
Abstract
Decision-making by intensivists around accepting patients to intensive care units is a complex area, with often high-stakes, difficult, emotive decisions being made with limited patient information, high uncertainty about outcomes and extreme pressure to make these decisions quickly. This is exacerbated by a lack of clear guidelines to help guide this difficult decision-making process, with the onus largely relying on clinical experience and judgement. In addition to uncertainty compounding decision-making at the individual clinical level, it is further complicated at the multi-speciality level for the senior doctors and surgeons referring to intensive care units. This is a systematic review of the existing literature about this decision-making process and the factors that help guide these decisions on both sides of the intensive care unit admission dilemma. We found many studies exist assessing the patient factors correlated with intensive care unit admission decisions. Analysing these together suggests that factors consistently found to be correlated with a decision to admit or refuse a patient from intensive care unit are bed availability, severity of illness, initial ward or team referred from, patient choice, do not resuscitate status, age and functional baseline. Less research has been done on the decision-making process itself and the factors that are important to the accepting intensivists; however, similar themes are seen. Even less research exists on referral decision and demonstrates that in addition to the factors correlated with intensive care unit admission decisions, other wider variables are considered by the referring non-intensivists. No studies are available that investigate the decision-making process in referring non-intensivists or the mismatch of processes and pressure between the two sides of the intensive care unit referral dilemma.
Background
Intensive care units (ICUs) are specially staffed and equipped, separate and self-contained areas of a hospital dedicated to the management of patients with life-threatening conditions. They provide dedicated facilities for the support and monitoring of vital physiological functions and use the specialist knowledge and skills of medical, nursing and other personnel experienced in the management of these problems. These units are widely recognised to reduce mortality rates in critical illness and do so in a cost-effective manner.1,2 However, the number of beds is a limited resource, with far more referrals made than available bed numbers. This problem is only expected to worsen over the coming years with the rise in demand for intensive care bed days estimated to likely be in the order of 4% per annum. 3 It is also acknowledged that not all patients benefit from admission to the ICU, with evidence that certain patient factors (e.g., comorbidities, such as chronic obstructive pulmonary disease and end-stage liver cirrhosis, and conditions such as multi-organ failure) are associated with better or worse outcomes from referral to ICUs than others. 3
With this mismatch of supply and demand, it is the job of senior intensivists to decide how to allocate this resource. These are often high-stakes, difficult, emotive decisions being made with limited patient information, high uncertainty about outcomes and extreme pressure to make these decisions quickly. This is exacerbated by a lack of clear guidelines to help guide this difficult decision-making process, with the onus largely relying on clinical experience and judgement. A recent report by a task force of the world federation of societies of intensivists that explored issues of triage and guidelines stated that ‘Although algorithms can be useful they can never supplant the role of skilled intensivists’. 4 However, a lack of guidelines, when working in ambiguous, pressurised and risky contexts, can derail decision-making due to the tendency to rely on psychological biases and faulty heuristics that override more rational processing. For example, using ‘representative heuristics’ to label a patient as ‘unlikely to do well’ on ICU based on prototypical knowledge about that patient type, instead of more rational consideration of the specific qualities of that patient, an issue that is often exacerbated by time pressure to make these decisions quickly.
This uncertainty, compounding decision-making at the individual clinical level, is further complicated at the multi-speciality level for the senior doctors and surgeons referring to ICUs. The lack of consensus around what constitutes an intensive care patient at the unit level can risk further ambiguity for those referring to the unit. Furthermore, these decisions mirror the challenges of those faced by intensivists, also being; difficult, high-stakes, emotive decisions made with lack of time and often without a full understanding of what intensive care can offer these patients. This decision also lacks any clear guidelines or algorithms to help guide it.
This is a systematic review of the existing literature about this decision-making process and the factors that help guide these decisions on both sides of the ICU admission dilemma.
Method
PubMed literature search
Terms: ‘intensive care unit’, ‘referral’, ‘admission’, ‘accepting’, ‘refusal’. Forty-one papers were identified and a further three identified from manual searching of references. Abstract assessment for relevance led to 17 papers being discarded as not relevant due to being either not primary research or due to studying intensive care factors not to do with admission or referral factors. Further content analysis of the remaining 26 papers led to them being allocated into four categories:
Objective factors correlated with admission decisions by intensivists Factors identified in clinical scenario-based studies investigated intensive care decision-making Qualitative investigation of decision-making in ICU admission decisions by intensivists Factors identified in referring to ICU decision-making by non-intensivists
Papers were analysed and results presented within these categories, with some papers fulfilling criteria to be analysed under multiple categories (see Figure 1).
