I think the most important thing is to help the family come to the same agreement otherwise you are going to get conflict between the family and the medics’.
Strategies for building trust with Mr AK’s family varied according to respondent. One ST stated: ‘It’s not something I would speak to the family about unless I had put some groundwork in and made sure I had their trust’. To build trust, clinicians discussed ensuring that where possible the same consultant communicates with a family. One clinician explained ‘Having the same consultant for a number of weeks helps so maybe that consultant has been with the family for a while so that does maintain some level of continuity’. Overcoming denial was key. One clinician explained the reluctance to discuss withdrawal of care as sometimes ‘a kind of a denial thing … they (families) don’t want to think about their relative dying so it’s a part of their grieving process to deny it’. Such observations confirm research showing that rushing families to make the decision to withdraw life sustaining treatment before they are ready can erode the trust that families have in clinicians, 28 and that effective communication skills are essential for building trust. 29
Breaking perceptions of normalization
Clinicians discussed how, over time, families get used to seeing the patient in critical states and view it as ‘normal’, and that breaking perceptions of this for Mr AK’s family were important. For patients with a severe chronic disease, their functional decline is incremental to a point of significant incapacity; this can shape discussions on the withdrawal of care during an acute illness. For example, one participant said ‘it’s about people adjusting their normal values … and (the family may think) he is doing okay even if they are just on a breathing machine and not doing anything else’. Others felt that one must be patient while communicating and allow families to take their time. (e.g. ‘doesn’t happen overnight’). One clinician talked about slowly preparing families for the outcome ‘I think it has to be a very slow process … you have to try and gradually drip feed a bit more information and repeat things over and over’. This reflects research showing that helping families to recognize a patient’s deterioration is an integral part of the process when shifting to palliative care. 30
Ensuring realistic expectations of ICU care
Clinicians discussed the importance of explaining the limitations of ICU care to Mr AK’s family, with next-of-kin often unaware of the average statistics on likelihood of recovery in ICUs and focusing on exceptional cases (base-rate neglect). For example, a SD said ‘I think because of the media, expectations of intensive care are quite high. Just the expectations of things like CPR … one has to understand how little they (next-of-kin) actually know’. Clinicians felt that the best way to communicate was by providing an ‘evidence-based’ approach: for instance by explaining to families the percentage of patients who have been in similar situations and have not survived.
More specifically, clinicians also discussed that, often, families are unaware of the consequences of life-saving treatment, and that this was important to raise with Mr AK’s family. Due to lack of medical knowledge, they argued families are sometimes shocked to see how inhumane some of the procedures are and immediately regret their decision. One participant said: ‘They (families) actually don’t really understand the implications of a certain test or like CPR’. Determining family knowledge on life-saving treatments was essential, as was communicating the implications of this treatment option against palliative care. For instance, by emphasizing of a comfortable death: ‘it’s not being in any pain, it’s not vomiting, it’s not being constipated, it’s not being agitated, it’s not climbing up the walls in delirium’.
Avoiding guilt
Clinicians discussed the need to anticipate family resistance to withdrawing care due to feelings of guilt. A clinician explained ‘some people- they almost don’t want to feel that they have given up on their relative’. Clinicians discussed addressing this for Mr AK through making it explicit to families that the clinicians are ultimately responsible for patient outcomes. One said: ‘You don’t ask the family’s permission to withdraw life support because they feel like they are responsible for decision … you frame it in a way that you are taking responsibility for it’. Another said: ‘it needs to be communicated them that it is the medical team’s decision … I think people find it less troubling and feel less guilty about it’. These observations reflect research describing the high levels of emotional discomfort, guilt and sense of responsibility felt by surrogates who feel accountable for a patient’s death. 31
Spirituality and religion
For this scenario, faith was considered an important issue. Clinicians were mindful that some Muslim families may feel for religious reasons, unable to support withdrawal of life-sustaining care; this attitude is not unique to Islam, and held by various religious groups. In such cases, clinicians would perhaps choose to explain ‘death as predetermined and that nature will take its course’ while encouraging a shift to palliative care. Presumably, the extent to which religion would be a factor in decision-making would depend on the family’s own interpretation and expressed commitment to spiritual guidelines. Also, factors considered unacceptable to some communities (e.g. lack of prospects for recovery of consciousness), may be considered more acceptable in other communities. Another strategy for managing the interaction between faith and EOL decisions was to enlist chaplains or members of palliative team for support. For example, one clinician said ‘In times of disagreement, maybe a religious person in the hospital like a chaplain or other teams who are more accustomed to that so the palliative care team who can maybe explain it differently’.
