
Abstract
The system of trauma care has been revolutionised over the last decade with the introduction of major trauma networks across the United Kingdom and the development of subspecialist national training in pre-hospital emergency medicine. Pre-hospital care providers feed trauma patients into trauma units or major trauma centres depending upon the severity of their injuries and their stability for a potentially longer primary transfer to access specialist major trauma services. Trauma services are continually adapting and improving with the introduction of more advanced techniques into the pre-hospital arena are on the horizon, enabling trauma patients to receive more specialised treatment from medical professionals earlier after injury; this article will discuss some of the recent developments within pre-hospital emergency medicine, in-hospital trauma care and on into the intensive care unit, and how this has led to improved outcomes.
Introduction
The two specialties of pre-hospital emergency medicine (PHEM) and trauma intensive care have developed significantly over the last twenty years and are now intertwined with each other through the UK major trauma network. Pre-hospital medicine has previously been the domain of ambulance paramedics and technicians, but as paramedics are increasingly seen working in emergency departments (ED) and GP surgeries, so doctors are working increasingly in the prehospital environment, offering a wide range of skills and treatment options than might have previously been unavailable. The skills required to be proficient in pre-hospital medicine are similar to those required by the trauma intensivist stabilising patients in the emergency department, but in addition require self-sufficiency and an ability to work with less backup and fewer resources, within an increasingly robust and regulated system.
Pre-hospital emergency medicine
Pre-hospital emergency medicine is delivered by a variety of agencies in the United Kingdom:
Ambulance service trusts – provide the vast majority of responses and work from the level of ambulance technicians up to paramedic, specialist paramedic and doctor-led Medical Emergency Response Incident Teams (MERIT). Air ambulances – provide Helicopter Emergency Medical Services (HEMS) and in England and Wales operate as charities. The Scottish Ambulance Service operates HEMS as part of their NHS role. The British Association for Immediate Care (BASICS) – has local schemes across the United Kingdom where medical professionals volunteer to provide immediate care at the scene of accidents and medical emergencies. Levels of pre-hospital practitioner. CCT: certificate of completion of training; GMC: general medical council; PHEM: pre-hospital emergency medicine.
