
Abstract
We conducted a literature review of the intensive care unit-acquired weakness syndromes (critical illness polyneuropathy, critical illness myopathy and critical illness neuromyopathy) with the primary objective of determining their incidence as a combined group. Studies were identified through MEDLINE, Embase, Cochrane Database and article reference list searches and were included if they evaluated the incidence of one or more of these conditions in an adult intensive care unit population. The incidence of an intensive care unit-acquired weakness syndrome in the included studies was 40% (1080/2686 patients, 95% confidence interval 38–42%). The intensive care unit populations included were heterogeneous though largely included patients receiving mechanical ventilation for seven or more days. Additional prespecified outcomes identified that the incidence of intensive care unit-acquired weakness varied with the diagnostic technique used, being lower with clinical (413/1276, 32%, 95% CI 30–35%) compared to electrophysiological techniques (749/1591, 47%, 95% CI 45–50%). Approximately a quarter of patients were not able to comply with clinical evaluation and this may be responsible for potential underreporting of this condition.
Introduction
Worldwide, the majority (70–80%) of patients admitted to an intensive care unit (ICU) now survive;1–5 follow-up has identified multiple sequelae with generalised weakness in particular found to be a common and troublesome problem.6–9 Whilst there has been major heterogeneity in terminology used to label this generalised weakness, a critical illness associated polyneuropathy, myopathy and neuromyopathy (where both neuropathy and myopathy coexist) have broadly been identified. These syndromes are now all included under the clinical diagnostic label of intensive care unit-acquired weakness (ICUAW). 10
The development of an ICUAW syndrome may have important consequences on patient outcomes; prolonged ventilatory weaning,11,12 increased ICU 12 and hospital length of stay, 13 increased hospital mortality,14,15 increased 180-day mortality 16 and persistent disabling weakness with reduced quality of life out to one year from ICU discharge.17–19 There may also be a number of potentially modifiable risk factors for ICUAW; prolonged ICU stay/bed rest,20,21 hyperglycaemia/insulin therapy,13,22–24 corticosteroids 20 and neuromuscular blockers. 14
Unfortunately, there is marked heterogeneity across the studies of ICUAW. A systematic review by Stevens et al. 13 highlighted, for example, the heterogeneity in the diagnostic criteria used. This currently makes drawing firm conclusions regarding ICUAW difficult and may partly explain some of the inconsistent findings across the studies, such as an incidence varying from 9% 25 to 86%. 26
With the increasing recognition that the ICU care we deliver needs to ensure the optimal functional outcome of patients, further study and a better understanding of ICUAW are important next steps. There have been a significant number of studies published8,15,16,23,24,27–32 since the previous systematic review supporting updating the estimate of the incidence of ICUAW. In addition, with the marked variation in diagnostic criteria used across studies, further investigation of this heterogeneity may be useful in identifying trends, for example in incidence, within the diagnosis. This may then allow more homogenous groups and their outcomes to be identified for intervention and prognostication.
Unfortunately, the inconsistent reporting of the diagnostic criteria precludes its influence on incidence from being evaluated directly. However, part of the heterogeneity within the diagnostic criteria may relate to the varying diagnostic techniques used – clinical, neurophysiological or histological examination. The diagnostic techniques used across the studies are adequately reported and could be used to identify any variation in the incidence of ICUAW according to the diagnostic technique used.
The aims of this review are: (1) to determine the approximate incidence of all the ICUAW syndromes as a group, (2) to determine the incidence of the ICUAW syndromes categorised by diagnostic technique (clinical, electrophysiological and histological diagnoses) and (3) to determine the incidence of failure of completion of diagnostic assessment and the attributable causes (that are not a lack of study consent) categorised by diagnostic technique.
Methods
Data sources and searches
The online databases MEDLINE, Embase and the Cochrane databases were searched from the period 1977 until 1 July 2011 to identify studies to include in this review. The search terms used were: muscle weakness, paresis, polyneuropath(y)/(ies), muscle hypotonia, muscular disease(s), intensive care unit(s), intensive care, critical care, critical illness, respiration artificial, artificial ventilation. These terms were mapped to the appropriate subject headings and ‘exploded’. The search was limited to studies published in English and those involving humans.
