
Abstract
Introduction
Both in the UK and internationally, discharge from an intensive care unit to home for end of life care is a rare and challenging occurrence. These challenges include clinicians’ ability to identify appropriate patients in whom it is possible to communicate with about their wishes and preferences, the critical nature of their condition and the interface between hospital and community services.
Method
We present a case report of a patient who had been admitted to hospital with a myocardial infarction and subsequently suffered a cardiac arrest, from which he was successfully resuscitated. Subsequently, he suffered multi-organ failure, but despite treatments, the ceiling of care was reached. With a poor prognosis, medical and nursing staff engaged in advance care planning to determine his wishes and preferences at the end of life and to facilitate his discharge from the intensive care unit to his home.
Conclusion
This case study has highlighted that through good communication amongst patients, families and professionals and collaborative working across boundaries and organisations, appropriate patients in the critical care setting can have a real choice regarding where they wish to be cared for and die at the end of their life.
Introduction
The majority of people would prefer to be cared for and die in their usual place of residence; however, hospital remains the most common place of death. 1 Within the critical care environment, patients rarely have the freedom to choose their preferred place of death. Both in the UK and internationally, the discharge of a conscious patient from the intensive care unit (ICU) to home for end of life care (EOLC) is a rare occurrence. 2 Consequently, health-care professionals are unable to develop the skills, knowledge and confidence to identify potentially appropriate patients whose preferred place of death is home and to communicate this possibility with the patient and those important to them. This case study describes the experience of medical and nursing teams in the care of a patient and his family approaching the end of life in a specialist cardiac intensive care unit.
Background
We present the case of a 71-year-old married man with a medical history of coronary artery bypass grafts 20 years ago and chronic kidney disease. He was a farmer and had spent his life in the same house farming his land. Both his sons are farmers, and there are a number of grandchildren who all lived on the farm with him.
The patient was admitted to hospital following a non-ST elevation myocardial infarction. The initial coronary angiogram demonstrated severe three-vessel disease including a 95% stenosis of the right coronary artery (RCA) and occluded bypass grafts. Percutaneous coronary intervention (PCI) to the RCA was considered too high risk, as the lesion was heavily calcified. Shortly afterwards, the patient developed ventricular fibrillation requiring six shocks and cardiopulmonary resuscitation. An emergency high-risk PCI and stent were successfully performed. Following the procedure, the patient was admitted to the ICU and extubated within 12 h; however, he required inotropes, vasoconstrictors and diuretics as his liver, renal and cardiac function remained compromised. His condition improved, and he was discharged to the ward; however, he subsequently required re-admission to the ICU with cardiogenic shock, worsening end-organ dysfunction and sepsis. Once again, following treatment, he made some recovery and was discharged from ICU to the ward only to require further readmission for cardiogenic shock requiring inotropes and continuous renal replacement therapy. On inotropes, his trans-thoracic echo demonstrated severe biventricular dysfunction with severe mitral regurgitation, severe tricuspid regurgitation and moderate aortic regurgitation. Despite optimal treatment, the patient remained in heart failure with an ejection fraction of 11%. Over the following days, he remained stable on inotropic support, but no significant improvement was noted.
A multi-disciplinary meeting was held and agreed that the patient was not suitable for any further escalation of treatment due to his age and severity of end-organ dysfunction. The patient and his family were seen by the cardiologist in charge of his care who discussed his poor response to treatment. It was explained that the maximum ceiling of support had been reached, and the prognosis was poor. The news was devastating for the patient and his wife; however, at this point, he expressed a desire to die at home.
Patient and family perspective
The following morning a nurse taking handover from the night staff noticed the patient was psychologically and emotionally depleted. He disclosed how distressing he had found the news of his poor prognosis and how he felt completely out of control. He dreaded dying in hospital with all the noise from alarms, ward activity, bins banging and being disturbed for nursing interventions; he stated he wanted to be at home, on his farm with his family where he belonged.
The nurse adopted a pro-active approach and ensured that his desire to go home was fully discussed with the medical team on the ICU ward round. The hospital supportive and palliative care team was contacted to enlist their support in meeting his wishes. The patient was already known to the supportive and palliative care team who had been seeing him for management of his symptom of breathlessness and supporting his family. A clinical nurse specialist (CNS) from that team met with the patient and his family and explored their understanding of his situation and his wishes and preferences.
The hospital End of Life Steering group has approved the use of the Principles of Care for Dying Patients document, developed by the London Cancer Alliance. This document embodies the approach in One Chance to Get it Right, 3 drafted by the Leadership Alliance for the Care of the Dying Person in response to the report More Care, Less Pathway, 4 which recommended the phasing out of the Liverpool Care Pathway. The approach is focused around five priorities of care and how these should be applied to ensure high-quality care in the last days or hours of life, and it is these priorities that guided decision making amongst those involved in the discharge.