Systematic literature search methodology.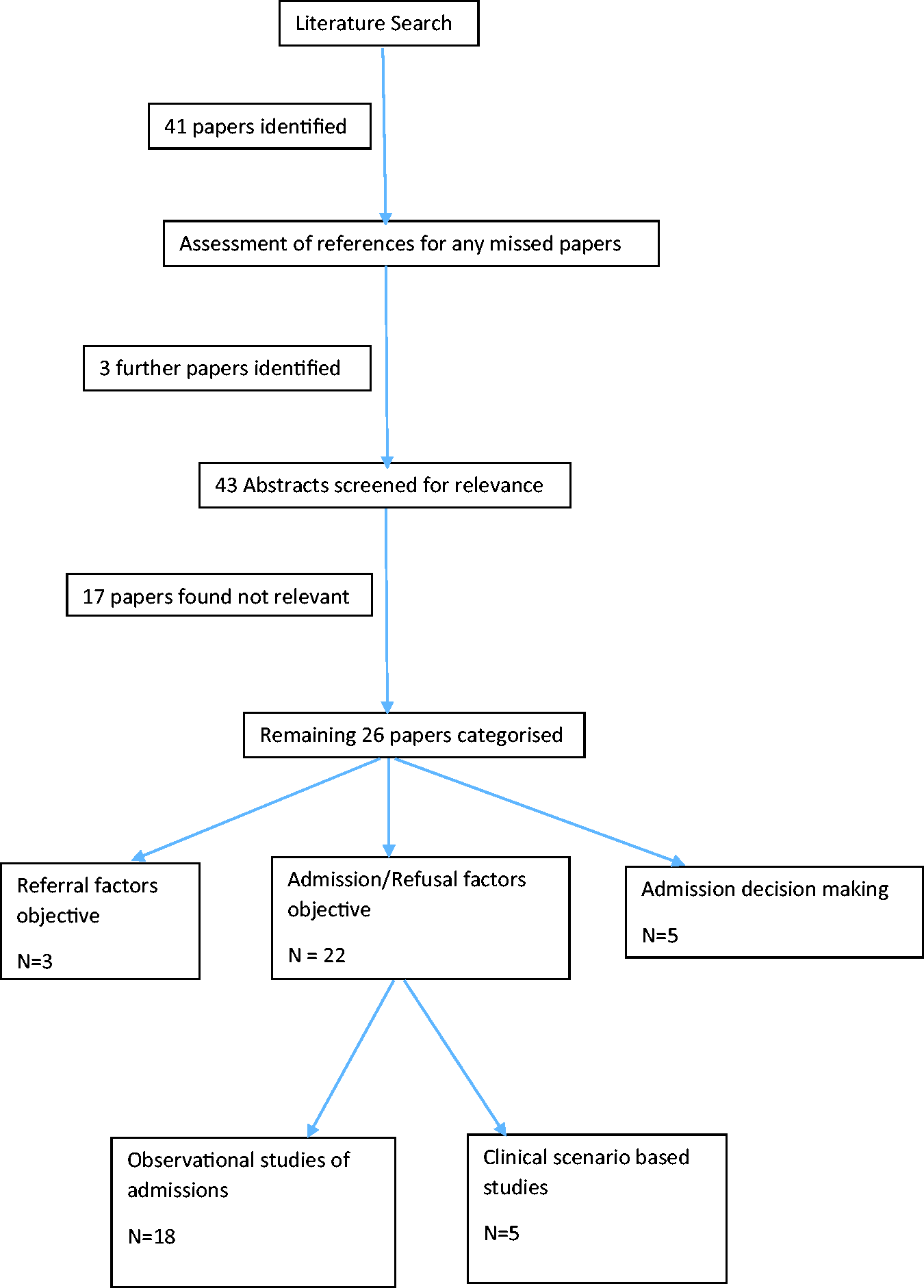
Results
Objective factors correlated with admission decisions by intensivists
Observational prospective studies analysing factors associated with ICU admission or rejection.
