
Abstract
Pleural procedures are fundamental skills for intensive care specialists. While competency in these procedures is not explicitly mandated within the Intensive Care Medicine (ICM) curriculum, achieving proficiency remains a vital goal for ICM trainees. Anecdotal evidence suggests that training in this area is often perceived as inadequate, with considerable variability in practice across intensive care units (ICUs). We conducted the first survey of ICM trainees in the UK to evaluate routine practices, formal training, accreditation, and perceived competence. The findings revealed significant gaps in training. Confidence levels in performing chest drain varied widely, and a notable deficiency in thoracic ultrasonography (US) training was identified. Additionally, it was observed that many ICUs frequently rely on non-ICM specialists to perform pleural procedures. These results underscore critical areas for improvement within ICM training. The authors advocate for enhanced education, structured training programmes, and increased support to address these deficiencies. This will ensure that trainees and future consultants are adequately equipped to perform pleural procedures with confidence and competence.
Keywords
Introduction
Pleural procedures are important and potentially life-saving interventions for intensive care unit (ICU) patients but are associated with a risk of significant complications. 1 Achieving competency in these procedures necessitates a combination of theoretical knowledge, technical proficiency, and adequate clinical exposure.
There is considerable variability in who performs pleural procedures for ICU patients during working hours and out-of-hours in UK hospitals. Despite this, no comprehensive study has assessed the experience, training, and confidence level among Intensive Care Medicine (ICM) trainees in performing these procedures.
We conducted a national survey to explore the current practice of pleural procedures within ICUs, focusing on training and confidence levels among ICM trainees from established training backgrounds.
Methods
A web-based survey was designed to evaluate the current state of pleural procedures training, confidence, and exposure among ICM trainees in the UK. The survey also aimed to identify the individuals performing these procedures in ICUs nationwide. It was distributed to ICM trainees across the UK between the 3rd of October and the 30th of November 2024 by the regional ICM trainee’s representatives and members of the Dual ICM & Respiratory trainees WhatsApp group.
Results
A total of 186 ICM trainees from training deaneries across the UK responded to the survey, representing 17.7% of all ICM trainees nationally. The participants represented a range of training levels, ranging from ST3 to ST9.
Of the respondents, 57 (30.6%) were single-specialty ICM trainees, while the majority, 129 (69.4%), were dual-specialty trainees. The breakdown of dual-specialty trainees is as follows: ICM with anaesthesia 79 (42.5%), ICM with emergency medicine 22 (11.8%), ICM with acute medicine 15 (8.1%), ICM with respiratory medicine 10 (5.4%), and ICM with renal medicine 3 (1.6%).
Regarding chest drain insertion and management training, 137 participants (73.7%) reported receiving theoretical and practical training, while 49 (26.3%) stated they had either no training or only theoretical exposure. The lowest proportions were observed among dual trainees in ICM and anaesthesia at 63.3% (50/79) and ICM and renal medicine at 66.7% (2/3). Trainees in ICM and emergency medicine reported 81.8% (18/22) receiving training, while single-specialty ICM trainees had a proportion of 75.4% (43/57). All surveyed dual ICM and respiratory trainees reported receiving both theoretical and practical training.
Only 46 respondents (24.7%) were accredited in thoracic ultrasound (US), while the majority, 140 (75.3%), were unaccredited.
The survey also assessed preferences for chest drain insertion techniques. Half of the respondents, 93 (50%), preferred Seldinger chest drains, whereas only (10.2%) favoured surgical drains. A significant proportion of respondents 72 (38.7%) expressed no preference.
Most respondents 127(68.3%) reported inserting fewer than five chest drains oner the last 12 months. A smaller proportion 26 (13.9%) inserted between 5 and 10 drains, while 17 trainees (9.1%) reported performing none. Only a minority inserted 10–20 drains, 12 (6.5%) or more than 20, 4 (2.1%) (Figure 1).