The title and abstract of all publications identified by the search strategy were screened, with the full text of all those describing an ICUAW syndrome reviewed. The reference list of each full text article reviewed was screened to identify additional relevant papers.
Study selection
Studies fulfilling the following eligibility criteria were included: (1) patients were admitted to an adult ICU, (2) patients were diagnosed with an ICUAW (critical illness polyneuropathy, critical illness myopathy or critical illness neuromyopathy), (3) sufficient data to calculate the incidence of an ICUAW was provided, (4) study patients were not potentially included in another study included in this review and (5) the full-length report was published. Patients with weakness attributed to a specific aetiology (e.g. spinal cord compression) were excluded.
Studies where the diagnostic criteria were either not consistent with a diagnosis of an ICUAW or were inadequate were excluded. Whilst there has recently been consensus diagnostic criteria published, 10 all studies included in this review recruited patients prior to this publication where diagnostic criteria were variable. The minimum criteria required for study inclusion were any of the following: (1) a new clinical diagnosis of generalised weakness determined by an objective clinical assessment tool (e.g. Medical Research Centre sum scores), (2) reduced compound motor and sensory nerve action potential amplitudes consistent with critical illness polyneuropathy, (3) normal sensory nerve action potential amplitudes with either of short duration, low amplitude motor potentials on electromyography (EMG) or low-amplitude motor potentials and nerve:muscle ratio >0.5 on direct muscle stimulation consistent with critical illness myopathy, (4) muscle histology consistent with critical illness myopathy or (5) a combination of neurophysiological abnormalities as given above consistent with critical illness neuromyopathy.
For the third question of this review addressing the incidence of failure to complete diagnostic testing, only papers presenting this information were included in this part of the analysis. The denominators abstracted from each paper for these calculations were the number of patients analysed in the study plus the number who were not included because of failure to complete the diagnostic evaluation.
Data extraction and quality assessment
A modified version of the validated Newcastle–Ottawa Scale (NOS) 33 with the addition of three further criteria suggested by Altman et al. 34 was used to appraise the observational studies. The NOS evaluates three domains; the selection of the study populations (range 0–4 points), the comparability of the study populations (range 0–2 points) and the assessment of the outcomes (range 0–3 points). The modified NOS we used had three additional assessments (objectivity of diagnostic criteria used (0–1 point), appropriateness of diagnostic criteria (0–1 point) and ability of diagnostic criteria to differentiate critical illness polyneuropathy (CIP), critical illness myopathy (CIM) and critical illness neuromyopathy (CINM) (range 0–2 points) within the outcome domain (range 0–7 points). The modified scale has a maximum score of 13 with a score of 0–4 being judged as a low-quality, 5–8 as medium-quality and 9–13 as a high-quality study. The modified NOS was agreed by the authors prior to commencing the review. Randomised controlled trials (RCTs) were appraised according to the Cochrane Collaboration’s assessment tool for risk of bias. 35 Each study was assessed by one of the authors for quality using these tools.
Data synthesis and analysis
Patient, illness, treatment and study design data were abstracted using a standardised data collection sheet and collated in Excel (Microsoft Corporation Redmond, WA, USA). Professional statistical advice was obtained and confidence interval (CI) analysis (95% CIs) on proportions using aggregated original study data was performed by one of the study authors using Confidence Interval Analysis Version 2.2.0 (University of Southampton, UK, 2000–2011).
Results
Study search and selection
The results of the literature search are shown in Figure 1; 33 studies including 2686 patients were evaluated in this review. The characteristics of the included studies are shown in Table 1. Of the 33 studies, 27 were prospective cohort studies, two were retrospective cohort studies and four were randomised controlled trials.
