
Abstract
Around 13% of patients admitted to critical care in Europe die in the Intensive Care Unit (ICU). In the United Kingdom, 15%–20% of patients admitted to critical care do not survive to discharge. Of those that die in ICU, 80% do so following an active decision to withdraw life-sustaining therapy (WLST). With the increasingly aged and co-morbid critical care population entering the ICU, there is an ongoing need for timely, considered discussions both when initiating life sustaining therapies, and also for effective, sensitive communication and management when it comes to withdrawing. In the case of WLST, very little data exists reflecting the proportion of scenarios involving an ‘awake’ patient with capacity to take part in this decision. It is, however, generally thought to be a small proportion. Most intensivists will therefore have less experience in this process, which perhaps is more representative of the work of our palliative care colleagues. We aim to discuss the most common scenarios in which WLST may occur in the awake and capacitous patient in critical care, the challenges to providing this, and some practical advice on how to perform it well, including the benefits of early interdisciplinary collaboration alongside palliative care.
Deciding when it is appropriate to withdraw life sustaining therapies
The starting point for reaching appropriate decisions is a careful and multi-faceted approach to the clinical situation, including assessment of prognosis and benefit/burden of treatments, which may necessitate a second specialist opinion where uncertainty exists. The General Medical Council (GMC) has clear guidance for professionals around treatments which have the potential to prolong life, and when to consider discontinuation or withdrawal of these treatments. 1 Treatment options must be clearly discussed and communicated with appropriate language to patients and their loved ones and should include goals of care, benefits, burdens and risks. 1
It is acknowledged that patients, their loved ones, and staff may find it more difficult to contemplate withdrawal of a life-prolonging treatment than not deciding to start it in the first place. 1 At times there can be feelings of guilt and emotional distress associated with these decisions, especially if felt that the decision directly results in the patient’s death. However, it is imperative that healthcare professionals guide and reassure members (and staff) throughout this process that this is not the case, while retaining sound professional judgement to ensure that treatments are not continued which are of no overall benefit to the patient. This is where interdisciplinary collaboration between ICU and palliative colleagues is of benefit. 2
Where disagreements exist, either between patient, families, or within healthcare teams, these can generally be resolved by involvement of senior colleagues, requesting second opinions or independent advocates. It is always important to explore the reasons for disagreement. If the disagreement is connected to a religious belief, it may be helpful to seek support from the chaplaincy service, who may be able to act as an independent mediator to help the family understand, come to terms with and accept a best interests decision. 3 Case conferences or mediation services may be needed, and every conversation should be clearly documented in the medical records. Where there is ongoing dispute, formal procedures may need to be considered including legal advice.
Challenges of WLST in awake patients in critical care
Familiarity
Management of dying patients is something that intensivists are relatively experienced in, although there remain challenges in providing a death free from pain, distress, and anxiety in the critical care environment. Although critical care units have a similar proportion of deaths compared to hospices, patients in critical care are often younger and the deterioration more likely to be unexpected. 4 In many circumstances, the patient lacks capacity or consciousness due to either the nature of their acute illness or pharmacological sedation to facilitate treatments. Intensivists may therefore be less familiar with removal of WLST in the ‘awake’ patient. There can be significant ethical uncertainty surrounding the withholding of therapies versus their active withdrawal.5,6 Speaking to patients and families about deterioration, dying, ascertaining priorities and ‘what matters?’ 7 to guide management in the terminal phase of illness is a core component of the approach used by specialist palliative care teams. Hence this is an area where combining the skills and experience of both critical and palliative care is beneficial.