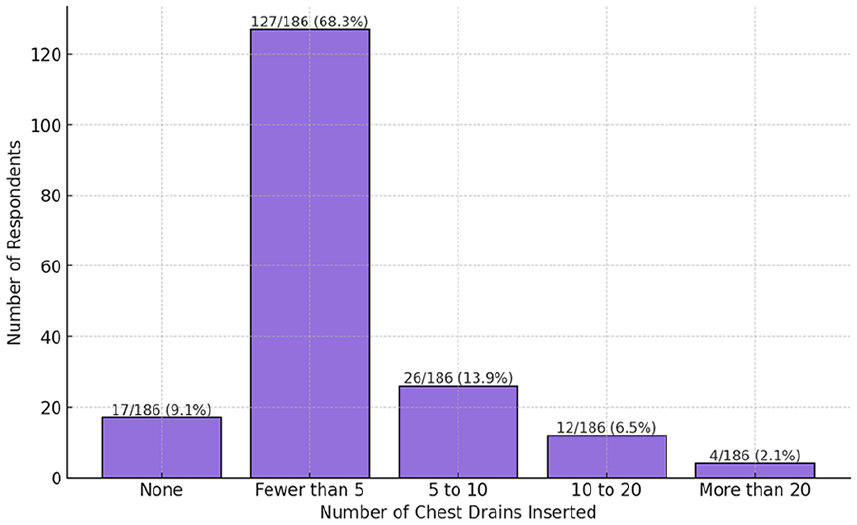
Number of chest drains inserted by ICM trainees in the last 12 months.
Confidence levels for chest drain insertion were evaluated for pneumothorax and pleural effusion. The mean confidence scores were: 7.12/10 for pneumothorax and 6.94/10 for pleural effusion. Notably, confidence improved with training seniority, increasing from 6.3 and 6.1 at ST4 to 8.9 and 8.6 at ST9 for pneumothorax and pleural effusion, respectively. Interestingly, ST3 trainees reported relatively high confidence at 7.0 for pneumothorax and 7.16 for pleural effusion.
Trainees who had performed between 10 and 20 chest drains or more than 20 in the past year reported the highest confidence scores (9.2–10/10), while those who had not performed any scored the lowest (3.8/10). Similarly, dual-specialty trainees in respiratory medicine reported the highest confidence levels for chest drain insertion (9.3/10), while dual ICM with anaesthesia and lone ICM trainees had comparatively lower scores (6.4/10 and 7.1/10, respectively). Those who received training reported higher confidence (7.8/10) compared to those who did not (5.3/10) (Figure 2).
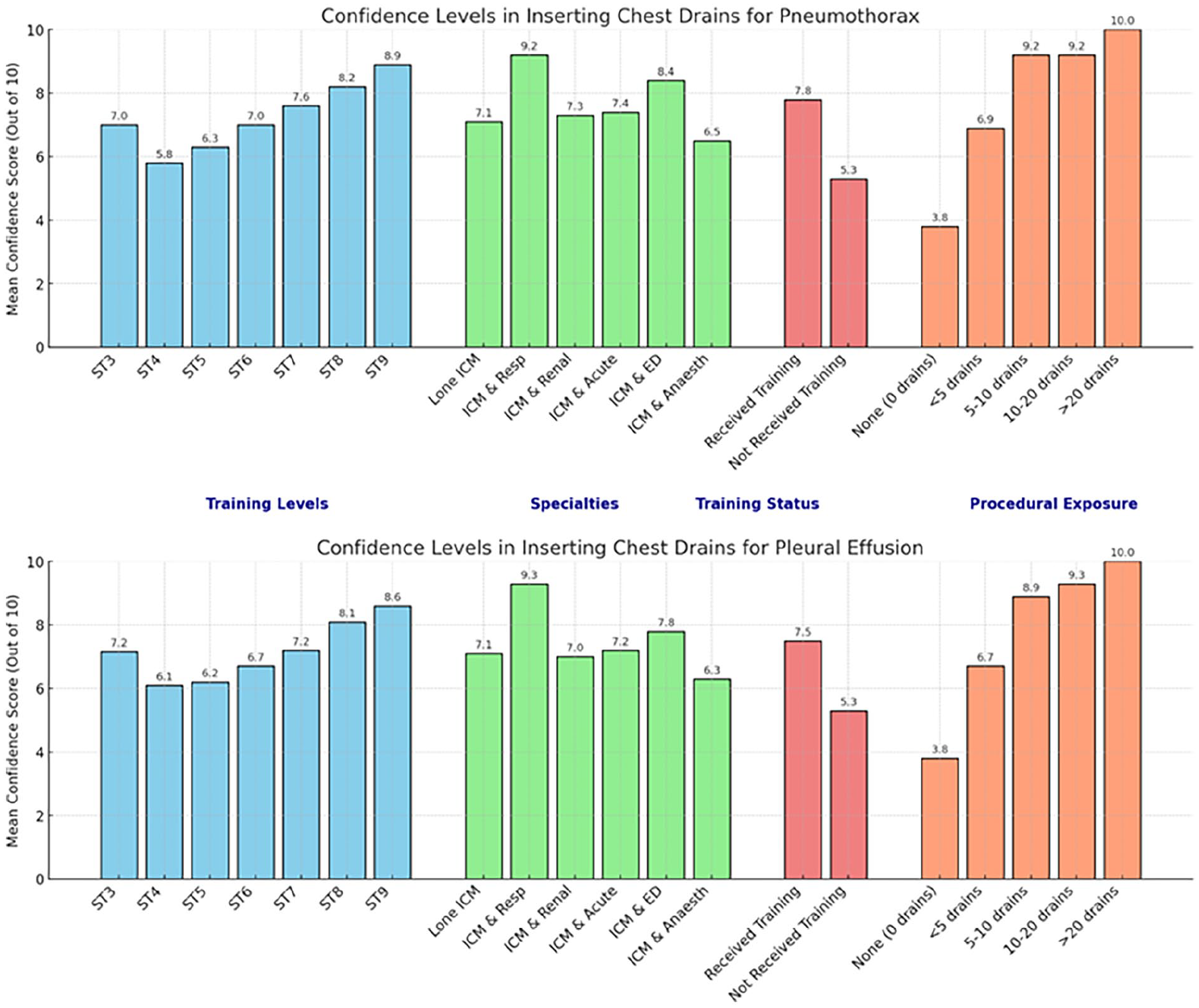
Confidence levels in inserting chest drains for pneumothorax and pleural effusion.
The survey examined which professionals primarily perform chest drain insertions in the respondents’ ICUs. During normal working hours, 48.9% (91/186) of chest drains were inserted by ICM teams, while this figure increased slightly to 62.9% (117/186) out-of-hours, with procedures being performed by ICM trainees or consultants.