There is now a wide range of skills and experience offered by those who provide pre-hospital medicine. These are summarised in Table 1.
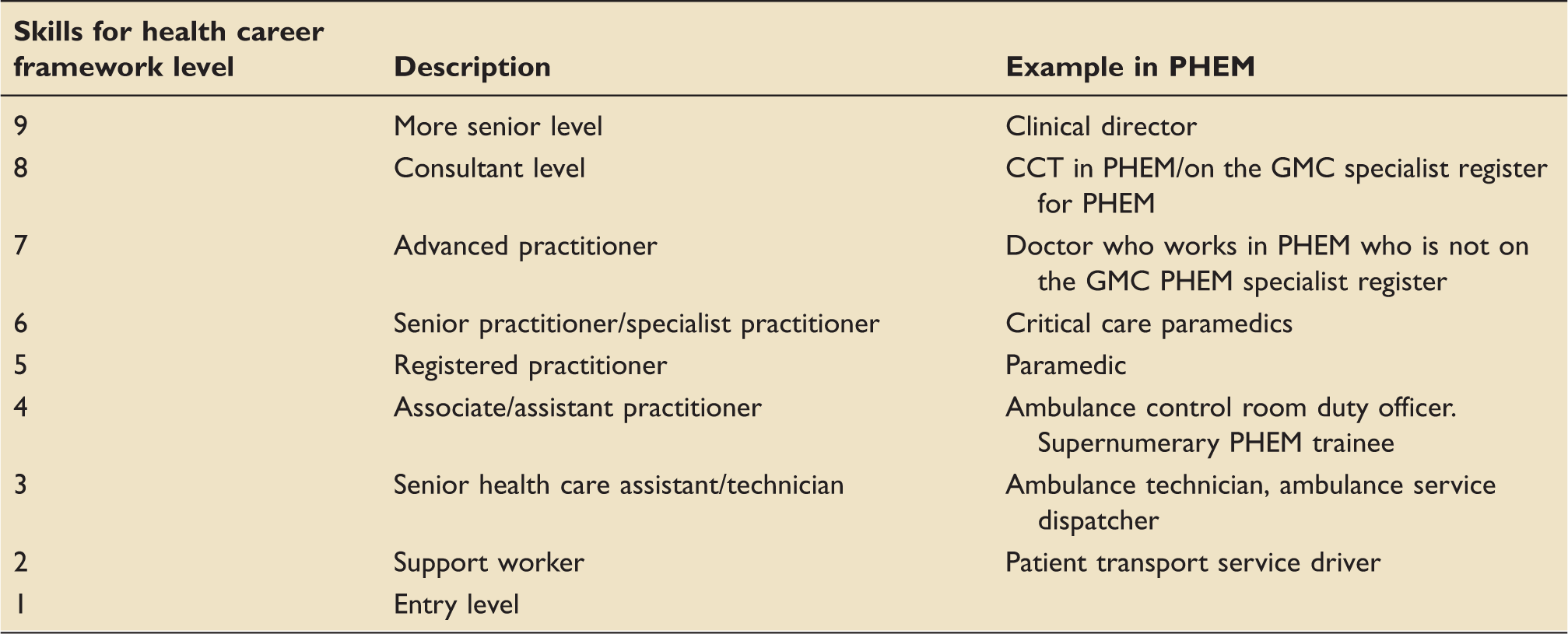
Historically, medical training in PHEM has been rather ad hoc through local fellowships. A national training scheme was introduced in 2014 with applications for subspecialty training now accepted from trainees in acute medicine, emergency medicine, anaesthetics and intensive care medicine. The training program is a year of whole time equivalency training in pre-hospital emergency medicine covering clinical and non-clinical domains; those completing the training program as well as their primary CCT are eligible for entry onto the specialist register for PHEM to practice at level 8.
The role of PHEM
There is increasing evidence that optimal prehospital care, offered earlier after the injury, improves outcome, and PHEM doctors commonly work with other prehospital professionals to improve care in the very early stages. The 2007 National Confidential Enquiry into Peri-Operative Deaths (NCEPOD) ‘Trauma: Who cares’ report 1 found that 9.6% and 8% of severely injured trauma patients had an inadequate airway and ventilation respectively on arrival in hospital; a rapid sequence induction (RSI) of anaesthesia and intubation to optimise oxygenation and ventilation performed before the patient reaches hospital may be of benefit1,2 and can be as safe as in-hospital RSI. 3 Current NICE guidelines recommend that a drug-assisted intubation is performed within 45 min of the incident, and providing resources for this to happen prior to hospital is advocated. 4
The concept of the ‘golden hour’ is familiar to in-hospital trauma physicians; similarly, an on-scene time of less than 10 min (the ‘platinum 10 min’) has been advocated. 5 However, many of the interventions previously performed in hospital may now be performed by PHEM clinicians, which may justify longer on-scene times. 1 Prehospital echocardiography and ultrasound to identify time-critical life-threatening injuries in the primary survey are becoming more popular.
Adequate triage and identification of injuries is important to identify patients who would benefit from care in an MTC. Some paramedics undergo extended training to specialise in critically ill patients; others gain experience in minor injuries and illnesses, allowing pre-hospital clinicians to treat more patients or signpost to alternative pathways (e.g. minor injury units, or an outpatient review) to reduce the numbers attending the Emergency Department.