Conversations around care
Much of the current focus in critical care is centred on treatment escalation planning, tailored to each individual patient’s wishes and needs so that certain therapies are not started at all. However, due to the time-pressured nature of critical illness, lack of information at time of referral, and potential for diagnostic uncertainty in this cohort, this escalation planning is not always immediately possible. In many circumstances, timely and supported conversations about disease trajectories, risk versus benefits of starting and the reality that at some stage, life sustaining treatments may be discontinued do not happen before treatments commence. This may put intensivists more often in the circumstances of withdrawing as opposed to withholding therapies, which they are known to be far less comfortable with. This challenge is further enhanced by the relative ‘ease’ of starting some more invasive therapies in the critical care unit in comparison to other areas of the hospital. High flow nasal oxygen, for example, is seen as a relatively low burden intervention with good maintenance of patient comfort, and easily be started on patients with respiratory failure. 8 Its planned removal, however, can prove far more challenging. The transition in care from a period of active intervention with curative intent to planned removal of this can be fraught with misunderstanding, moral distress and potential conflict amongst the multi-disciplinary team, patient, and their loved ones. These scenarios are a particular source of distress for intensive care physicians. 9 Involving palliative care colleagues from the outset in this process can provide support for patients and families as well as professional support for critical care team members.
Confusion with euthanasia or assisted dying
Some patients and their loved ones may fear that WLST is akin to a form of euthanasia or assisted suicide. It is therefore important that the communication process around WLST addresses this potential concern among patients, their loved ones, and healthcare professionals involved. WLST is ethically, legally and clinically a distinct entity, which focuses on the benefit versus burden of medical treatments. Discussions about WLST, when undertaken sensitively and in a structured manner, can be an empowering conversation for patients and their next of kin, who may feel they have otherwise ‘lost control’ of their situation and decisions relating to care. This is furthermore an area which palliative care specialists are well versed at discussing with patients. Palliative care specialists can provide reassurance and assist critical care teams with education/briefing/debriefs from an objective perspective if required.
Environment
The critical care setting is a medicalised, bright and noisy environment. Continued monitoring and noisy alarms are common. For this and other reasons, some patients may not wish to die in hospital. However, hospice beds are not always available and only 6% of intensive care patients are directly transferred home 10 for end of life care. Transferring someone home for EOLC from the ICU is inherently complex and time consuming. Traditionally, this was only possible for longer term critical care patients with a very clear expected trajectory of death after cessation of therapy.
Health boards are now aiming for more equitable access for patients and families to specialist palliative care in community settings, 11 so more commonly complex discharges can now be made from ICU departments to home at shorter notice. Virtual ward services including ‘virtual hospice beds’ are increasingly commonplace and involve the provision of intensive hospital or hospice- level support for patients wishing to return home to die.12,13 The logistics require significant advanced planning and fastidious handover between hospital and community teams, and this transition is greatly eased with the involvement of palliative care colleagues from an early stage.
Challenging symptoms
Withdrawal of life sustaining treatment in awake patients may exacerbate symptoms such as anxiety, breathlessness, agitation and delirium. All of these can be potentiated by psychological distress. In the critical care setting, intensivists are more likely to use the intravenous route for administration of medications, mostly commonly morphine and midazolam 14 to manage symptoms. Risks of failureof venous access and the burden of maintaining the intravenous routes mean that symptomatic relief for WLST in awake patients often favours the use of subcutaneous medications. 15 Administration of medicines via this route may be less familiar in critical care. Timely collaboration with palliative care can make planned transitions from IV to subcutaneous routes more seamless, especially where patients are transferred to downstream wards or planned for home. If WLST is to happen within the ICU, IV or subcutaneous routes can be used, and this should be considered as part of the planning for each individual. If symptoms escalate, including agitation, delirium or distress, there may be the necessity to use additional medications to manage symptoms including levomepromazine or phenobarbital (Table 2).
Communication
Communicating effectively the intricacies of WLST treatment decisions to patients and families (as well as healthcare professionals involved) is of critical importance.
Value based medicine (VBM) is a concept which is advocated, but not necessarily achieved routinely in medical practice. VBM is a development of evidence-based medicine and can be described as: ‘the practice of medicine incorporating the highest level of evidence-based data with the patient-perceived value conferred by healthcare interventions for the resources expended’,13,16 This approach aligns with the concept of realistic medicine 17 which aims (among other tenets) to encourage shared decision making, promote a personalised approach to care, a move away from ‘Dr knows best’ to reduce waste/harms and inefficiency while continuing to deliver excellent care. The definition/principles of VBM and Realistic Medicine are to ensure that medical treatments being delivered to patients are not only appropriate and patients are fully informed, but that treatments are also aligned with the patient’s goals of care. 18 Goals of care are individual to patients and may not always be aligned with clinical guidelines. It is therefore incumbent that we, as clinicians ask patients what their goals are and what mattes to them.