Although his desire to go home was supported by his family, the patient was dependent on inotropes and renal replacement therapy. He and his family were made aware that he could not be maintained on inotropic support at home, and following cessation of these drugs, deterioration may be rapid. Furthermore, they understood that cessation of the inotropes whilst in hospital, and possible rapid deterioration may result in him becoming too unwell and unstable to transport, or dying during the transfer home; however, the patient still wanted to attempt to get home. A Do Not Attempt Cardiopulmonary Resuscitation Order (DNACPR) was completed that would travel with him in the ambulance.
The ITU perspective
Following discussion between the ICU medical, nursing team and CNS in Supportive and Palliative Care, it was agreed to try to facilitate a rapid discharge in order to meet the patient’s and his family’s wishes. As prognosis was poor and likely to be hours to short days, a rapid discharge within 24 h would be required (Figure 1). The ICU team planned to perform continuous renal replacement therapy overnight prior to discharge to reduce the risk of potential pulmonary oedema during transfer. The patient had received Levosimendan and required low-dose noradrenaline, which would be weaned off throughout the morning of discharge and exchanged for an infusion of dopamine which would run via a newly sited peripheral line, so that the central venous and haemodialysis catheters could be removed. The dopamine would continue until the patient arrived home and then this would be stopped by the ICU nurse escort on arrival at the farm. Although this was a complex discharge, it was considered that a nurse escort, as opposed to a medical escort, would be appropriate considering the context of the patient being discharged for EOLC, having accepted the risk that he may die during transfer and a DNACPR being in place. The medical handover, in the form of a discharge letter to the GP, accompanied the patient. Anticipatory medications were prescribed and ordered from the pharmacy in order to manage common symptoms at the end of life. A temporary community drug chart was completed to enable either the nurse escort or community palliative care nurse to administer the anticipatory medications en-route or in the home until the GP visited and completed the usual chart used by community nursing staff. Hospital senior management gave permission for the nurse escort to carry out interventions such as drug administration outside of the hospital setting. The patient and family were made aware that they could contact the ICU at any time for advice and at lunchtime on Friday an emotional farewell took place on leaving the unit for his final journey home.
Timeline of discharge.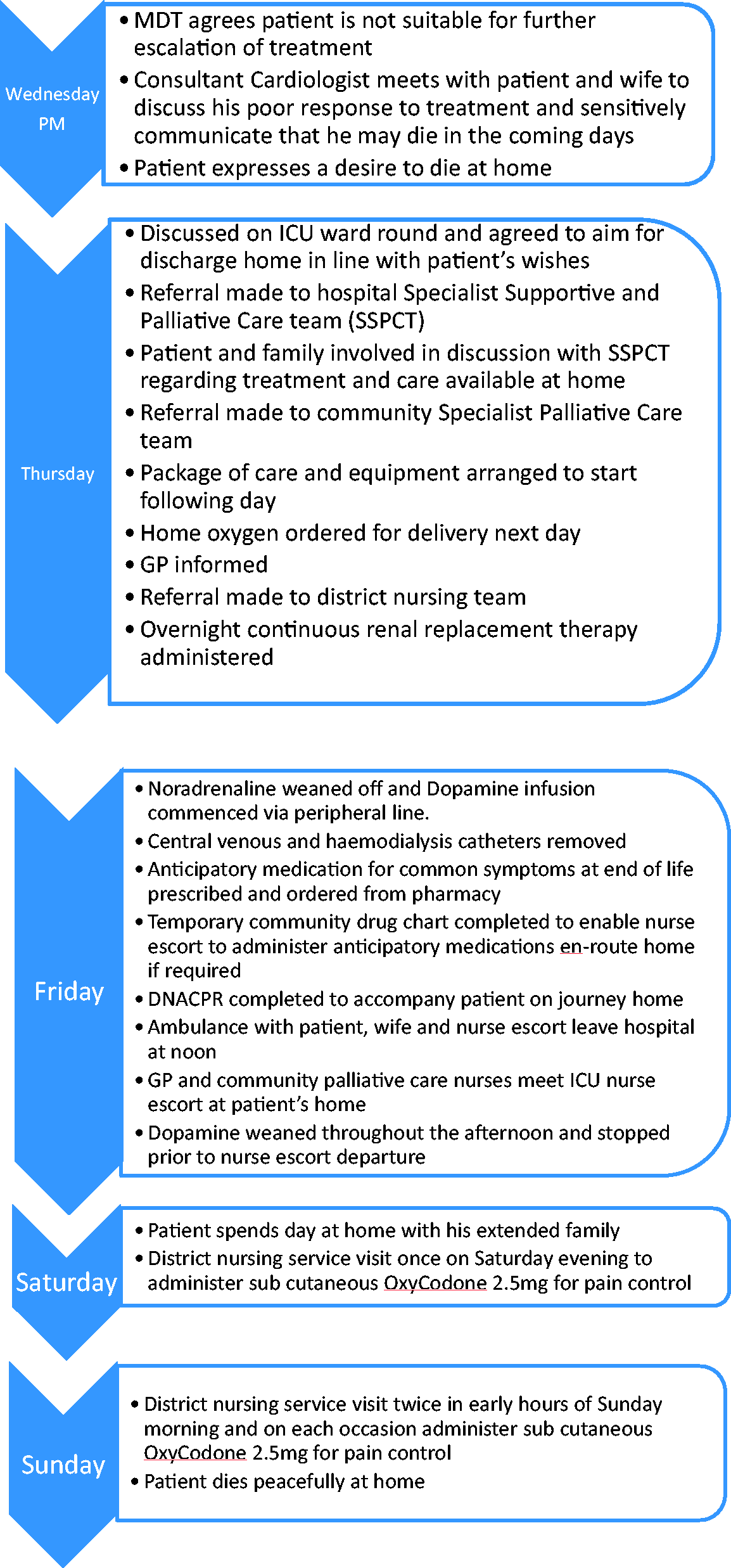
Liaison with community services
The hospital supportive and palliative care CNS contacted the community specialist palliative care team in the area in which the patient lived. Specialist palliative care services in the community help to manage complex patient care issues above that which generalist community services such as the GP and district nurse can provide. The responsiveness of the community palliative care service in this patient’s area contributed significantly to being able to get him home as quickly as was achieved. Following referral to their service, they sourced a package of care with visits from carers three times a day to meet his personal needs. They also ordered equipment that would be required including a hospital bed, pressure-relieving mattress, slide sheet and commode, to be delivered on the morning of discharge. They also arranged for a CNS from their team to be present at the home to receive a handover of care from the ICU nurse escort.