The UK Trauma Network
The concept of regional trauma networks was developed to improve the management of patients sustaining major trauma. The NCEPOD ‘Trauma: Who cares’ report, 1 and the National Audit Office ‘Major Trauma Care in England’ report 6 had identified a lack of coherence, structure and senior leadership for this group of patients, resulting in poor outcomes and potentially preventable deaths. The severity of trauma is classified using the Injury Severity Score (ISS); this system assigns an Abbreviated Injury Scale score to each injury. The scores are then allocated to body regions, and the values from the three body regions with the highest total scores are squared and summated. By convention, patients who have sustained injuries consistent with an ISS greater than 15 are defined as having suffered from major trauma and those with an ISS of 9–15 have suffered moderately severe trauma. 7 Patients with a score greater than 8 would ideally be managed in a Major Trauma Centre (MTC); however, it is not possible to calculate the ISS at the point of triage (it is a research tool), so there are protocols for the PHEM team to determine the appropriate destination for injured patients.
The UK Trauma Network operates on a hub-and-spoke model, which involves all providers commissioned to deliver trauma care services within a geographical area; including pre-hospital services, a Major Trauma Centre, all other hospitals receiving acute trauma admissions (‘Trauma Units’), and regional rehabilitation services. Figure 1 gives an example of how such a service operates.