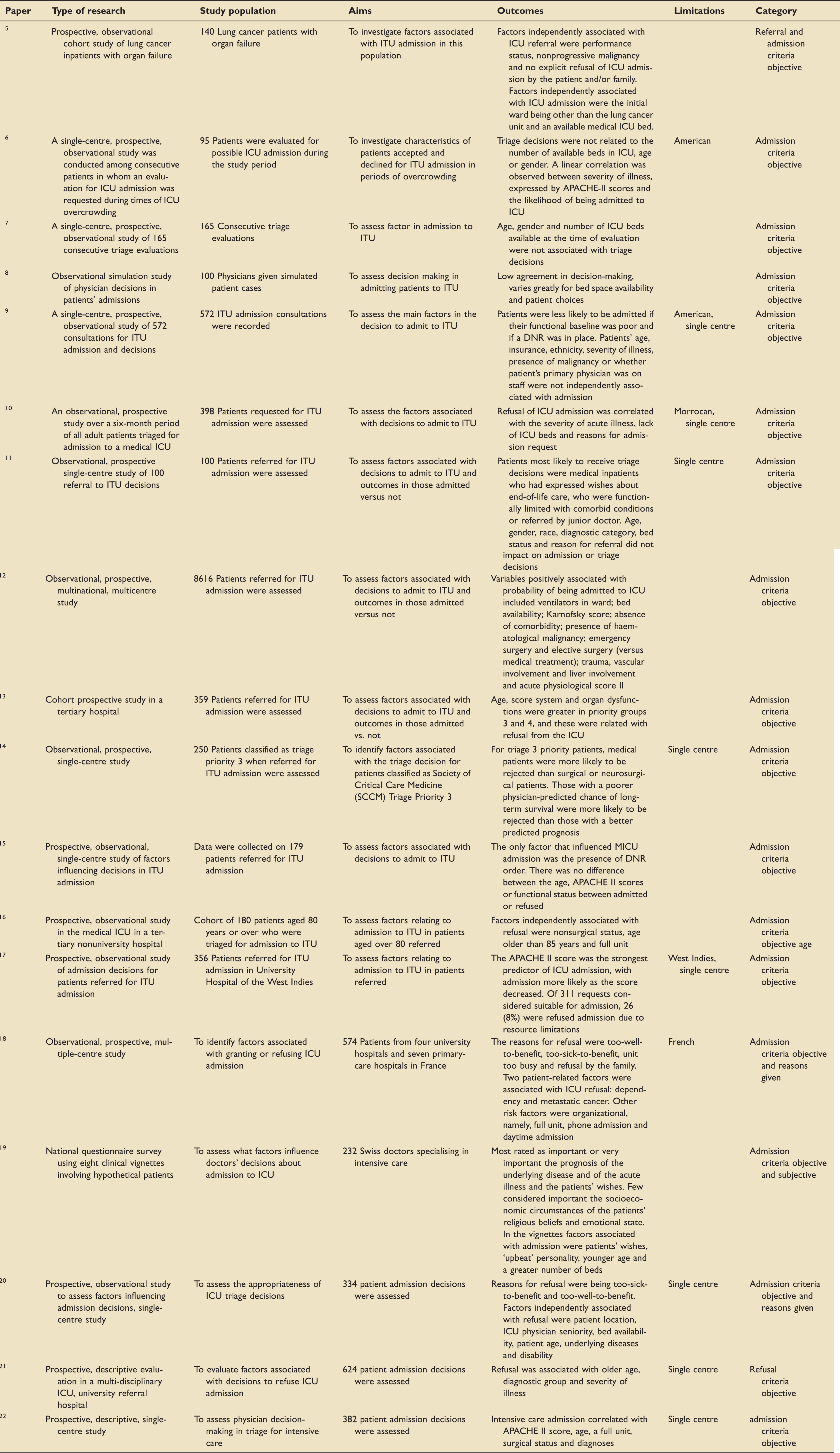
DNR: do not resuscitate; ICU: intensive care unit; MICU: medical intensive care unit; ITU: intensive therapy unit.
Factors associated with ICU admission or rejection.