Literature search results. Study characteristics. Note: ICUAW, intensive care unit-acquired weakness; SD, standard deviation; IQR, inter-quartile range.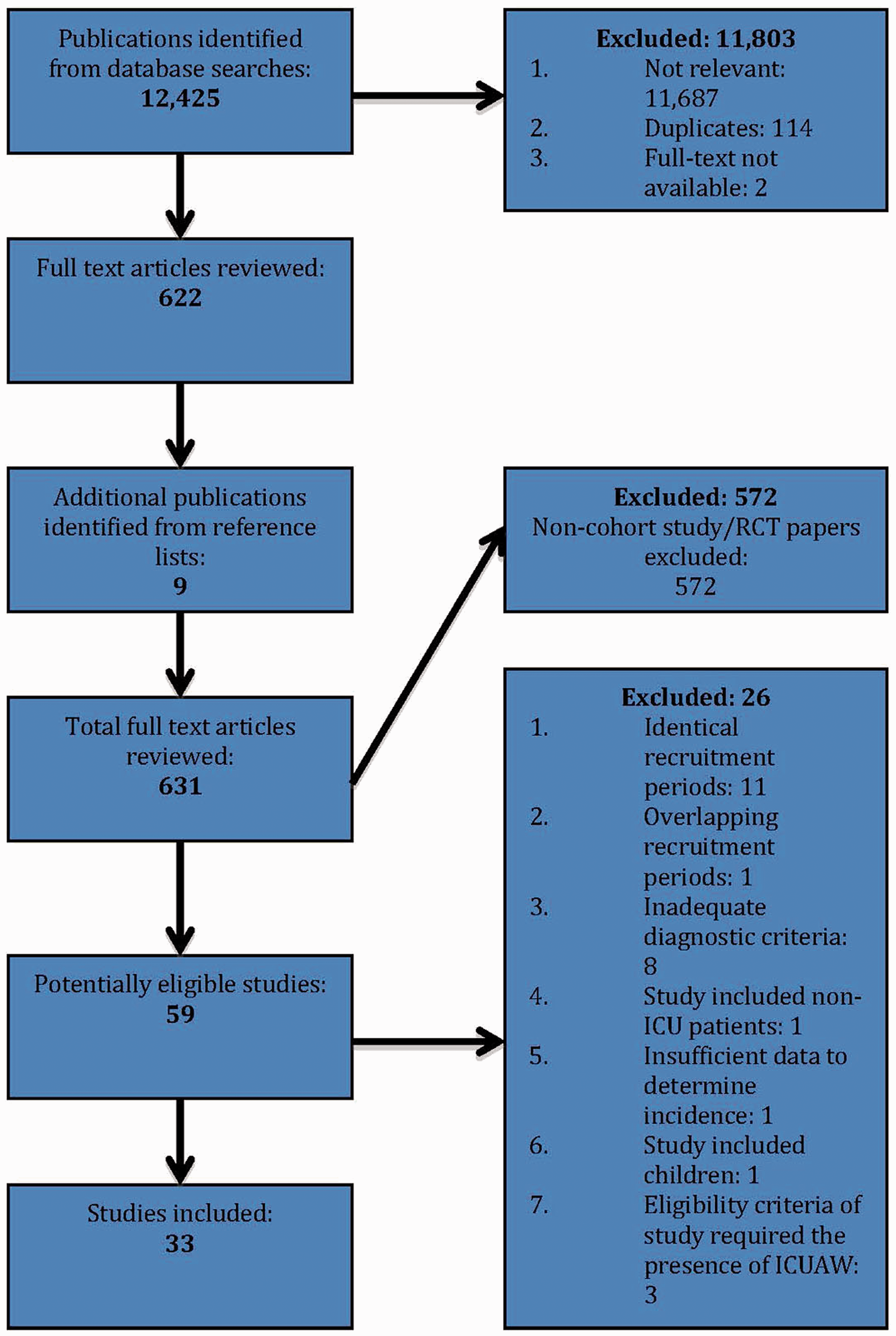

Quality of included studies
Eleven out of the 29 (38%)25,28,29,32,36–42 observational studies were graded of low quality, 17 out of 29 (59%)12,14–16,20,24,26,27,30,43–50 as medium and one (3%) 51 as high quality. There were four RCTs included; two studies were deemed of low risk,22,23 one unclear risk 8 and one with high risk 31 of bias.
Incidence of ICUAW
Incidence of ICUAW.