The South of England major trauma system.
8
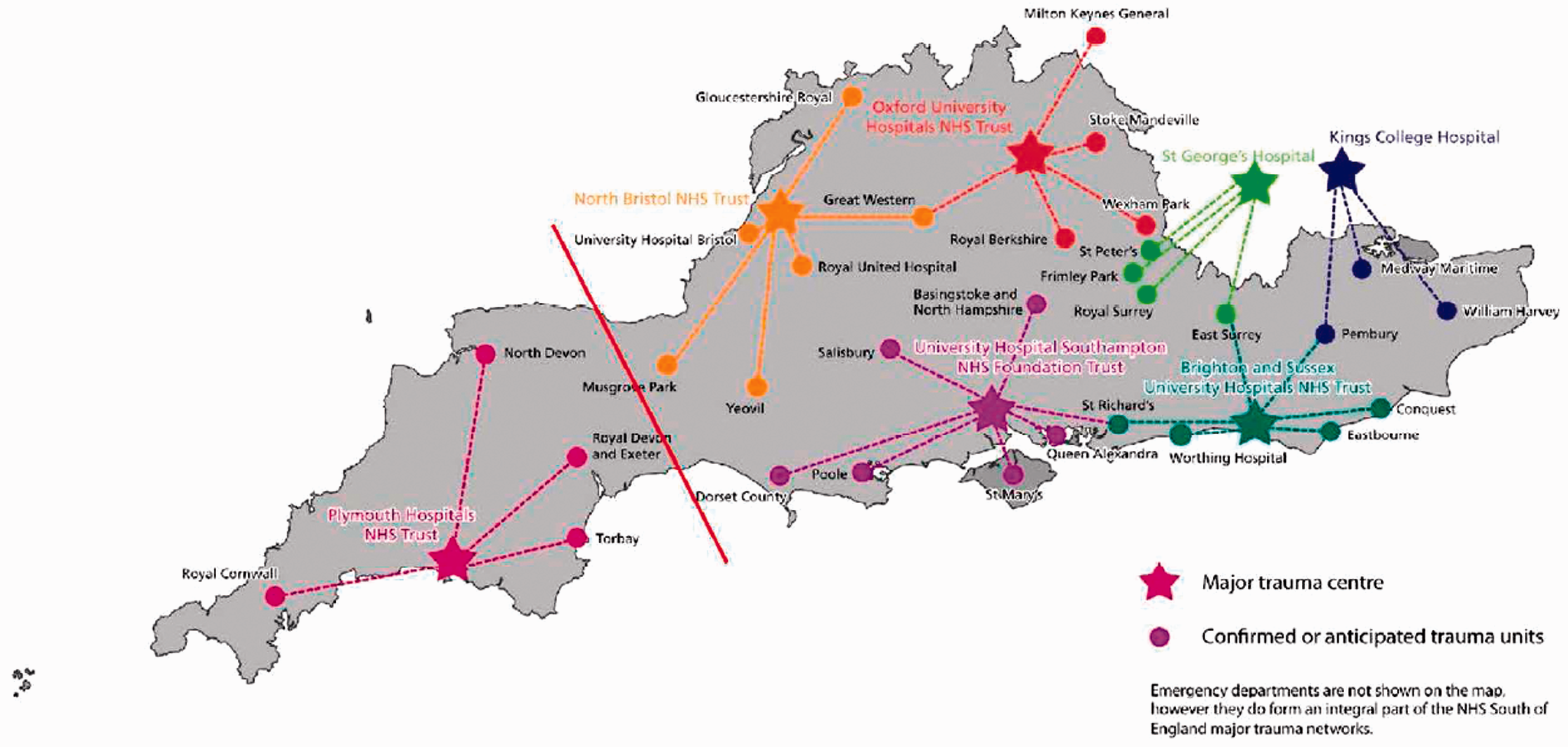
A Major Trauma Centre has the resources to provide all the high-quality specialist services required to receive and manage injured patients on one site, with full assessment and diagnostics in the emergency department and consultant-level care throughout. 2 There are three types of MTC – those that treat adults, those that treat children and those that treat both. There are 27 MTCs in England. Figure 2 shows the locations and types of MTC across England. Since the introduction of trauma networks, severely injured patients treated in an MTC have a 20% improvement in mortality compared with previously. 10 Treatment at an MTC is associated with good recovery in 62·3% patients, compared with 55% treated elsewhere. 11
A trauma unit (TU) is a hospital within a trauma network that provides care for most injured patients, but without the full spectrum of acute and rehabilitation services offered by an MTC. It can provide some specialist services for patients who are not multiply injured and can stabilise and transfer patients for escalation of care when required.
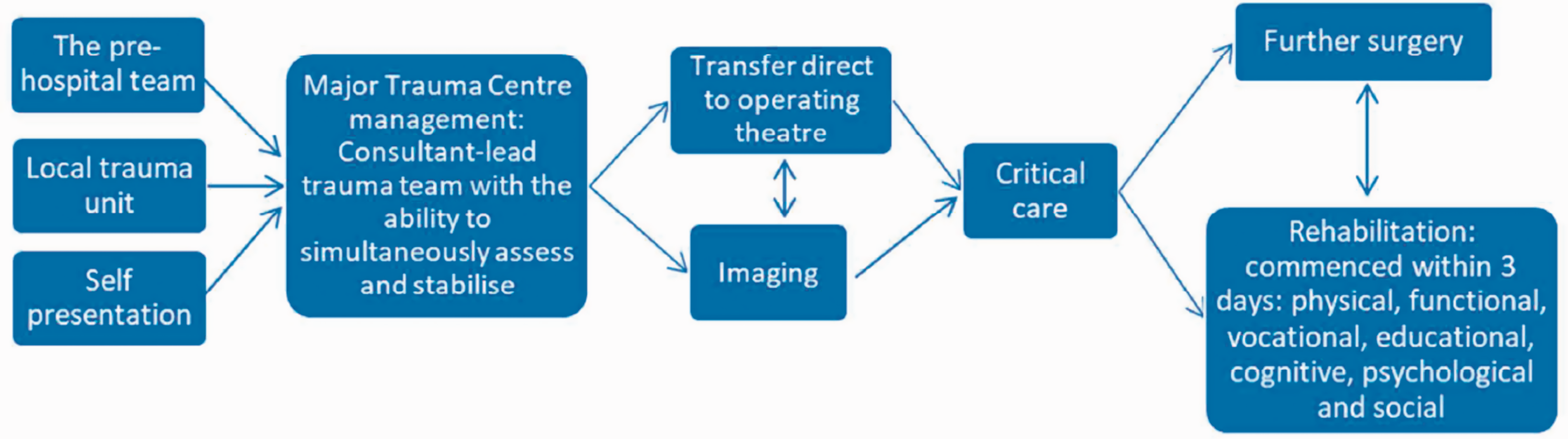
The interface between prehospital services and local trauma networks includes the decision by the prehospital care provider as to if a patient requires management in a major trauma centre and whether they are stable enough to bypass a trauma unit to undergo primary transfer. Figure 3 shows an example of the patient journey through the major trauma system.