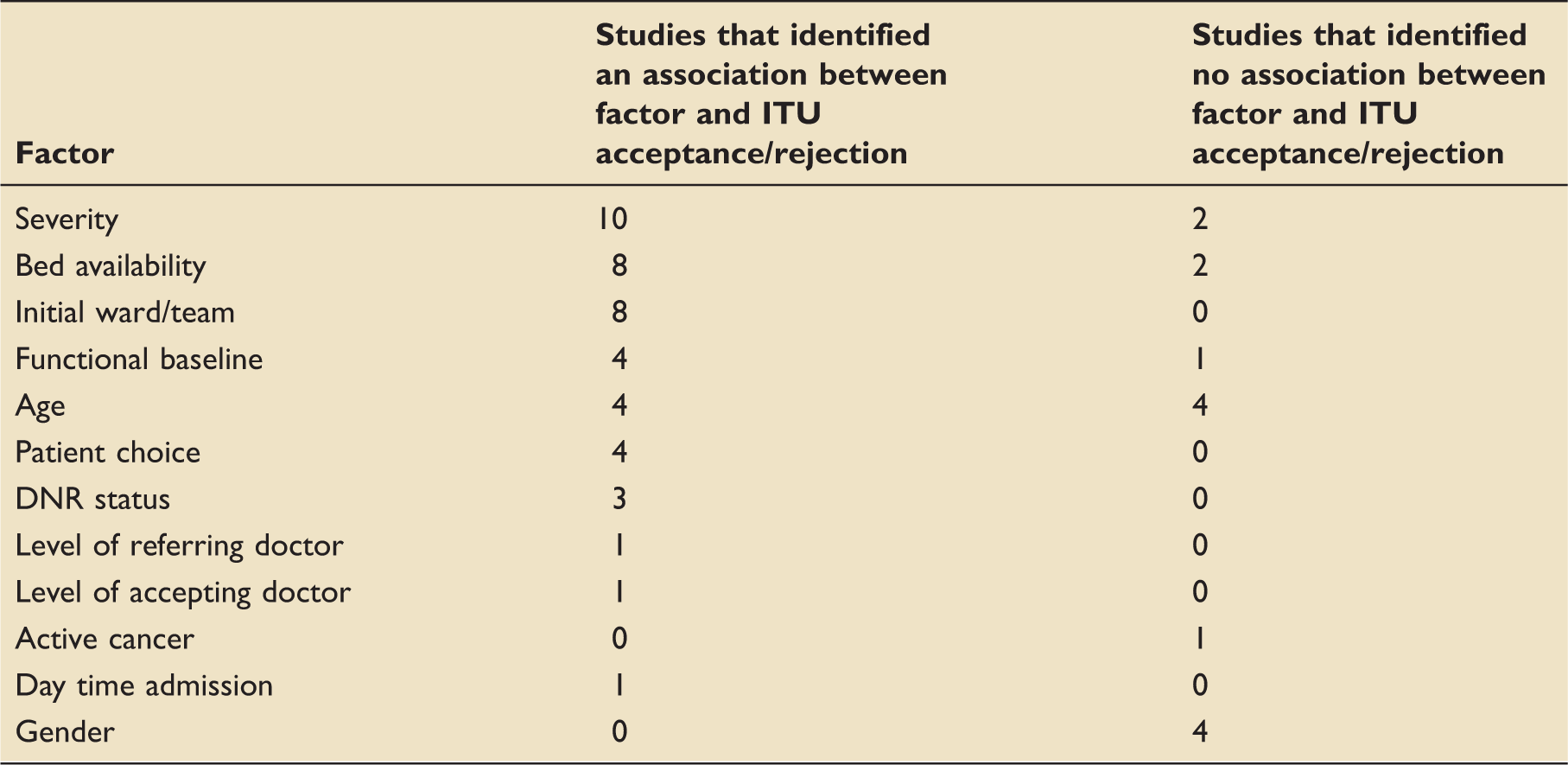
DNR: do not resuscitate; ITU: intensive therapy unit.
Factors identified in clinical scenario-based studies investigated intensive care decision-making
Clinical vignette based studies of ICU decision making.
