
Abstract
Background
Globally, ultrasound is being used to assist in central venous and difficult peripheral intravenous access in a variety of emergency and non-emergency clinical settings.
Context
After reading Flood’s paper on safe central venous access and noting the difficulties clinicians find in probe stabilisation whilst performing dynamic intravenous access, we decided to share our teaching technique.
Innovation
The purpose of this correspondence is to highlight the ‘afternoon tea technique’ as a potential teaching method for probe stabilisation.
Implications
It is hoped that this technique will improve the image quality in dynamic procedures and increase the success rate of ultrasound-guided intravenous access in clinical practice.
After reading Flood’s editorial 1 on ‘Central venous catheters (CVC) – staying safe at the sharp end’ with great interest and appreciating the rise of ‘Point of Care Ultrasound’ (POCUS) in intensive care medicine, we wish to share our teaching technique for probe stabilisation called the ‘afternoon tea technique’.
Ultrasound-guided central venous and peripheral intravenous (IV) access is a safe and effective method for obtaining vascular access in intensive care and emergency department settings in both adult and paediatric patients. 2 Interestingly, the use of ultrasound for peripheral IV access has been shown to reduce the requirement for CVC in non-critically ill patients. 3
The dynamic and static ultrasound-guided peripheral IV access examinations are being carried out by post-graduate medical and non-medical clinicians globally. 4 It is accepted that probe holding (grip), position and stabilisation are crucial to provide adequate image quality to improve successful IV access.5,6
With increasing access to POCUS equipment, medical schools such as the University of Leeds 7 have begun to educate undergraduate medical students on the use of ultrasound for difficult peripheral IV access. This education is being provided by clinical teachers of grades of foundation year 2 doctors to consultant level.
To encourage medical students and trainees to adopt effective probe ‘etiquette’, to prevent poor probe stability, caused by a pencil/pinch-grip8,9 (Figure 1), and improve image quality, the ‘afternoon tea technique’ was devised as a teaching method. Classically in Victorian Britain, the fifth finger was held out whilst drinking tea in aristocratic households. Therefore, the notion of ‘afternoon tea’ and the concept of ‘keeping your little finger’ in contact with the patient’s skin was created (Figure 2) in a bid to keep the probe stable whilst carrying out the procedure.
Poor probe stabilisation. The afternoon tea technique.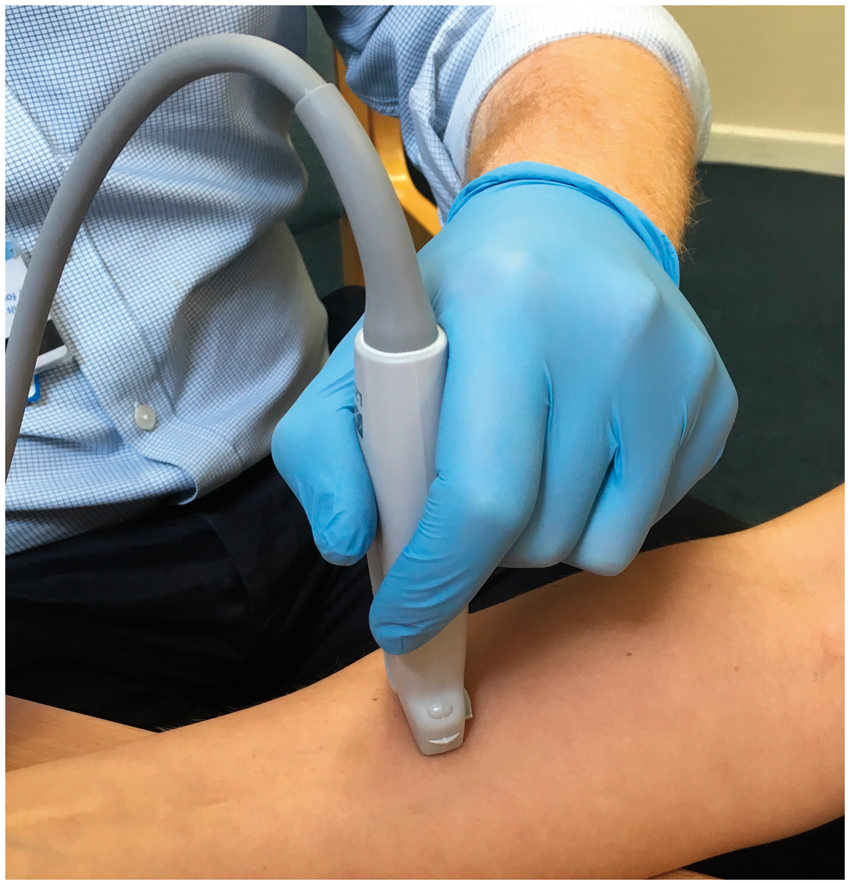

We feel this concept as a teaching aid is one possible fun and simple method to convey the importance of the following:
Probe grip stabilisation in the practice of dynamic ultrasound-guided IV access.5,6 Encourage medical students and clinicians to reflect – on the probe grip and pressure. Previous workers have suggested trainees are often told, by clinical peers and teachers, to press harder and/or grip the probe more tightly.
10
For examinations such as peripheral central IV access, a light grip with no pressure
11
is required to prevent the veins from collapsing when guiding the IV needle cannula into the vessel.
11
The ‘afternoon tea technique' (Figure 2) is an extension of the optimal probe grip: power grip/palmar grip, rather than a pencil/pinch grip, tucking one or two fingers behind the probe (Figure 1) to distribute the weight of the probe evenly across the whole hand.8,9 This grip will help alleviate the risk of work-related upper limb disorder (WRULD) in this emerging group of POCUS clinicians.
This technique, in our opinion, will help to increase the success rate of dynamic ultrasound peripheral IV access and reduce the risk of WRULD.
Footnotes
Acknowledgements
We are grateful to all the students who we educate on the use of ultrasound in the West Yorkshire area, for allowing us to improve our teaching techniques.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
LMcM.
Contributorship
LMcM, SW, MH, SN and AW researched the literature. LMcM designed the teaching technique. LMcM, MH and SN created the first draft of the manuscript. SW and AW wrote the final version of the manuscript. SN and AW were the paper manuscript editors.