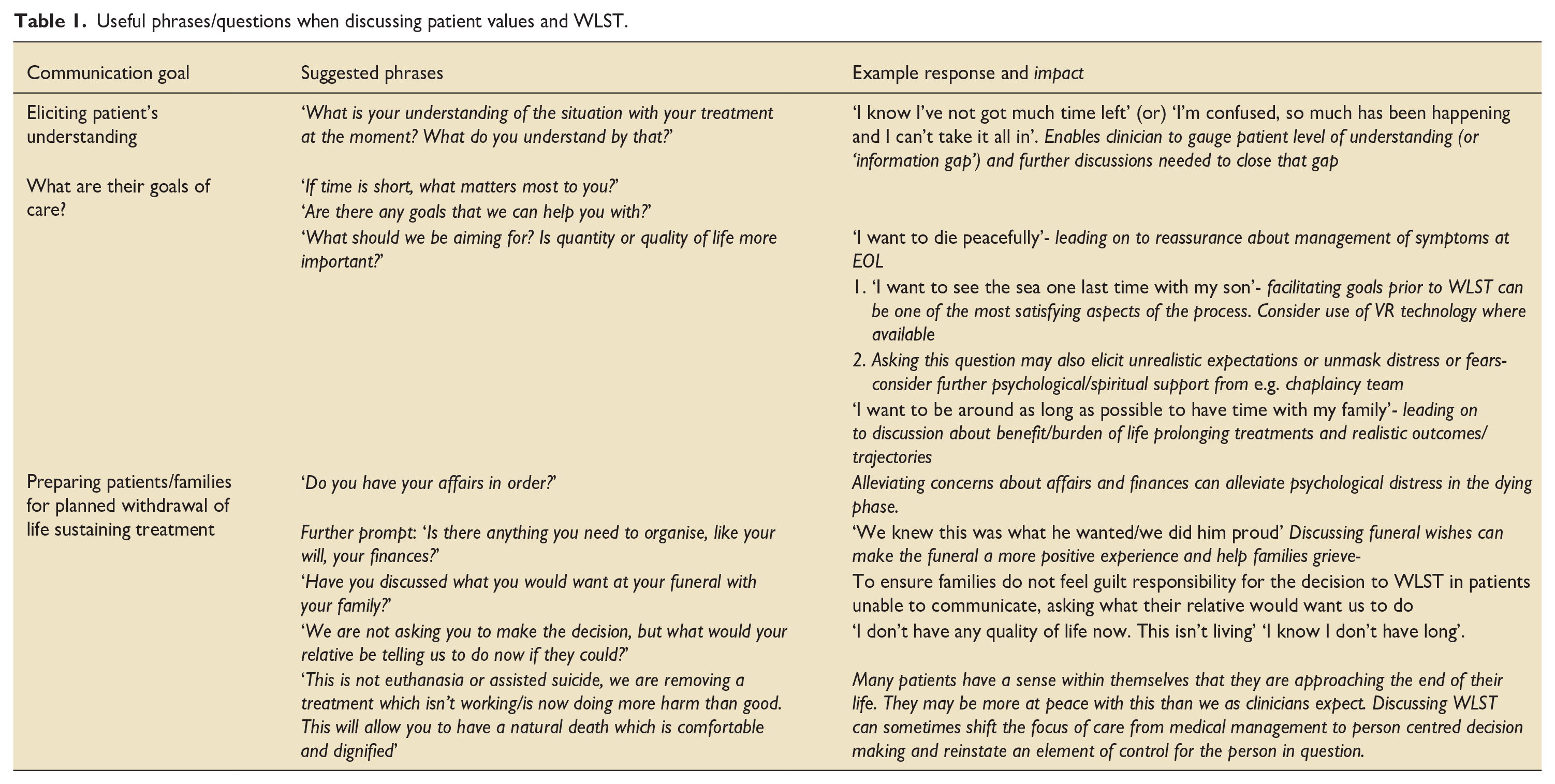
Conversations with patients and their loved ones around continuing or discontinuing life sustaining treatment should not only include risks/burdens versus benefits of treatments but must also include eliciting goals of care. Table 1 contains suggestions for questions or phrases which may be useful when holding discussions with patients and their families around WLST in the ICU setting. These phrases and the routine use of a VBM and Realistic Medicine approach should be encouraged through all healthcare settings.