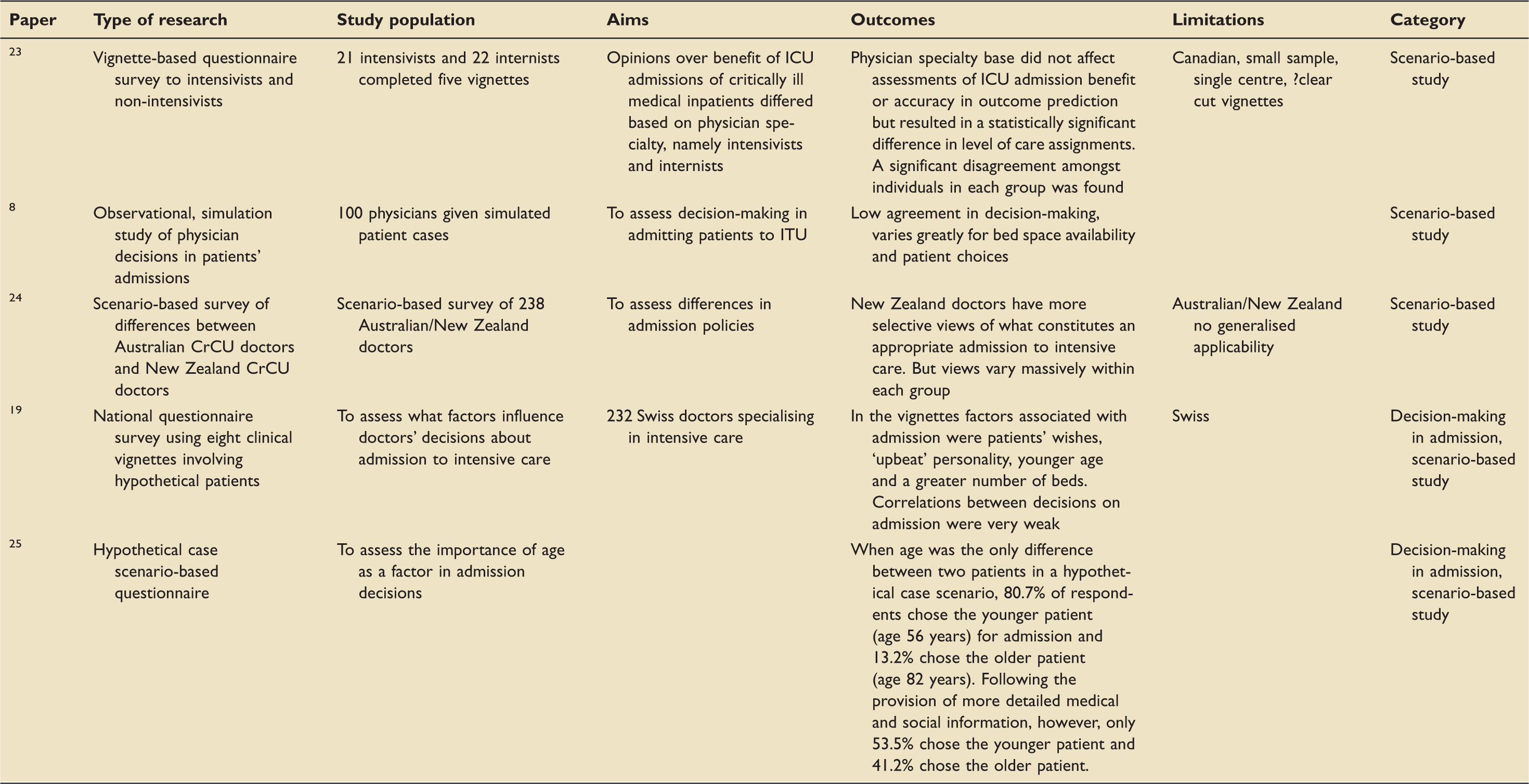
CrCU: critical care unit; DNR: do not resuscitate; ITU: intensive therapy unit.
Two of these used general scenarios to a population of intensivists to identify important factors. These studies identified similar factors to the above category of studies, including age, bed space and patient choice. Interestingly, the most important finding in each of these studies was the low agreement in decision-making amongst the intensivists, with very weak correlations between decisions to admit.
One of the studies used scenarios to assess the difference in admitting decisions between Australian and New Zealand intensivists. Although it did find that New Zealand intensivists had more selective views of what constitutes an appropriate admission to intensive care, it also found that views vary massively within each group.
One study used a scenario-based design to assess decision-making around patient age and ICU admission decisions. When the vignette differed only by age of the patient, the vast majority picked to admit the younger patient; however, following the provision of more detailed medical and social information skewed in the favour of the older patient, this levelled out to half the participants picking the younger patient. This study again showed big differences in the decisions made between intensivists within the group of intensivists making decisions.
