
Abstract
NHS England is to introduce a new Commissioning for Quality and Innovation to reduce delayed discharges from adult critical care to ward-level care. A delayed discharge is greater than 4 h, this occurred in 64.2% of patients in the critical care minimum data set database from Intensive Care National Audit & Research Centre from the last five years; 46.3% were delayed between 4 and 24 h and 17.9% were delayed more than 24 h. For those who had a delay in their discharge of greater than 24 h, the data suggests that “sicker” patients ultimately do better, since there was a reduction in expected mortality of 5892 patients to an actual mortality of 5201 patients over the five years. More in depth analysis of this data is necessary to try to identify which patients are more likely to benefit from extending their critical care stay once the need for organ support has abated. The current Commissioning for Quality and Innovation offers a slightly perverse incentive against this cohort of patients.
Critical care delayed discharge: Good or bad?
The Intensive Care National Audit & Research Centre (ICNARC) have been measuring delayed discharge in adult, general critical care units in England, Wales and Northern Ireland participating in the Case Mix Programme for many years. The critical care minimum data set (CCMDS) definition they use is
The patient has been declared clinically ready for discharge or transfer and a formal request has been made to the hospital bed management system, and the date and time of this status is recorded as such in the clinical record.
The aim of the CQUIN is to reduce delayed discharges from adult critical care to ward level care in the same hospital by improving bed management in ward based care, thus removing delays and improving flow. Discharges occurring directly to home will also be included as these are a reflection of a delay in discharge to a ward.