Discussion
In this study we aimed to understand how interactions with families shape EOL decision-making and to identify the strategies used by clinicians to ensure effective consensus building on EOL. Although we found various factors to shape decision-making on EOL (e.g. experience), negotiating consensus (or at worst acquiescence) becomes a goal for clinicians once a patient is identified as requiring a palliative approach. Concerns over the consequences (e.g. legal) of not reaching a consensus weighed heavily in decision-making, and, according to clinicians, this often arose from unrealistic family expectations of care, the normalization of patient incapacity and belief systems that influence end-of-life decision-making.
In the UK, where this study was undertaken, the Mental Capacity Act 5 obliges those caring for a patient who lacks capacity to seek the views of those close to the patient who can represent their perspective: however, decisions ultimately rest with the institution and professionals. Yet, the Mental Capacity Act Code of Practice (sections 8.18 and 8.24) 32 obliges a referral to the Court of Protection in cases where there is dispute concerning best interests. Against this context, it is notable that participants in the current study discussed the importance of managing families, rather than seeking views as to what the patient would wish. It is possible that the framing and presentation of the vignette, with a religious element and a family reluctant to engage, pushed people immediately into a negotiating rather than a view-seeking mode. Alternatively, and in a type of ‘loss aversion’ (where people focussing on avoiding ‘losses’ – viz. adverse consequences), 33 participants may not have perceived there was a decision to be made, and thus focussed on avoiding moral distress, time-consuming complaints and legal disputes.
In terms of the extant literature, the observations from ICU clinicians were consistent with research showing that surrogate decision-makers can misjudge the preferences of their loved ones, 13 and that unrealistic patient and family expectations were seen as a potential barrier to high-quality palliative care. 29 To address this, effective, coherent and targeted communication is required, with sensitivity to the traditions and emotional states of families being essential to building consensus. Furthermore, rather than focussing on more subjective issues such as quality-of-life (which involve value judgements), clinicians may better focus on the impact of continuing or avoiding unnecessary and unpleasant procedures for patients. This resonates with research showing the importance of language used to frame treatment alternatives to EOL care 34 and the importance of discussing specific interventions in terms of their risks and benefits. 35 It also reinforces the importance of considering faith where this is important to patients and families. 36 Constraints around resourcing were generally not considered in relation to EOL decision-making, yet may be important influences upon decision-making in more resource-constrained contexts.