Useful phrases/questions when discussing patient values and WLST.
Withdrawal of life sustaining treatment: Getting it right in critical care
The panoply of basic and advanced organ support a patient may be given in critical care dictates that there is a multitude of scenarios in which an awake patient may have these supports removed. There is therefore no single accepted strategy for doing this. It may involve agreement of limitations of current supports (e.g. noradrenaline infusion), withholding of future interventions, or withdrawal of some or all of current life sustaining therapies.
The removal of respiratory support in an awake patient may include non-invasive ventilation via CPAP, BiPAP or high flow nasal oxygen. This generally tends to be done after a patient is given some form of pharmacological symptom management to reduce feelings of anxiety and breathlessness, titrated to effect. The outcome is generally death within a period of minutes-to-hours, although planning for and acknowledging uncertainty in this is also important.
Discontinuation of sole renal replacement therapy is less common than the decision to withhold it as a therapy in critical care. A decision to stop it may involve removal of invasive lines and potential transfer of the patient to a preferred location in the hospital. If this is the only organ support removed, it tends to confer a low risk of physical distress and a period of days until death.
The removal of vasopressors or inotropes equally tends to result in a low risk of distress for the patient. Death may occur quickly if the patient has required particularly high doses. These infusions can be weaned, however this is likely to result in a prolongation of the dying process, especially if only low doses were required. 19
Significant and conscious effort should be put in place to humanise this process as much as possible. Removing all unnecessary equipment, noise, and healthcare workers from the patient’s bedspace is advised, and the possibility of transfer to a safe outdoor space (such as a hospital garden or roof terrace) prior to withdrawal of life sustaining therapy should be discussed. 20
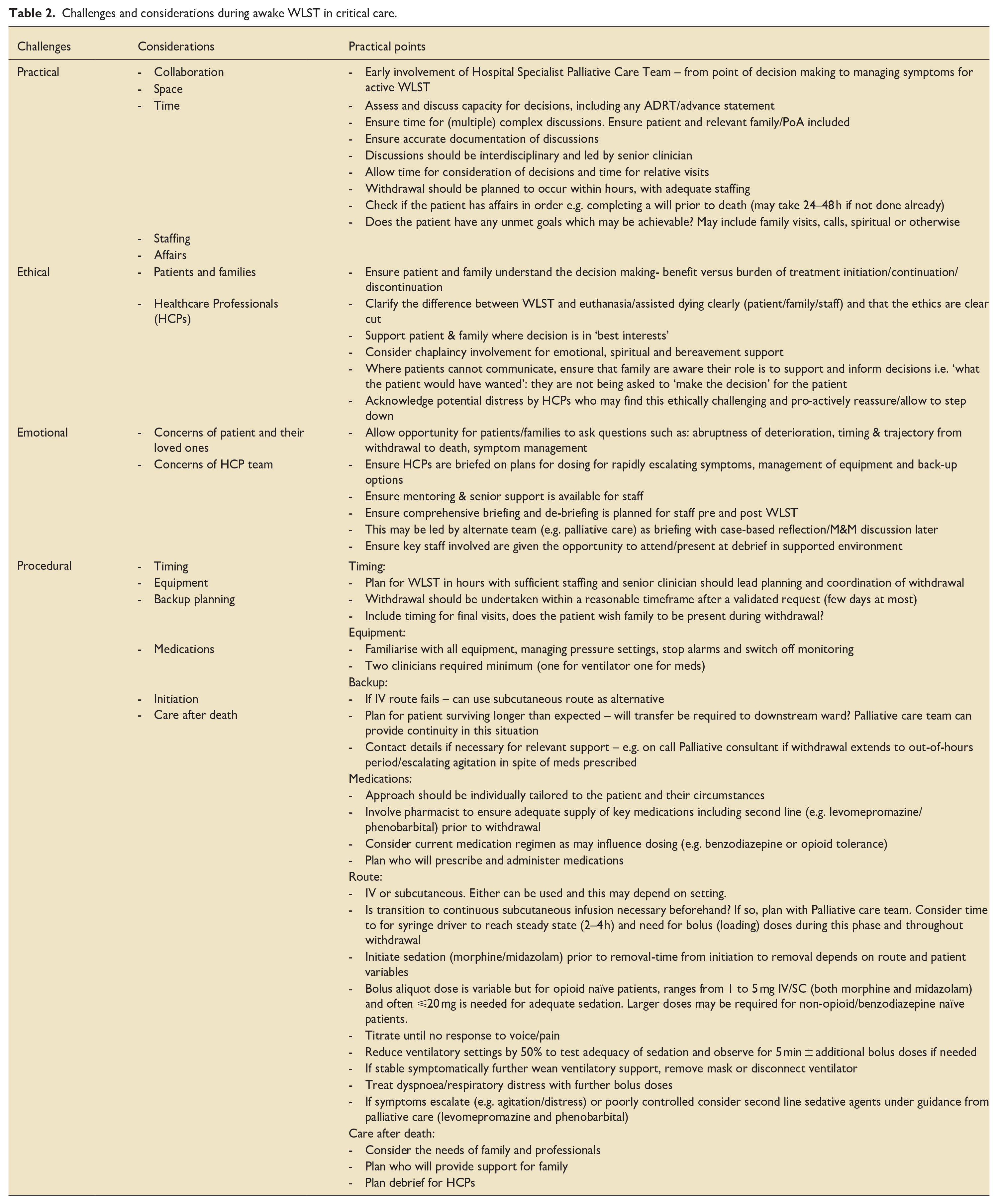
Table 2 Summarises recommendations to guide withdrawal of assisted ventilation in awake patients in both hospital and community settings (adapted from Association of Palliative Medicine (APM) and Specialist Palliative care Audit and Guidelines Group SPAGG guidelines and regional clinical experience).3,5
Challenges and considerations during awake WLST in critical care.
Case example