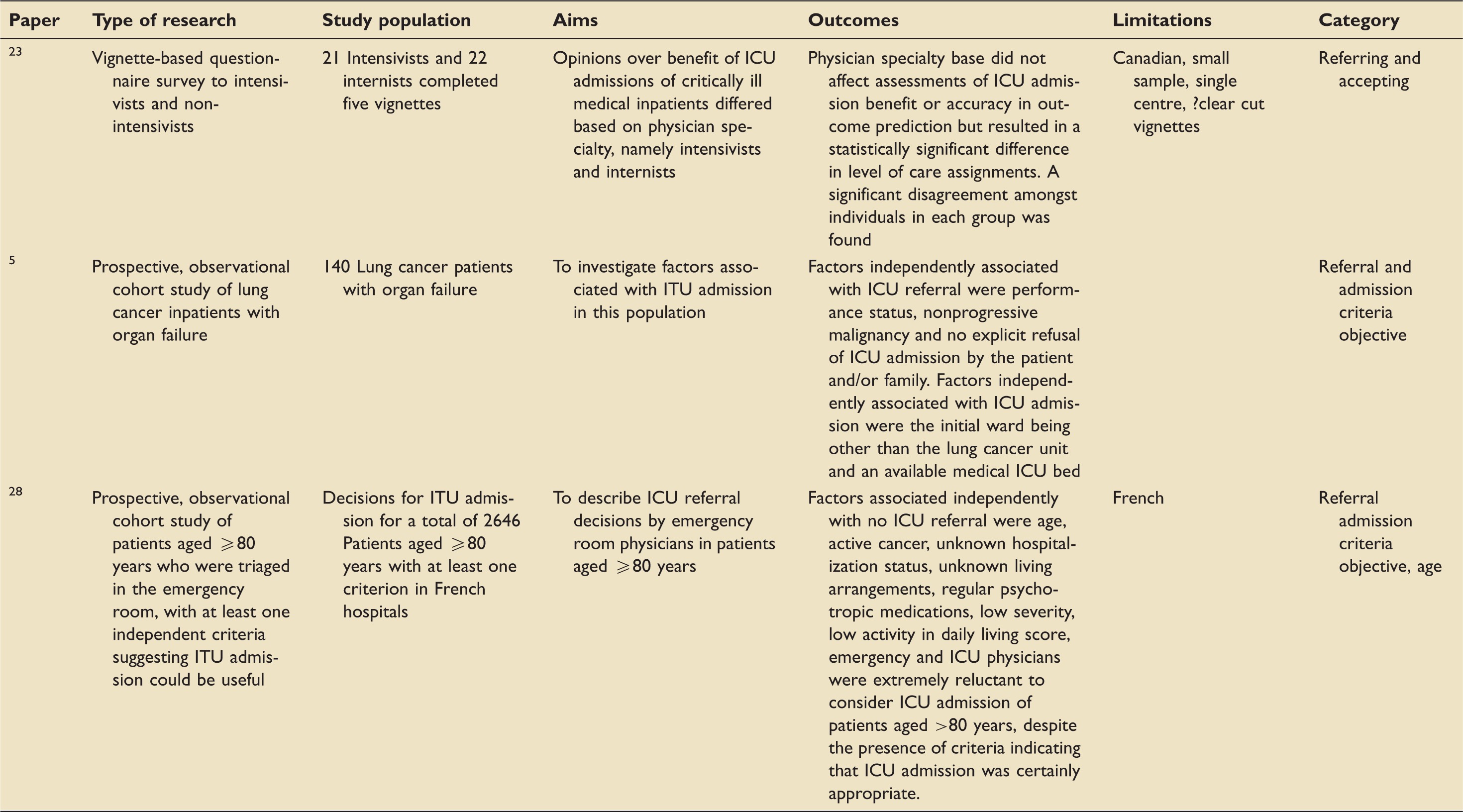
The final scenario-based study aimed to investigate the differences in opinion over the benefit of ICU admission from intensivists and non-intensivists. They found that there was no difference in assessments of ICU admission benefit between intensivists and non-intensivists; however, a statistically significant difference in levels of care assignments, such as treatment limitations and DNCPR decisions, was found between them. Again the most striking finding was the significant disagreement amongst individuals in each group regarding admission decisions.
