
Abstract
Objective
To identify factors associated with intensive care unit (ICU) admission in patients with traumatic thoracic injury.
Methods
Data for consecutive patients with thoracic trauma were collected prospectively. Outcomes were requirement for ICU care and prolonged (>7 days) ICU care.
Results
The study included 1333 patients, 484 (36.3%) of whom received ICU care: 125 of these (25.8%) received prolonged ICU care. Head injury, abdominal injury, injury severity score ≥16, haemothorax, chest tube placement and spinal surgery were significantly associated with ICU care. Head injury, number of rib fractures, chest drain placement, spinal surgery and extremity surgery were independent risk factors for prolonged ICU care.
Conclusions
Associated injury factors played a more prominent role than thoracic factors in the need for ICU and prolonged ICU care. A multidisciplinary trauma team (involving neurosurgeons, abdominal surgeons, orthopaedic surgeons and thoracic surgeons) is essential for the care of patients with traumatic thoracic injury.
Introduction
In Taiwan, trauma is the leading cause of death in those aged <50 years. 1 Thoracic trauma is directly responsible for ∼25% of trauma-related deaths worldwide and is a contributing factor in a further 25% of deaths.2–7 Thoracic trauma leads to respiratory failure, pneumonia, pleural sepsis and death.3,7,8 The combination of thoracic trauma and other associated multiple organ injuries results in even higher mortality rates, and is likely to require close monitoring and treatment in an intensive care unit (ICU) setting.3,7,8
To the best of our knowledge, there are no data available regarding factors that predict ICU treatment in patients with thoracic trauma and related injuries. An understanding of these factors may enable appropriate treatments to be administered more rapidly than is currently possible; these might include earlier initiation of tracheotomy and specialist bedside rehabilitation in those at risk of prolonged ICU stay. The aim of the present study, therefore, was to identify risk factors for ICU treatment in patients with thoracic trauma.
Patients and methods
Study population
This prospective study included consecutive patients with thoracic trauma admitted to the Department of Thoracic Surgery, Tungs’ Taichung MetroHarbor Hospital, Taichung, Taiwan, ROC (a level I trauma centre) between March 2005 and December 2008. Exclusion criteria were: (i) patients treated in an outpatient setting or transferred to another institution; (ii) age <18 years; (iii) patients admitted to the Department of Cardiovascular Surgery with cardiac or great vessel involvement whose care did not involve the Department of Thoracic Surgery (due to limited availability of cardiac enzyme and cardiac echo tests for diagnosis of mild heart injury). 9
Data including sex, age, admission and discharge dates, duration of hospital and ICU stay, injury severity score (ISS), type of injury, associated injuries, treatments received and mortality were collected from hospital medical records. Surgery and associated injuries were classified according to the body part involved (head injury, facial bone fracture, spinal injury, clavicle fracture, extremity fracture or abdominal injury). Soft tissue injuries were not included in this study.
The study protocol was approved by the institutional review board of Chung Shan Medical University Hospital, Taichung, Taiwan. Patient consent was not required.
Statistical analyses
Statistical analyses were performed on three separate databases: all patients with thoracic trauma; patients admitted to the ICU; patients with prolonged ICU stay (>7 days). Risk factors for ICU admission were chosen on the basis of literature review and according to criteria identified by the ISS.7,8,10–12 Data are presented as mean ± SD (range), or n (%). Univariate analyses were performed using χ2-test or Student’s t-test (when n ≥ 5) as appropriate, or Fisher’s exact test (when n < 5; for sternum fracture and stab injury). The total number of rib fractures was analysed using χ2-test for trend and Student’s t-test for comparison. Injury and treatment factors that were statistically significant following univariate analysis were included in multivariate analysis using backward stepwise logistic regression. In the multivariate analysis, injury and treatment factors were examined independently as separate groups. The resulting significant injury and treatment factors were considered jointly in multivariate analysis. Finally, the significant factors were analysed in combination with ISS ≥ 16 using multivariate analysis. P-values < 0.05 were considered statistically significant. Statistical analyses were performed using SPSS® software, version 17.0 (SPSS Inc., Chicago, IL, USA) for Windows®.