Additionally, 24.7% (46/186) of respondents reported that their ICUs relied not only on ICM doctors but also on a combination of other specialties, including respiratory medicine, cardiothoracic surgery, other surgical teams, emergency medicine, and radiology, during working hours. The most commonly involved specialties were cardiothoracic surgery (26%), respiratory medicine (17%), and radiology (17%). This reliance decreased slightly to 19.4% (36/186) during out-of-hours periods.
Discussion
Our survey captured responses from trainees across all training deaneries in the UK, encompassing those from all levels and backgrounds, including Anaesthetics, Emergency medicine, single-speciality ICM, and medical specialties.
While the majority of trainees reported receiving theoretical and practical training in pleural procedures, only a minority were accredited in thoracic US. This highlights a significant gap in formal accreditation, despite the importance of thoracic US in guiding pleural procedures.
Notably, the majority of trainees who lacked formal training in pleural procedures had backgrounds in anaesthesia or single-specialty ICM. This may be explained by the fact that some respondents accessed training or accreditation through joint specialties with respiratory medicine, acute medicine, or emergency medicine, or prior to commencing the ICM training programme. These findings align with a previous survey of non-consultant anaesthetists in a London hospital, which similarly identified significant gaps in formal training and low levels of confidence in performing chest drain insertions. 2
A lack of thoracic US competency, along with inadequate training and exposure to pleural procedures, is not unique to ICM trainees; it has also been demonstrated among higher specialty medical trainees (HSTs) in a recently published regional survey. 3
Most trainees reported a relatively high level of confidence (7/10 or above) in performing intercostal chest drain insertion unsupervised for pneumothorax.