NHS England does recommend that the CQUIN scheme should be complemented by monitoring of (i) cancelled high risk elective operations, (ii) night time discharges from Critical Care, as these tend to be symptoms of a failure to discharge timeously. Success in timely discharge should be associated with reduced problems in these dimensions. Critical Care ODNs (Operational Delivery Networks) should monitor these outcomes.
A 2013 paper by Garland and Connors 3 looked at mortality rates and delay in discharges in 2401 survivors in their 13-bed medical intensive care unit in Canada. They found the lowest mortality with a 20-h delay in discharge (odds ratio of death 0.35 compared with no delay). Even with a 72-h delay in discharge, mortality was still reduced (OR 0.93).
I therefore put in a freedom of information (FOI) request to ICNARC asking for the percent hospital mortality post-critical care discharge over the last five years of validated data from the national case mix programme database subdivided into no delay, 0–4 h; a delay of 4–24 h and >24 h delay. Soon after the request, I had a telephone conversation with Professor Kathy Rowan and discovered that ICNARC are not bound by the FOI act; however, she kindly agreed to accede to my request including both adjusted and unadjusted mortality for the time periods.
The results are exactly as supplied by ICNARC with the following acknowledgement These data derive from the Case Mix Programme Database. The Case Mix Programme is the national, comparative audit of patient outcomes from adult critical care coordinated by the Intensive Care National Audit & Research Centre (ICNARC). For more information on the representativeness and quality of these data, please contact ICNARC. Flow of included admissions.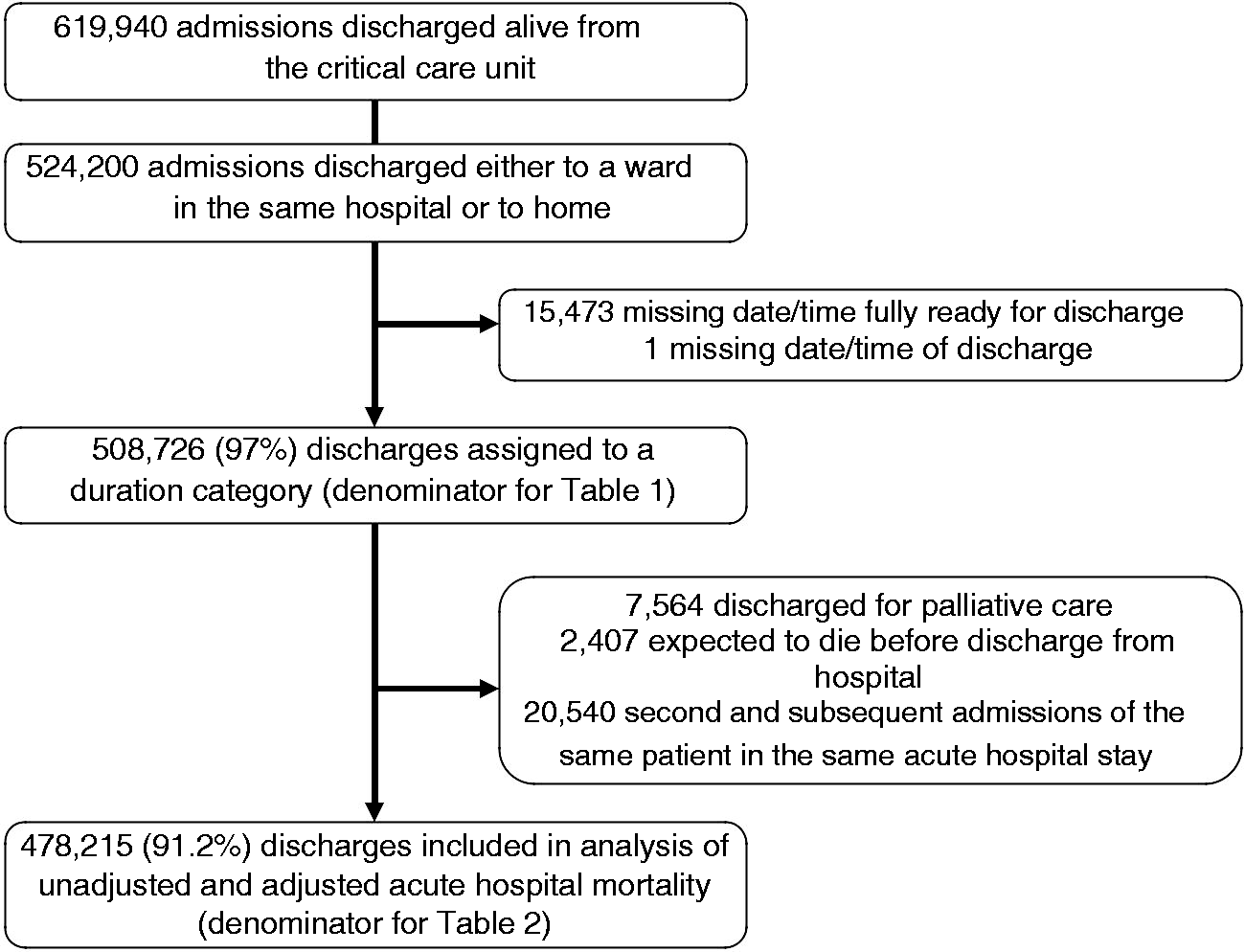
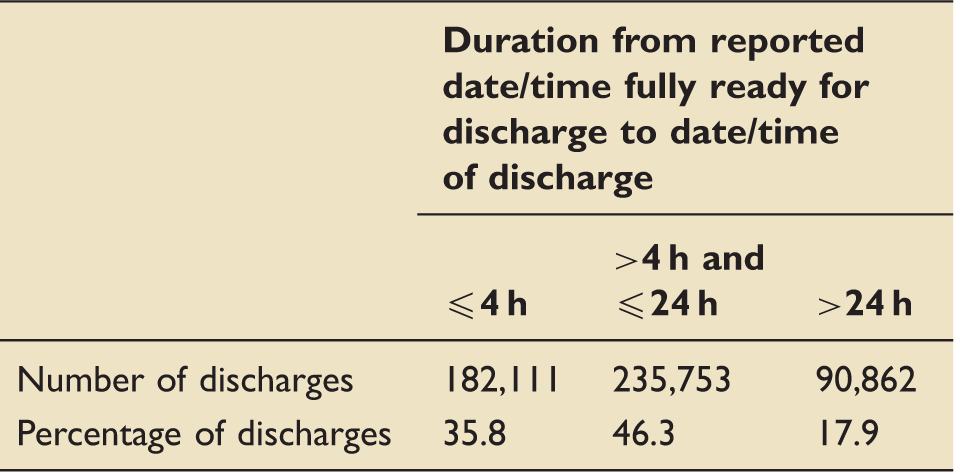
Number and percentage of discharges by duration from reported date/time fully ready for discharge to date/time of discharge (duration category).
Unadjusted and adjusted acute hospital mortality by duration from reported date/time fully ready for discharge to date/time of discharge (duration category).