Results
The study included a total of 1333 patients with thoracic trauma (972 male/361 female; mean age 51.0 ± 16.6 years; age range 18–95 years), of whom 484 (36.3%) received ICU care (364 male/120 female; mean age 50.2 ± 17.5 years; age range 18–95 years). Of the patients who were treated in the ICU, 125 (25.8%) received prolonged care (>7 days; 96 male/29 female; mean age 50.4 ± 18.1 years; age range 18–91 years). There were no statistically significant between-group differences in patient age or sex distribution. A single patient with rupture of the inferior vena cava from thorax to abdomen was initially included in this study but was later excluded.
Demographic and clinical characteristics of patients with thoracic trauma, stratified by their requirement for intensive care unit (ICU) treatment.

Data presented as n (%).
Versus total patient group; χ2-test.
Versus ICU group; χ2-test.
χ2-test for trend. Patients without rib or sternum fracture were excluded.
ISS, injury severity score; NS, not statistically significant (P ≥ 0.05; χ2-test).
Demographic and clinical characteristics of patients with thoracic trauma injury, stratified by their requirement for intensive care unit (ICU) treatment. Results of univariate analysis of factors associated with ICU and prolonged ICU stay.
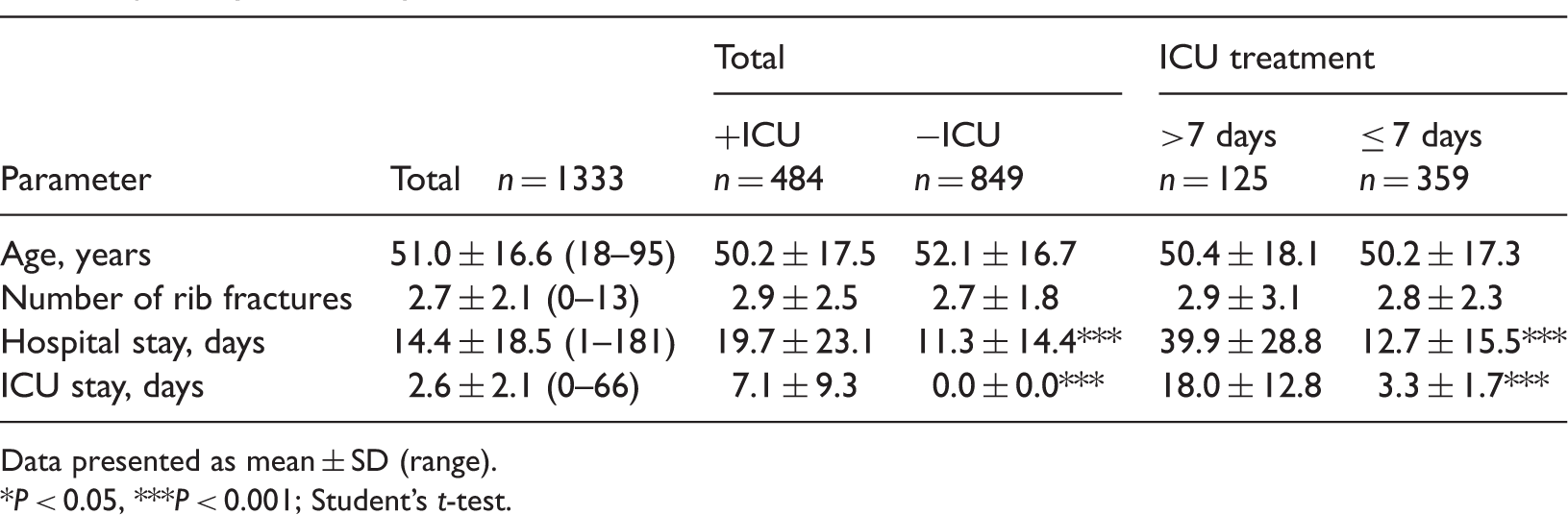
Data presented as mean ± SD (range).