A 61 year old woman with a background of idiopathic interstitial pneumonia was admitted to ICU with bilateral (covid) pneumonitis and superadded bacterial pneumonia. She had been assessed and was awaiting a decision regarding suitability for lung transplant and was deteriorating in spite of maximal therapy. Treatment included IV antibiotics, and high flow nasal oxygen (HFNO) on maximum PEEP settings. She was alert, oriented and extremely short of breath on removal of oxygen treatment for minutes. She had one sister who was her named next of kin and lived 7 hours away. The ICU team referred the patient to the Hospital Palliative Care Team to help manage symptoms of dyspnoea and for assistance with anticipatory care planning. The patient was seen and initially started on low dose oral morphine and sublingual benzodiazepines with good benefit.
[
Discussions were held jointly by the ICU and Palliative care Consultants with the patient around ongoing deterioration in spite of maximal treatment, with worsening symptoms and the potential for withdrawal of life sustaining treatment. The patient was fully aware that she was sick enough to die and when asked ‘what matters most’ she wished to know the outcome of the decision around the lung transplant and to see her sister. The patient had no will in place and wished for her sister to inherit her estate. When asked what she was most fearful of it was not death itself, but the mode of dying that is, a ‘difficult’ death with symptoms of breathlessness/choking. Dying at home was not a preferred option for this patient but had it been, this could have been explored by the Hospital Palliative care team linking in with the local ‘Virtual Beds’ hospice at home team.
[
With further discussion the decision that lung transplant was not an option was delivered sensitively to the patient, which gave closure. A local solicitor’s firm was contacted and the palliative care team facilitated (using video calls and email) the completion of the patient’s last will and testament- which took >24 h. The patient’s sister visited and the patient was clear that they did not wish her to be present when she died. Staff were briefed and medications/lines checked as well as back-up options including second line subcutaneous medications and how a potential move to a downstream ward would be facilitated. Time for questions was given to whole team. IV medications were initiated by experienced ICU nurses at 11:00am with the Palliative care and ICU consultants’ guidance. Once the patient was comfortably sedated, a reduction and removal of ventilation occurred. Medication was given as needed and the patient died peacefully at 14:10 h.