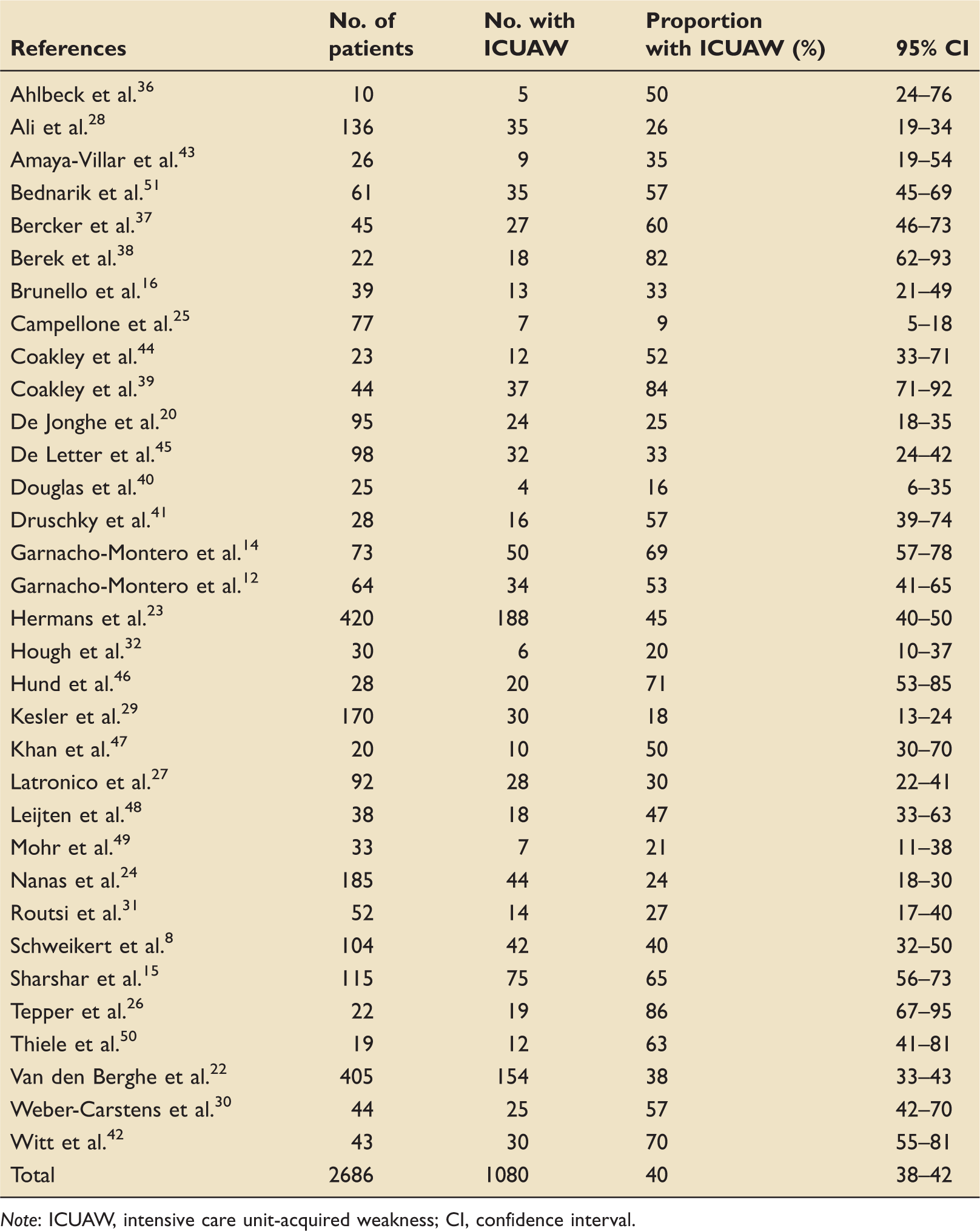
Note: ICUAW, intensive care unit-acquired weakness; CI, confidence interval.
Incidence of ICUAW by diagnostic technique
Incidence of ICUAW in subgroups according to diagnostic technique.

Note: ICUAW, intensive care unit-acquired weakness; CI, confidence interval.
Failure of completion of diagnostic assessment
Incidence of failure of completion of diagnostic assessment according to diagnostic technique.

Note: CI, confidence interval.