P < 0.05, ***P < 0.001; Student’s t-test.
Backward stepwise logistic regression analysis of injury and treatment factors associated with intensive care unit treatment in patients with thoracic trauma.
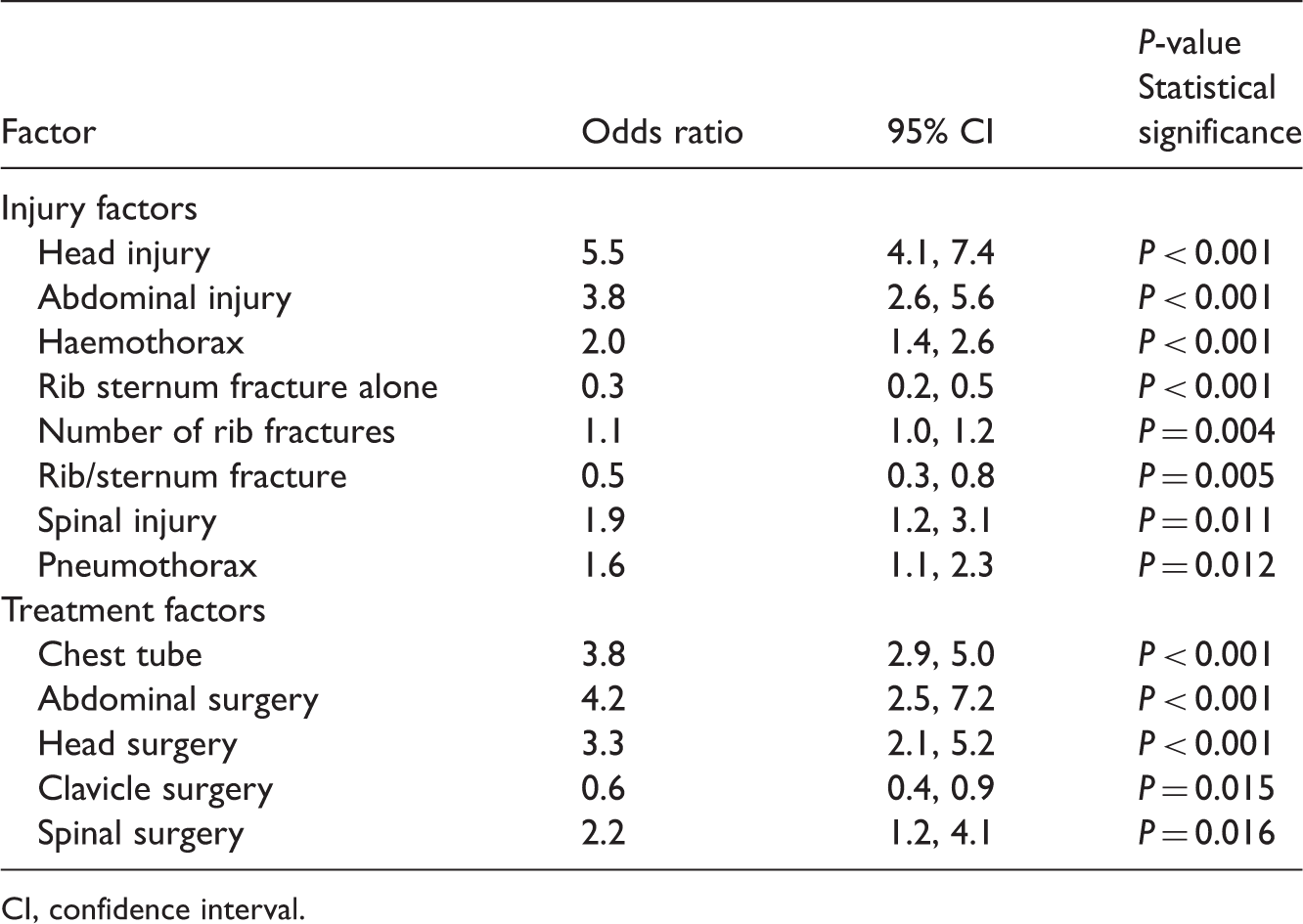
CI, confidence interval.