Nursing perspective
The role of intensive care nurses involves regular experiences of patient death. As a result, nurses tend to feel fairly comfortable supporting families through the process of WLST. However, speaking directly to the patient themselves may remain an unfamiliar scenario.
While this situation provides a privileged role for the nurse, it requires development of specific skills. Development of communication skills and continuity to build trusting relationships with patients and their families are two factors that have been identified as challenges in this scenario. 21 The Scottish Government promoted the RED MAP Framework as a nursing resource to overcome communication challenges to empower nurses with these discussions. 22
These discussions involve multiple requirements for the patient’s nursing team. Firstly, a nurse is a vital advocate for their patients. They will respect and represent the patient to the degree to which they wish to be involved in their care discussions. 23 Secondly, a nurse will act as a vital bridge between patient and medical staff. The continuity of contact helps to build a rapport and detailed knowledge of a patient which can be invaluable with end-of-life discussions. 24 It is often routine tasks such as bed bathing or administering IV antibiotics that facilitate moments of connection with patients to allow personal and emotional conversations to occur.
In relation to the scenario described above, vital nursing communications revealed that the patient was not afraid to die. They highlighted her priorities were that all avenues of clinical treatment had been exhausted, that she would be able to see her sister before she died, and that she completed a will. As a result, a strong MDT collaboration enacted these priorities which alleviated her fears and allowed her a peaceful and comfortable death.
The support provided by the Palliative care team in this scenario gave assurance to the nursing staff that aspects of management unfamiliar to them (such as subcutaneous dosing) were correct and beneficial to the patient.
The ability to provide a peaceful and comfortable death in such a circumstance gave the nursing team a strong sense of pride in their work. The calm structure and tailoring of this period to the patient’s priorities and fears allowed a challenging situation to become a source of achievement for the team. This was further affirmed as it was achieved in the fast-paced critical care environment, where awake WLST remains relatively infrequent.
Benefits of collaboration between critical care and palliative care teams
A common misconception among patients and healthcare professionals is that Palliative care pertains only to care of the dying. This stigma or misperception (both among healthcare professionals and patients) can adversely impact timely referrals to Palliative services, where earlier input may have been valuable. Palliative Medicine comprises a spectrum of treatment from supportive (patients undergoing active treatment) to end of life care for any life limiting disease. Palliative care is now advocated alongside routine oncology care by the American Society of Clinical Oncology (ASCO) from the point of diagnosis. 25 Multiple randomised trials have shown benefits including improved quality of life, symptom management, reductions in anxiety/depression and caregiver distress, and less aggressive management at end of life. Furthermore, there are studies which show a survival advantage of palliative care alongside concurrent oncology treatment. 26
There is a growing evidence base for the benefits of collaboration between palliative and critical care. This includes potential benefits for critical care staff as well as cost benefits. 27 A study by Poi et al. 28 examined ICU clinicians’ perceptions on how the integration of palliative care into the ICU affects interprofessional collaborative practices in care of critically ill, and how team dynamics evolved with a collaboration incorporating palliative care practice. Results from this study are summarised in Figure 1.