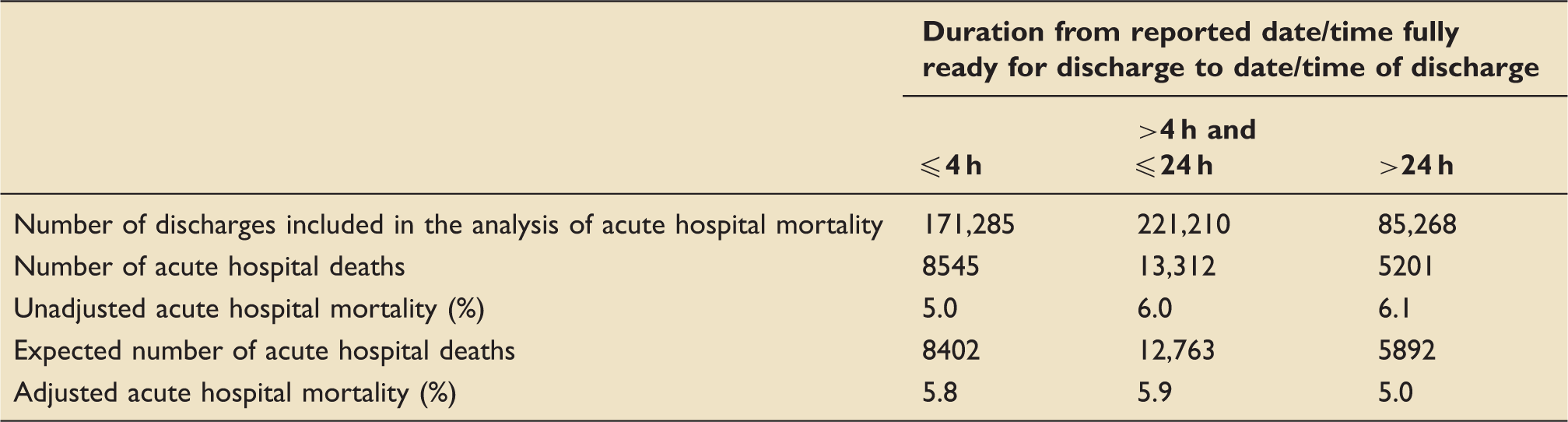
This national critical care data from the last five years demonstrate that the majority of patients, 64.2%, had a delayed discharge greater than 4 h. More importantly, it suggests that “sicker” patients ultimately do better if they have a delay in their discharge of greater than 24 h, with a reduction in expected mortality of 5892 patients to an actual mortality of 5201 patients. For our complex patients at East Lancashire Hospitals NHS Trust, with a length of stay greater than one month, we already implement a planned discharge to ensure that their ongoing care can be provided on the ward. This can take a number of days and usually starts at the weekly MDT meeting, ward nursing staff are invited to critical care to familiarise themselves with the patient prior to discharge, and we offer post-discharge support.
These data suggest that perhaps we should adopt this approach for more patients; however, further analysis would be helpful to determine who would benefit most. Further analysis could include more time subdivisions of the 90,862 (17.2%) patients delayed greater than 24 h, as well as investigating if there is any correlation between length of stay or number of organs supported and benefit from a delayed discharge. Also we already know that overnight discharges have a worse outcome, therefore a more detailed analysis of time of day of discharge and whether there is a relationship with delayed discharge and outcome is appropriate. Subsequent communication with ICNARC has indicated that it is their intention to explore delayed discharge in more depth.
It appears that for optimum outcomes, the sickest patients should have a “delay” in critical care discharge so that they stay at least a day longer than we presently intend them to. As it currently stands, the CQUIN provides a slightly perverse incentive not to do this. Perhaps, a more difficult to measure, but ultimately more useful critical care CQUIN, would be one that linked delays both in admission and discharge. Good practice would be indicated by no delayed admissions despite selected patients remaining in critical care after their need for organ support has abated. The target would thus be more likely to reward higher quality critical care discharge decision making rather than just being a proxy for flow through the wider hospital.
Footnotes
Addendum 27/10/2016
The latest news from our ODN via an email from Donald Franklin who is Head of Commissioning Incentives Policy at NHS England Specialised Commissioning Commercial Directorate is that the TR1 Adult Critical Care timely discharge CQUIN is not being introduced into next year's contracts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.