Backward stepwise logistic regression analysis of combined injury and treatment factors associated with intensive care unit treatment in patients with thoracic trauma.

Injury severity score (ISS) ≥ 16 was a significant factor with odds ratio 2.3 (95% CI 1.6, 3.4).
No longer statistically significant with the addition of ISS ≥ 16.
CI, confidence interval.
Backward stepwise logistic regression analysis of injury and treatment factors associated with prolonged intensive care unit (ICU) treatment (>7 days) in patients with thoracic trauma.
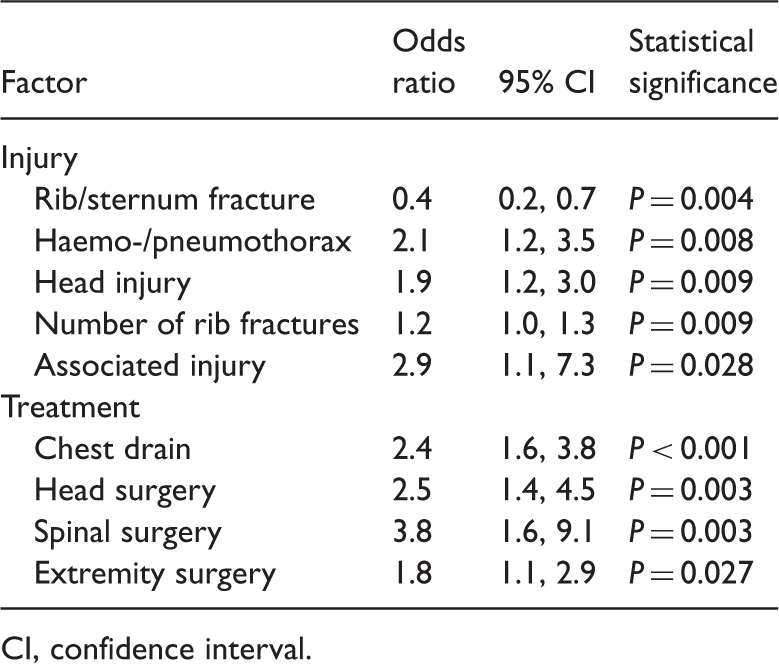
CI, confidence interval.
Backward stepwise logistic regression analysis of combined injury and treatment factors associated with prolonged intensive care unit treatment (>7 days) in patients with thoracic trauma.

CI, confidence interval.
Discussion
Thoracic trauma comprises 6% of all traumas but accounts for up to 50% of trauma-related deaths.2–7 Given the severity and the socio-economic impact of thoracic trauma, a focused study on the critical care of these patients is warranted. The present study investigated 1333 patients admitted to the Department of Thoracic Surgery in a single institution to determine factors associated with the need for ICU care. The study population reflected the precarious nature of thoracic trauma patients, with 36.3% requiring ICU treatment.