Chest drains insertion is a critical skill, particularly in emergencies such as tension pneumothorax or when present in mechanically ventilated patients. However, a minority of trainees, including those more senior (up to ST6), reported low confidence (3/10 or below) in this area, underscoring the variability in training and experience.
In general, ICM trainees demonstrated good confidence in troubleshooting chest drains, with a mean confidence score of 7.2 out of 10.
Confidence levels were slightly lower for inserting intercostal chest drains for pleural effusion compared to pneumothorax. This is understandable given that only a minority of trainees in our survey were accredited in thoracic US, a skill strongly recommended by the British Thoracic Society for these procedures. 4 Fortunately, the need for emergency chest drain insertion for effusion is less common, and in many cases, intervention can be delayed until a qualified practitioner is available.
However, it is important to note that delays in pleural intervention for patients with complicated pleural infections have been associated with poorer outcomes, including longer hospital stays and increased complications. 5 This emphasises the need for accessible and timely training to ensure trainees are prepared to manage these scenarios effectively.
Our survey indicated that confidence in performing pleural procedures is positively associated with the level of training, procedural exposure, and attendance at pleural training sessions. This underscores the critical role of hands-on experience and participation in practical training sessions in developing competence in these procedures.
Half of the trainees surveyed preferred Seldinger chest drain insertion over surgical drains, while 10% favoured surgical drains. This reflects the current trend towards the use of small-bore Seldinger chest drains.
Our survey highlights variability in who performs chest drains across ICUs and emphasises that ICM trainees are not consistently involved in pleural procedures. Non-ICU specialists contribute significantly to pleural procedures for ICU patients during both working and out-of-hours periods. This may be attributed to a lack of training and lack of thoracic ultrasound (US) competency among ICM specialists but could also stem from local trust policies. These factors have limited the exposure of ICM trainees to such procedures, a situation that was heavily criticised in our survey. Trainees described this lack of involvement as both frustrating and disappointing.
This lack of exposure is reflected in the finding that most trainees, 68.3%, had performed fewer than five pleural procedures in the last 12 months. It has previously been noted that hospital policies allowing only respiratory registrars to insert chest drains risk de-skilling ICM specialists who require competence in these procedures. 6
Although it is understandable that in specific and complex situations, non-ICU specialists – such as cardiothoracic surgeons or radiologists – might be expected to perform pleural procedures for ICU patients, it is the opinion of the authors that this should remain the exception rather than the rule.
Finally, while level 4 competency (‘Trusted to act unsupervised with clinical oversight within training’) in intercostal chest drain insertion was a requirement by the end of Stage 3 in the previous ICM curriculum (2001), 7 the current curriculum is less prescriptive about individual tasks and competencies. This places greater responsibility on individual trainees and their supervisors to identify and address training needs. 8
In our survey, ICM trainees expressed a strong interest in receiving further training and greater exposure to pleural procedures. We believe this is of paramount importance to ensure that ICM trainees and future consultants are both confident and competent in performing these procedures and in teaching them to their junior colleagues.
Conclusion
This survey highlights a potential gap in the acquisition of crucial clinical skills among ICM trainees, particularly those with anaesthetic or single-specialty ICM backgrounds. Thoracic US and pleural procedures are areas that may warrant greater emphasis within ICM training programmes.
A proportion of UK ICUs continue to routinely rely on other specialists to perform pleural procedures for their patients. This practice risks de-skilling ICM trainees and limiting their exposure to these essential procedures.
We hope the findings of our survey will raise awareness of the importance of training and accreditation in pleural procedures and thoracic ultrasound. Additionally, we hope it will support ICM tutors and programme directors in developing appropriate training, education, and support to address these gaps effectively.
Footnotes
Acknowledgements
We would like to acknowledge the members of the dual respiratory-ICM trainees’ WhatsApp group and the regional ICM trainees’ representatives across the country who assisted in distributing this survey.
Author contributions
DS contributed to designing the survey and writing the manuscript. EA contributed to writing the manuscript and making the graphs. AA contributed to writing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.