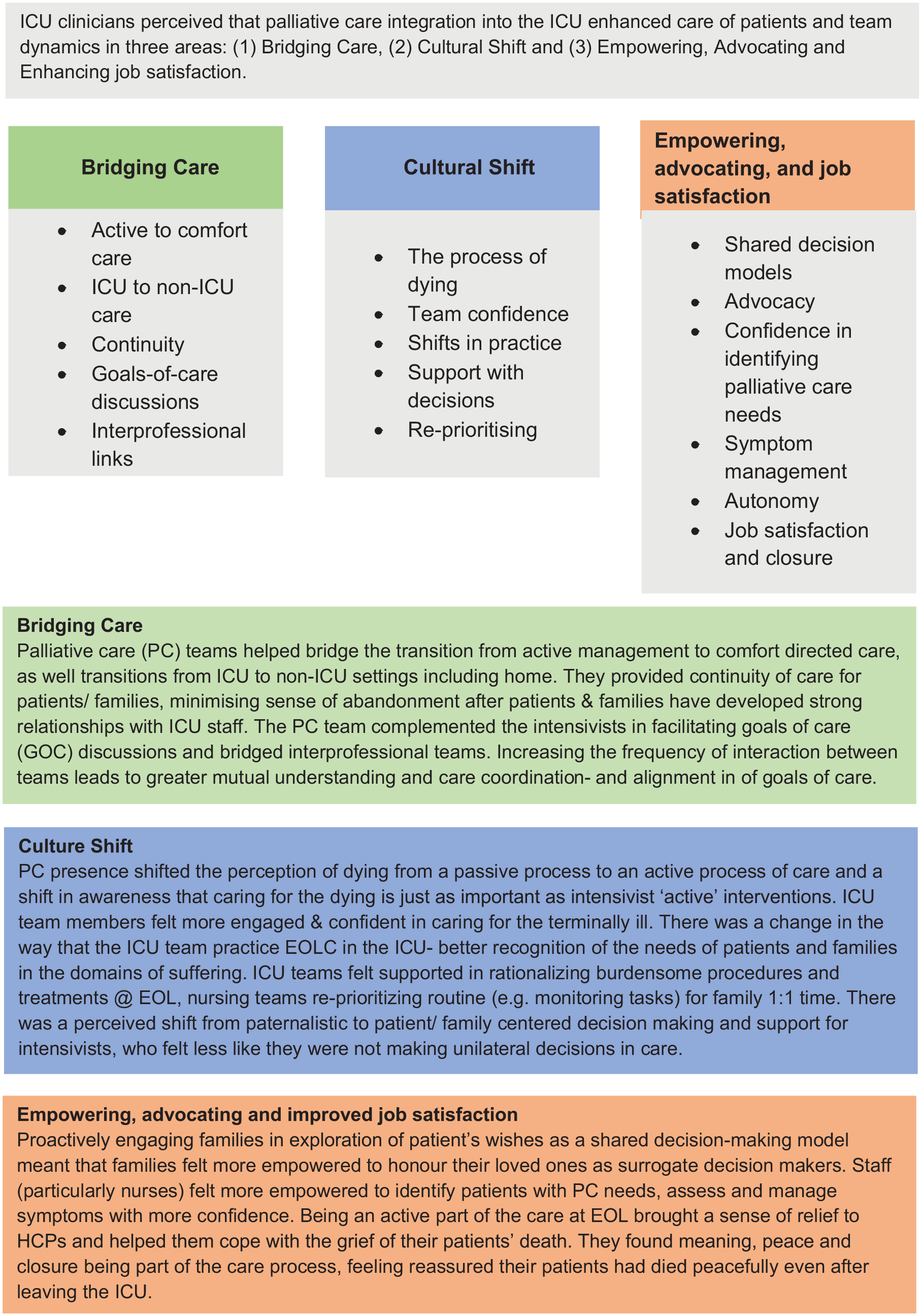
Benefits of collaboration between ICU and Palliative care as perceived by ICU staff (from Poi et al. 28 ).
In our experience, there are numerous potential benefits of interdisciplinary working between Palliative Care and ICU to improve outcomes for patients, families and staff. Not only in cases similar to that outlined in this paper but in many situations within critical care. Through ICU and palliative care teams working together we have noted that although our skillsets are different, there are also many similarities in what we do, and yet our approaches complement each other, resulting in positive outcomes (Figure 2).