Strategies for consensus building in end-of-life (EOL) decision-making.
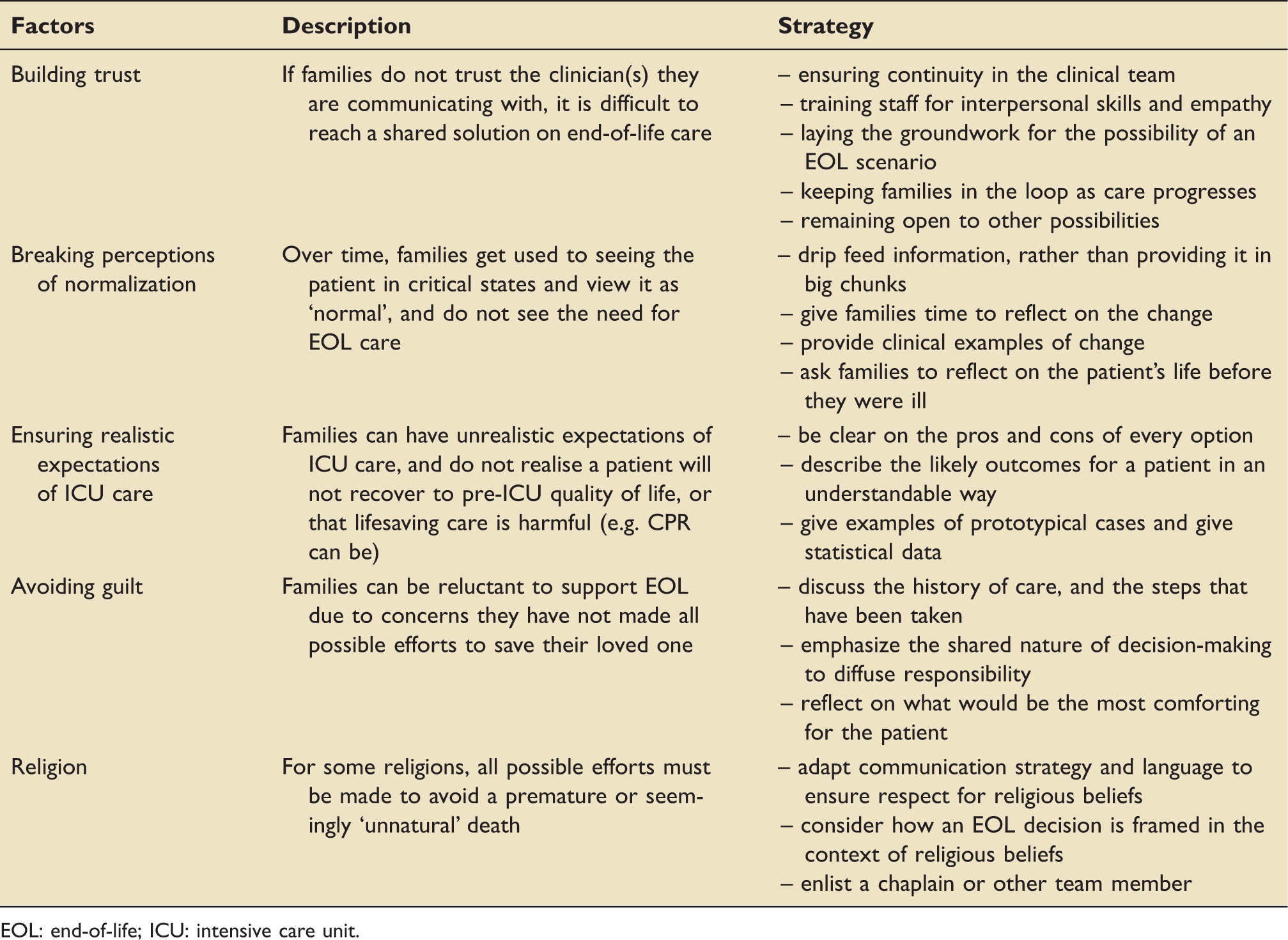
EOL: end-of-life; ICU: intensive care unit.
The study has a number of limitations: it was performed in one institution and three ICUs across North West London. Although participants were diverse and data saturation was achieved (e.g. in discussing how to work with families), participants in other hospitals (or countries) may have responded differently. The study relies on participants projecting their decision-making behaviour (which may not be accurate), and the generalizability of findings is unclear.
Finally, the study was undertaken before the global COVID-19 crisis, and arguably reflects ‘peacetime’ operations in ICU, where family members are able to visit loved ones. However, the concerns identified here, particularly around trust, remain relevant. Our previous research has shown the challenges of resource scarcity for decision-making in ICU, 26 with decisions on ICU admissions often being ethical decisions as much as they are clinical decisions. Where COVID-19 cases remain high, refusal to admit patients to ICU may become a form an EOL decision, and engagement with families is essential for maintaining trust, and ensuring that ICU staff feel that they have provided the best care in very challenging circumstances.
Conclusion
End-of-life decisions are amongst the most challenging for ICU doctors to make: they involve application of expertise, consideration of resources and ethics and interactions with families who may feel they should contribute to the decision. This study found, through a series of vignette interviews, that the undertaking of EOL decisions was often affected by a form of loss aversion whereby concerns over the consequences of not reaching a consensus with families weighed heavily in the minds of clinicians. Conflict was perceived to arise from unrealistic family expectations of care, family normalization of patient incapacity and belief systems that prohibit end-of-life decision-making. Effective, coherent and targeted communication (e.g. patient deterioration and limits of clinical treatment) were suggested as ways to avoid conflict and reach consensus on decision-making.
Supplemental Material
sj-pdf-1-inc-10.1177_1751143720954723 - Supplemental material for At the end: A vignette-based investigation of strategies for managing end-of-life decisions in the intensive care unit
Supplemental material, sj-pdf-1-inc-10.1177_1751143720954723 for At the end: A vignette-based investigation of strategies for managing end-of-life decisions in the intensive care unit by Tom W Reader, Ria Dayal and Stephen J Brett in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by a small grant from the London School of Economics. Infrastructure support was provided by the NIHR Imperial Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NIHR, the NHS or the UK Department of Health and Social Care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.