Severely injured patients may need to be initially managed in a peripheral trauma unit for several reasons:
12
An unmanageable airway at the scene, MTC more than 60 min away, Self-presentation, Injuries initially thought not to be severe enough to warrant MTC treatment, but progress, or the severity only becomes apparent later.
Following stabilisation at the TU, a decision can be made to transfer to an MTC or to continue with management locally. The decision to transfer will be dependent on the services required for the patient, for example cardiothoracic surgery, neurosurgery or burns, as well as the urgency with which the patient requires specialist care, balanced against their stability.
Improvements in trauma care
Functional disability and mortality have both improved with recent improvements in trauma care. 1 In addition to improved structure of trauma networks, and the infrastructure within hospital, recent clinical improvements include improved access to imaging, clearer understanding of fluid and blood resuscitation, and the administration of tranexamic acid. Timely whole-body CT imaging is recommended once the primary survey and life-saving interventions have been performed and is associated with a 25% reduction in mortality compared with non-whole body or no CT. 13
The concept of hypotensive resuscitation is not new14,15 and aims to achieve adequate perfusion but minimising the risk of clot disruption. Current guidelines advocate that fluid should only be given in the absence of a radial pulse (or a central pulse for penetrating torso injuries) in adults and older children. Crystalloids should be avoided, and if blood products need to be given, one unit of fresh frozen plasma should be given with every unit of packed red cells to minimise coagulopathy. 12 There is, however, room for improvement – the NCEPOD ‘Trauma: Who cares’ report estimates that 12.8% of severely injured patients received inappropriate fluid resuscitation. 1
Thirty-five percent of the deaths in the CRASH-2 trial were due to bleeding, and coagulopathy is commonly seen; tranexamic acid reduces mortality from 7.7% to 5.3%, if given within 1 h of trauma, and is recommended in all trauma patients bleeding or at risk of bleeding. 16 Conversely, tranexamic acid after 3 h of trauma has been shown to worsen survival. 17
The trauma intensive care unit
The provisions for managing trauma patients within critical care depend on whether the critical care unit is located within an MTC or a TU.
In general, all critical care units accepting trauma patients need staff who are familiar with managing such injuries, as well as access to cross-speciality supporting services including pain management and rehabilitation medicine. 7 General multiple-organ support, ability to provide massive transfusions of blood products if required, and the facilities and staff to image and transfer critically ill patients are necessary for all trauma critical care units.
Within a specialist centre, it is possible to provide more advanced organ support including ECMO and more advanced monitoring such as intracranial pressure measurement. Staff are familiar with managing patients following damage control surgery.
Intensive care units in the major trauma centres will care for the vast majority of high acuity trauma patient and thus tend to have the input from the specialist services required by trauma patients during their initial stabilisation and subsequent recovery. These include:
Acute surgical services including neurosurgery; Interventional radiology for the control of non-compressible haemorrhage; Haematological expertise both medical and laboratory based for blood product support and advice; Trauma coordinators bridging the gap between the emergency department and the intensive care to ensure that less serious injuries are not missed; Physiotherapists are key members of the rehabilitation team – a process that starts as early as possible to maximise functional recovery; Occupational therapists work alongside physiotherapists to provide patient support and physical aids adapted to patients along their rehabilitation pathway; Speech and language therapists assist with the assessment of swallowing and feeding alongside dietitians as well as aiding patients who have communication difficulties as a result of their injuries.
Legal services are important for trauma patients who usually have a short-term inability to look after their own financial affairs.