The hospital supportive and palliative care CNS ordered oxygen, and this was delivered to the home the evening prior to discharge. The patients GP was contacted and updated on the patient’s recent admission and the plan for discharge. It was agreed that the GP would refer the patient to the district nursing service and that he would visit the patient on the afternoon of discharge. GPs are in overall charge of the patient’s care in the community. An important aspect of the district nursing role is to enable patients to die peacefully at home. Following referral, they will carry out a full assessment of a patient’s needs and provide nursing care. This includes the administration of subcutaneous medication for symptom control and the setting up and management of syringe drivers.
The community perspective
Just after lunchtime on Friday afternoon, the patient arrived home and the ICU nurse escort was met by a community palliative care CNS and a nurse from the Hospice at Home team, with the arrival of the GP 20–30 min later. It is good practice for a GP to visit a dying patient to aid clinical management and for administrative requirements relating to death certification following death. Having been seen by the GP, the community palliative care nurse was able to verify death, which can help to prevent the need for a lengthy wait for a GP to attend particularly if the death is out of hours. The GP and community palliative care team were grateful that the patient was sent home with the anticipatory drugs (i.e. home oxygen, midazolam, oxycodone, metoclopramide and glycopyrrolate), particularly as the discharge was on a Friday afternoon. Obtaining controlled drugs may have been challenging and may possibly not have arrived in time for when needed. After handing over to the community palliative care nurses and GP, the nurse escort began weaning the dopamine infusion by 15 µg every 15 min. The dopamine was stopped, and once the nurse escort felt that things were settled in the home, she returned back to the hospital in the early evening.
The family reported that following discharge the patient was able to eat and drink his favourite food, spend time with his grandchildren and watch old family cine films. His daughter-in-law performed leg massages and he found comfort in seeing the Vicar. He required one visit from the district nursing service on Saturday evening and two visits in the early hours of Sunday morning for administration of stat doses of subcutaneous opioids to control his pain. The Hospice at home team was en-route to visit him the next morning, with a view to commencing a continuous subcutaneous infusion for analgesia but he had died peacefully by the time they arrived. He died with his wife and sons by his side, looking out of the window at the farm he loved.
His family later contacted the intensivist in charge of his care on the day of discharge and expressed the gratitude they felt for the short time that they had him at home and the precious memories this had left them with.
Their hope is that other families will have the same opportunity to bring their loved ones into the home environment when prognosis is poor.
Conclusion
Discharging conscious patients home to die from the ICU is a rare occurrence. Whilst many patients in the critical care setting may not be suitable for transfer, this case study demonstrates that certain patients may have a preference, and be appropriate, to transfer home to die. This can be achieved through good communication amongst patients, families and professionals and collaborative working across boundaries and organisations. Whilst patient preference was the driver in this particular case, it is hoped that the example described here will help multi-disciplinary teams to identify whether some patients can be discharged home for their EOLC.
Footnotes
Consent
Published with the consent of the patient's next of kin.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.