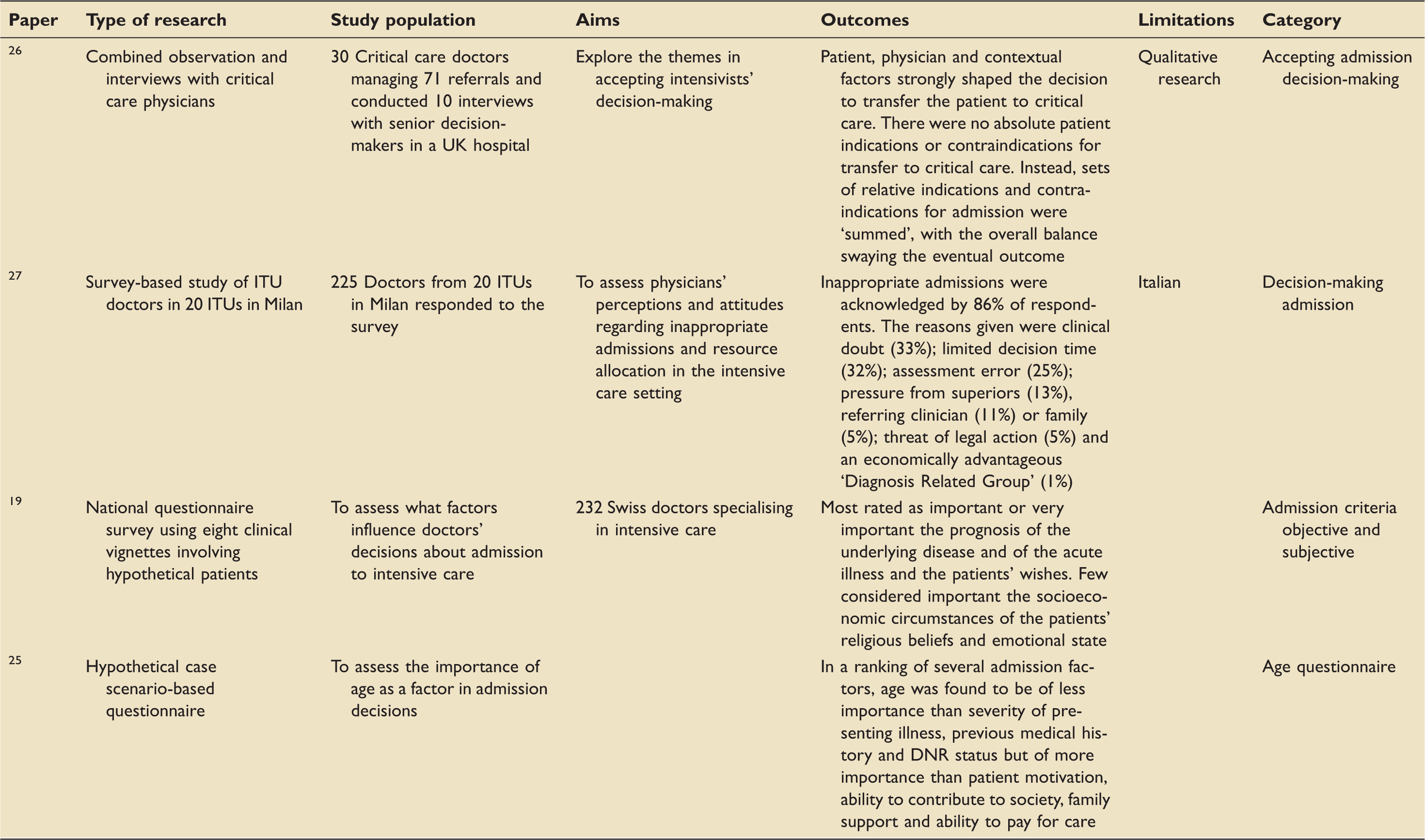
Qualitative investigation of decision-making in ICU admission decisions by intensivists
Survey or interview based studies of ICU decision making.
DNR: do not resuscitate; ITU: intensive therapy unit.
The use of ranking importance of factors highlighted the importance of many of the factors identified by objective correlation of factors in decision-making or real cases such as severity of illness, patient wishes, DNR status, age and bed availability. A new factor was also identified as playing a role in admission decision-making which was not shown in the objective factor correlation studies – patient’s personality, with an ‘upbeat’ patient personality favouring a decision to admit to ICU.
One study using a survey to investigate intensivists’ perceptions and attitudes regarding inappropriate admissions and resource allocation found that the vast majority admitted to having made inappropriate admission decisions. The reasons behind these included clinical doubt, limited decision time, assessment error, pressure from superiors or referring clinician or family, threat of legal action and in economically advantageous patient groups.
One study used an ethnographic approach of combined observation and interviews to qualitatively investigate the decision-making process and concluded that patient, physician and contextual factors strongly shaped the decision to transfer the patient to intensive care. There were no absolute patient indications or contraindications for transfer to intensive care. Instead, sets of relative indications and contraindications for admission were ‘summed’, with the overall balance swaying the eventual outcome. It also identified a very experientially led decision-making process.
Factors identified in referring to ICU decision-making by non-intensivists
Studies investigating decision making by referring non intensivists.
DNR: do not resuscitate; ICU: intensive care unit; ITU: intensive therapy unit.
One of these studies looked at factors associated with ICU referral. Some of these factors match those identified in factors associated with ICU admission, such as age, severity of illness and functional baseline. Some factors were seen to influence referral decision-making which have not been identified in the studies investigating accepting decision-making, such as active cancer status, unknown living arrangements and regular psychotropic medication use, all of which were correlated with a decision not to refer the patient to ICU.
One, which has already discussed in the scenario-based study section, showed that there was no difference in assessments of ICU admission benefit or accuracy in outcome prediction between intensivists and non-intensivists, but there was a statistically significant difference in level of care assignments. A significant disagreement amongst individuals in each group was found.