Special circumstances
Paediatric trauma: There are just five dedicated paediatric major trauma centres in England and 11 combined adult and paediatric MTCs. One of the implications of this is that paediatric traumas will more frequently be stabilised at a local hospital and then transferred. The 2012 ‘Severe Injury in Children’ TARN study, 18 which looked at all patients from 2012 with an ISS > 15, aged less than 16 years, found that there were several differences in the patient journey for paediatric trauma patients, meaning that adaptations are required. Firstly, this group of patients includes under 2-year olds suffering from non-accidental injury: data from the study found that this accounted for 10% of paediatric trauma patients with an ISS > 15. A significant proportion of severely injured children (26%) do not arrive by ambulance and therefore do not undergo the pre-hospital triage meaning that patients who ideally would be managed at an MTC from presentation may actually need to be stabilised in peripheral TUs or minor injury unit which would not routinely accept trauma patients. Transfers for paediatric patients may be arranged by paediatric retrieval teams or by the referring hospital. Retrieval teams have more specialist knowledge, skills and equipment but the transfers typically take longer as teams go out from the regional paediatric centre. For time critical transfers, for example head injuries, the local hospital needs to provide this service. The responsibility for these transfers often fall to adult intensive care physicians within the trauma unit hospitals.
Chest injury: Patients who have sustained blunt chest trauma are a group requiring early, specialist intervention as they have a high risk of deteriorating with severe respiratory failure. If immediate intubation is not indicated then patients should ideally be commenced on humidified high flow oxygen therapy; haemopneumothoraces should be managed appropriately at an early stage; and adequate analgesia needs to be rapidly established to prevent subsequent hypoventilation – this usually would include a regional anaesthetic technique. Commencement of early physiotherapy is also important but requires appropriate pain management to be effective.
Patients who should be monitored on critical care following blunt chest trauma include those who have four or more rib fractures and are elderly (65 years or above) or have underlying cardiovascular or respiratory disease. Patients with signs of impending respiratory failure should also be admitted; this includes those with deteriorating gas exchange, increased work of breathing, inadequate cough despite good analgesia or radiological evidence of significant early pulmonary contusion. 19 In addition to standard care, rescue techniques including ECMO and one-lung ventilation to improve VQ matching may be needed. Surgical rib fixation can be considered for flail segments, which has been associated with a reduced incidence of pneumonia,20–22 reduced duration of mechanical ventilation 22 and a reduced length of stay in ICU.20,22 Current recommended indications for surgical fixation include more than 3–5 rib fractures, if there is significant displacement, especially if mechanical ventilation is required. 19
The future
Advances in trauma and pre-hospital care have been numerous in the last 10 years, partly at least fuelled by innovations pioneered by the Defence Medical Services in recent conflicts. Further developments in the provision of advanced interventions in the pre-hospital environment are expected in the near future. Future potential pre-hospital innovations include:
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA): Extra Corporeal Membrane Oxygenation (ECMO):
An approach to controlling non-compressible haemorrhage in the torso without the need for an invasive resuscitative thoracotomy to compress the thoracic aorta. A balloon in introduced via the femoral artery and inflated within the descending aorta to control haemorrhage and increase perfusion to the brain and coronary arteries. It may be sited within the thoracic or abdominal cavity (with most services starting their provision of this intervention with the latter only) and is a bridge to buy time for transfer to a major trauma centre when definitive haemorrhage control can be achieved by surgery or interventional radiology. Some UK providers already provide this intervention in the pre-hospital environment and this is likely to be expanded to several other services.
Currently not practiced in the United Kingdom but almost certainly will be in the future based upon the experiences of its use in Paris.
23
Pre-hospital ECMO may have an early role supporting patients in cardiac arrest, known as extra-corporeal cardiopulmonary resuscitation (ECPR).
This intervention should only be offered to those for whom it is likely to provide benefit – allowing oxygenation of the brain and other vital organs to allow time for transport to specialist centres for (for example) percutaneous coronary intervention.
Conclusions
Medical care offered to trauma patients has undergone significant improvements in the last few decades. There is a more cohesive system, from the site of the injury, through to the emergency department and on into the intensive care unit, and this, combined with evidence-based treatment protocols, has seen an improvement in mortality and functional disability.
A map showing the location of Major Trauma Centres across England.
9
An example of patient flow through the major trauma system.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.