The reasons for failure to complete the clinical assessment were the combination of inadequate patient awakening and comprehension (377/381 [99%] patients), generalised pain (1/381 [0.2%] patients) and patient refusal to cooperate (3/381 [0.8%] patients). The reasons for failure to complete the electrophysiological assessment were inadequate patient compliance (11/17 [65%] patients) and technical problems (6/17 [35%] patients). The electrophysiological diagnostic criteria used across the studies were such that in only four of 17 (24%) studies was patient compliance actually required. In these studies, failure of diagnostic assessment because of inadequate compliance was 13% (11/83 patients).
Discussion
There are three main findings from this systematic review. First, the approximate incidence of the ICUAW syndromes as a group was 40% (95% CI 38–42%). Second, the incidence of the ICUAW syndromes when diagnosed clinically was significantly lower (32%, 95% CI 30–35%) than when diagnosed electrophysiologically (47%, 95% CI 45–50%). Finally, the incidence of failure of diagnostic assessment was significantly higher with a clinical diagnostic technique (26%, 95% CI 24–28%) compared to an electrophysiological technique (2%, 95% CI 1–4%).
There are two published systematic reviews in this area,13,52 the most recent included studies up until 2006. This review adds approximately a further 1200 patients and 12 new studies to this work. The incidence of ICUAW in this review is lower than in those done previously (60% 52 and 46% 13 ). The still sizeable incidence of ICUAW reflects the populations studied: those requiring mechanical ventilation beyond approximately seven days, patients with severe sepsis, multiple organ failure or conditions treated with relatively high doses of steroids.
This review is the first to evaluate the incidence of the ICUAW syndromes according to the diagnostic technique. The significant difference in incidence found between the groups diagnosed with a clinical technique compared to an electrophysiological technique may be explained by the techniques themselves (a lack of concordance between clinical and electrophysiological findings37,51) and/or by other methodological differences; differing rates of successful completion of testing, variation in the frequency of assessments, the timing of the diagnosis and study population heterogeneity. We did not find a detectable difference in study quality between the clinical and electrophysiological technique groups to explain the difference.
This review found that there was a significant difference in the proportions of patients unable to complete clinical assessment (26%, 95% CI 24–28%) compared to electrophysiological assessment (2%, 95% CI 1–4%). The major cause of this was a lack of patient compliance with clinical assessment. Patients unable to comply with clinical assessment tend to have a higher mortality rate15,16,20,28 and potentially have greater encephalopathy, both of which are associated with increased incidences of ICUAW.14,20,23,42,51 The lower incidence of ICUAW in the group diagnosed on clinical assessment is likely to be explained in part by higher rates of incomplete testing.
The strengths of this review include the detailed literature search, the systematic evaluation of included studies with an objective assessment tool and the inclusion of studies utilising the full range of recognised diagnostic techniques. There are limitations to this review. This review was largely the work of a single reviewer with the risk of introducing bias both in the selection of studies to include and in the assessment of included studies. To minimise this risk, clear criteria were set for each domain on the study appraisal form which were used both to assess eligibility for the review and to appraise the quality of the study.
The tool we used to grade the evidence was a modification of the NOS 33 with additional criteria recommended by Altman. 34 The rating scale was modified after a pilot run because the NOS was felt not to adequately discriminate between the different qualities of studies. This is therefore a new tool that is unvalidated and may not have appropriately graded all of the studies. The modified scale did however provide an objective assessment tool that appeared to be appropriate for the majority of the studies.
Conclusion
This systematic review has provided a comprehensive update to those done previously and found that the ICUAW syndromes are common (40%) in the groups of ICU patients requiring more than approximately a week of mechanical ventilation. The incidence of ICUAW varies with the diagnostic technique used, being lower with clinical compared to electrophysiological techniques. Approximately a quarter of patients will not be able to comply with clinical evaluation and this may be responsible for underreporting of this condition. Further research is required to validate the 2009 consensus diagnostic criteria and to identify the optimal method and time point for identifying this problem to then allow interventions to be evaluated and introduced.
Footnotes
Acknowledgements
The authors would like to thank Dr David Young, Statistician, University of Strathclyde, for statistical advice and Amanda Wright, Librarian, Gartnavel General Hospital, for her assistance with the literature search.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.