One study investigated the difference in factors correlated with both ICU referral and admission in a specific subpopulation of patients – those with lung cancer. They found that factors associated with ICU acceptance were similar to those outlined in the above for the general patient population of: bed space and initial ward they were referred from. Interestingly, here the most important factor for admission acceptance was being from a ward other than the lung cancer ward. Factors correlated with ICU referral were performance status, nonprogressive malignancy and no explicit refusal of ICU admission by the patient and/or family.
Discussion
This review had analysed many different study designs and approaches investigating decision-making in ICU referral and admission decisions. A wealth of information in the form of many, large, well-designed, prospective, observational studies exists assessing the patient factors that correlated with ICU admission decisions. Analysing these together suggests that the factors consistently found to be correlated with a decision to admit or refuse a patient from ICU are bed availability, severity of illness, initial ward or team referred from, patient choice, DNR status and functional baseline. These factors identified by this study type were also identified using clinical scenario-based studies to investigate factors associated with ICU admission decisions.
Some factors are not surprising including DNR status, patient choice and functional baseline, whilst others may be due to the varying health economics of the studies (for example, limited bed capacity or the severity of illness of patients accepted to a unit).
Age as a factor has been found to be associated with ICU admission decision and not associated with ICU admission decision in equal numbers of studies. Several survey studies done with intensivists themselves have shown that the majority of intensivists think that age is an important factor. Even amongst the dearth of information that exists on decision-making in referring non-intensivists, it has been shown that age is a factor that correlates with the decision to refer to ICU. Further investigation of this complex variable by way of clinical scenarios adjusted by age shows that age is an important variable when all other patient factors are matched, but when further patient information is available in favour of the older patient, it become less important. We suspect that this is because age may be clinically used as a surrogate for comorbidity and frailty.
Much less research has been done on the decision-making process itself and the factors that are important to the accepting intensivists when they make these decisions. The few small studies that exist show that in general the factors which objectively correlate to admission decisions are subjectively considered by intensivists too, with other factors such as patient personality, which may be harder to capture in an observation objective study design. The only study that exists looking qualitatively at the decision-making process by an interview-based study design gives an overview on how these patient factors added to physician and contextual factors to shape the decision to transfer the patient to ICU, with sets of relative indications and contraindications being ‘summed’, with the overall balance swaying the eventual outcome. 26 It has also been shown that intensivists are under a lot of pressure during these decisions and that the vast majority are aware of making the wrong decision at times due to external stressors influencing their decision-making such as clinical doubt, limited decision time, assessment error, pressure from superiors or referring clinician or family or threat of legal action. 27
Even less research exists on referral decision, with only a small study investigating factors that are correlated with ICU referral and demonstrating that as well as the factors correlated with ICU admission decisions, other wider variables are considered by the referring non-intensivists such as active cancer status, unknown living arrangements and regular psychotropic medication use, perhaps suggesting a more holistic patient assessment. 28 No studies are available that investigate decision-making process in referring non-intensivists or the mismatch of processes and pressure between the two sides of the ICU referral dilemma.
Conclusion
Many prospective observational studies and clinical scenario-based studies exist assessing the patient factors correlated with ICU admission decisions. Analysing these together suggests that the factors consistently found to be correlated with a decision to admit or refuse a patient from ICU are bed availability, severity of illness, initial ward or team referred from, patient choice, DNR status, age and functional baseline. There has been very limited investigation of the actual decision-making process and the factors that are important to the accepting intensivists. The few small-scale studies that exist show that in general the factors which objectively correlate to admission decisions are subjectively considered by intensivists too, with other factors such as patient personality, which may be harder to capture in an observation objective study design. Even less research exists on referral decision, with only one small study investigating factors that are correlated with ICU referral and demonstrating that as well as the factors correlated with ICU admission decisions, other wider variables are considered by the referring non-intensivists. No studies are available that investigate decision-making process in referring non-intensivists or the mismatch of processes and pressure between the two sides of the ICU referral dilemma.
Further research should be focussed on factors relating to referral to ICU and how these may differ from those related to ICU admission. In particular, investigating these differences and how they arise from the decision-making process by referring and accepting clinicians may facilitate the referral process and allocation of limited resources in a more efficient manner. We would also recommend further investigation of how the international variation of health economics impacts on clinical decision-making. Finally, it would also be of benefit to analyse the complex factor of age in relation to ICU admission and how it appears to be clinically used as a surrogate for other factors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.