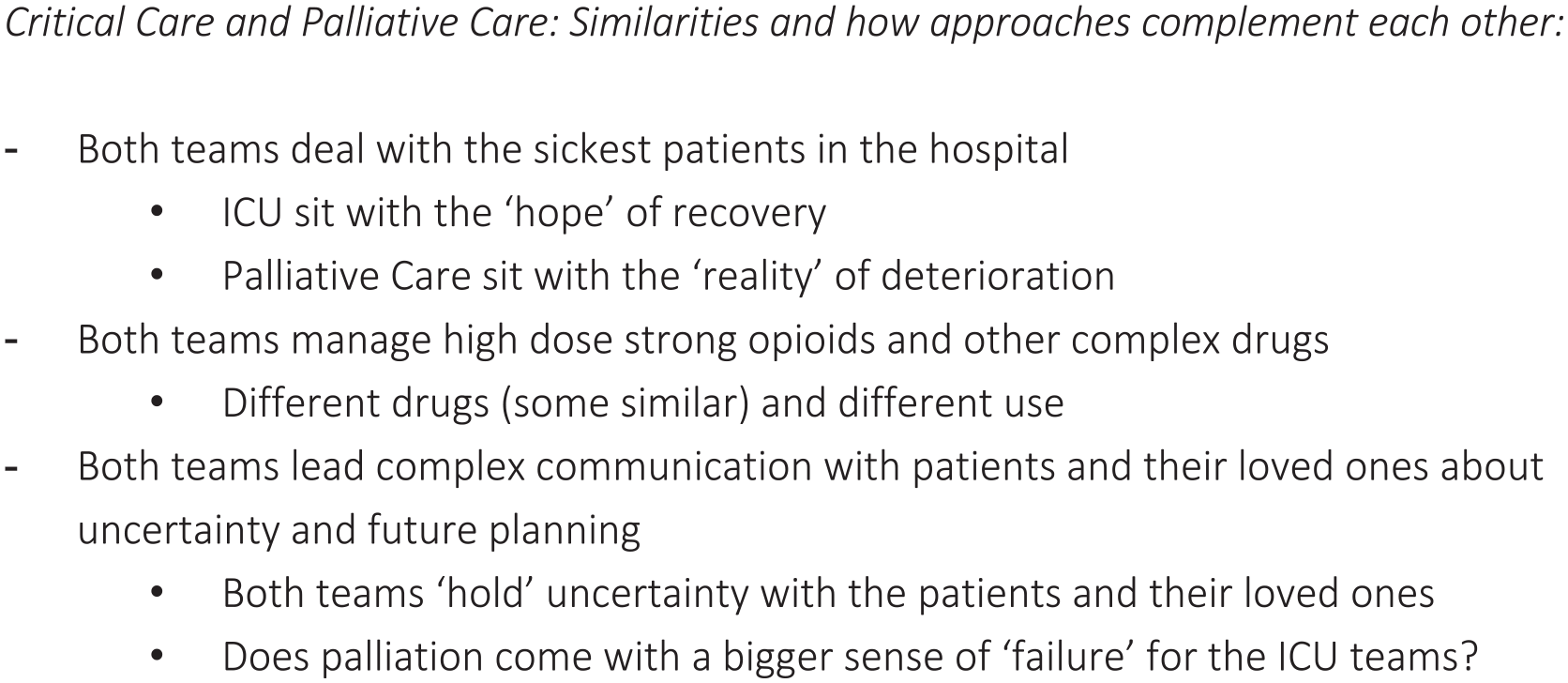
Comparison between critical care and palliative care approach.
Conclusions
In summary, WLST in awake patients can be challenging for both patients, families and healthcare professionals. It presents a unique situation for professionals, whereby treatment decisions are being made in tandem with a patient who may have full capacity and be able to look you in the eye and tell you their fears and hopes, and yet may be dead within minutes to hours of their treatment being withdrawn.
This brings with it the need for clarity among healthcare professionals on the ethical and legal basis and decision making around withdrawal of life sustaining treatments, and the ability to communicate this effectively with patients, families and their own teams who are involved in the process.
The process is far from a ‘one step fits all’ protocolised procedure, and must be individually tailored to the patient, their situation, the setting, with complex planning, coordination and back-up planning considered. A collaborative and shared decision-making model between Intensivists and palliative care clinicians is recommended to allow for a supported, holistic and comprehensive approach.
Neglecting to undertake this process and getting it wrong can have a massive knock-on impact on their loved ones who live on and can contribute to substantial, profoundly negative repercussions. 29 There are also risks to our teams if these scenarios do not run smoothly, potentially contributing to burnout among healthcare providers. There are numerous mutual benefits of ICU and Palliative Care teams collaborating, in WLST and many other scenarios. Navigating the pitfalls and getting this last phase of care right for our patients should be just as highly prioritised as the need to administer life-saving treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.