The predominance of male patients and the age distribution in the present study were consistent with data regarding total accidents in Taiwan (male/female ratio 2.85–2.97, age range 40–60 years), 1 although the age range was a little higher than figures reported in Germany or Pakistan.10,12 The durations of stay in the ICU and hospital in our study were similar to those reported elsewhere. 10 In addition, our finding that 85.5% of deaths occurred within 7 days of injury is consistent with other research, 10 underlining the importance of medical care within this period. The cut-off point for prolonged ICU care was chosen as 7 days in response to data indicating a high in-hospital death rate for patients requiring surgical ICU care for ≥ 7 days. 13
Although the focus of the present study was thoracic trauma, associated injuries (including head and abdominal injuries) were stronger risk factors for ICU treatment than thoracic parameters. Head injury was the most important and most common injury factor associated with ICU and prolonged ICU stay in the present study. This is consistent with studies which show that head injury is the most frequently reported associated injury in patients with thoracic trauma.8,12 Neurological trauma has been associated with poor prognosis in patients with thoracic trauma. 14 Patients with thoracic trauma often present with injuries at multiple sites that require treatment by more than one medical department. 15 In addition, patients with thoracic trauma and concurrent head injury who present with disturbed consciousness or positive imaging findings require ICU admission for close observation and treatment. Spinal surgery and abdominal injuries were also significant risk factors for ICU treatment in the present study, suggesting that concurrent injuries to the central axial plane of the body are associated with ICU admission.
Haemothorax was the most important thoracic factor associated with ICU admission in the present study. The number of rib fractures was also significantly associated with the need for ICU treatment, with the requirement for ICU admission increasing with increasing numbers of fractures. This finding is consistent with a report identifying the number of rib fractures as an indicator for trauma severity. 14
Injury factors that contributed to prolonged ICU stay in the present study were those to the head or haemo-/pneumothorax, together with increased number of rib fractures and associated injury. Significant treatment factors included chest drain and surgery at sites other than the chest, with prolonged ICU stay mainly due to these treatment factors.
Chest drain was the most common procedure performed in the present study, consistent with the data of others. 12 Chest tube was a significant risk factor for ICU stay, and chest drain was significantly associated with prolonged ICU treatment. Chest tube complications are known to be associated with longer duration of ICU and hospital admission. 16 Further studies are needed to define the causative role that chest tube placement plays in thoracic trauma patients under critical care settings.
There are several different trauma scoring systems to facilitate early identification of patients at risk of mortality and morbidity due to thoracic trauma.8,10,17,18 We used an ISS score ≥16 as a thoracic trauma severity indicator because the Taiwan Bureau of National Health Insurance issues a waiver of copayment based on this criterion. ISS ≥16 was found to be an important prognostic factor associated with ICU admission, in accordance with data indicating that ISS is an independent predictor of the length of hospitalization in patients with blunt thoracic trauma. 17 Data continue to support the use of ISS score as a predictor of ICU stay in thoracic trauma patients, as the majority (99.6%) of them have blunt thoracic trauma. Surprisingly, ISS was not a significant factor associated with prolonged ICU stay in the present study, although this could be explained by the fact that most of the thoracic trauma-related deaths occurred within 7 days of injury. The cases identified as ISS ≥16 may have been more likely to die during the first 7 days of ICU care. It is not possible to draw firm conclusions from these data due to limitations in study design (such as the inclusion of only thoracic trauma patients, who were admitted to a single institution) and data collection methodology.
There are several limitations associated with this study: (i) the database consisted of patients with thoracic trauma admitted to the hospital, and was obtained from the Department of Thoracic Surgery, rather than the Emergency Department or the ambulance service; (ii) the outpatients were not included; (iii) patients with cardiac or great vessel trauma were not included in the study; (iv) the retrospective design of the study. The present study, however, provides valuable information on the critical care of thoracic trauma patients that, to the best of our knowledge, was not available in the medical literature. In spite of the limitations posed by the design of this study, this large-scale investigation enabled the identification of important factors that help to predict which patients would require ICU care.
In conclusion, thoracic trauma in Taiwan generally affects male, middle-aged adults. More than one-third of patients require ICU treatment, a quarter of whom are admitted to the ICU for ≥7 days. Head injury and chest tube placement are the most important factors associated with ICU admission of any duration, while head injury and chest drain are the most important predictors of prolonged ICU stay. Overall, associated injury factors play a more prominent role than thoracic factors in the need for ICU and prolonged ICU care. A multidisciplinary trauma team (involving neurosurgeons, abdominal surgeons and orthopaedic surgeons, working together with thoracic surgeons) is essential for the care of patients with traumatic thoracic injury.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.