
Abstract
A challenge lies ahead in ensuring that consultant workforce planning within Intensive Care Medicine meets changing and expanding health care needs at a time of financial constraint. During the development of an enlarging consultant intensivist workforce, it is important to explore existing practices to ensure subsequent contracts provide optimal work intensity and on-call frequency as well as appropriate SPA time for clinical governance and professional development. We conducted a survey across 14 deaneries, 43 ICUs and 398 consultant job plans to compare current working practices and set these against new guidelines and standards. It demonstrated that 93% of consultants work 10 PAs or more, with an average of 5.14 Direct Clinical Care PAs in Intensive Care and an average of 2.14 SPAs. Seven of 43 ICUs had consultant-to-patient ratios greater than 1:8 and 33 ICUs had insufficient resident cover overnight, highlighting challenges with trainee staffing and anticipated service reconfiguration.
Intensive Care Medicine (ICM) within the United Kingdom has undergone several key changes over recent years. We have seen the establishment of the Faculty of Intensive Care Medicine (FICM), an entirely new training programme approved by the General Medical Council and a new commissioning structure with Clinical Reference Group approved standards. 1 All this has taken place on a background of significant financial constraint in the National Health Service (NHS).
The NHS spends 70% of health care funding on clinical workforce 2 and this is higher in ICM. It is also accepted that ICM consultant numbers are likely to increase and this will be a major challenge for managerial budgets. It is likely that current working practices will come under scrutiny.
At present there is scanty data available reflecting the variation in job plans in Intensive Care, in particular the number of Programmed Activities (PAs), Supporting Professional Activities (SPAs) and the provision of dedicated Direct Clinical Care sessions in Intensive Care; each PA and SPA representing a four hour quantum of time dedicated to either clinical or non-clinical time. We developed a questionnaire examining ICM working practices. It was distributed to Intensive Care Regional Advisors throughout the United Kingdom who then forwarded the questionnaire to units covered by a dedicated Intensive Care team or with a stand-alone rota. The intention was to get a better understanding of working practices amongst our Intensive Care colleagues around the United Kingdom and create the opportunity to compare approaches to staffing and service provision.
Our survey coincided with the Intensive Care Society’s published standards for Intensive Care Units (ICUs) 3 and we compared current workforce practices with these standards.
Methods
A questionnaire examining working practice and staffing within individual ICUs was distributed to all deaneries in Great Britain via ICM Regional Advisors in the summer of 2013. Regional Advisors were requested to forward this survey on to ICUs in their region with stand-alone rotas for ICM. Responses were chased by personal email during the autumn of 2013. The survey contained specific questions and the ability to provide a free-text response for clarity. Questions identified hospital type, the number and classification of ICU beds, as well as the numbers of consultants together with details of their job plans including Programmed Activity allocation, on-call and out-of-hours work. Details were also asked about trainee and junior doctor cover.
Responses were used to draw comparisons between staffing levels, practices in individual units and between regions. Comparisons were also made with the recently published ICS guidelines 3 on recommended practice and staff workload balance.
Results
In total, there were 43 responses covering 14 deanery areas. Twenty-five of the responding hospitals had Foundation Trust status, and 29 were teaching hospitals. Eighteen were general ICUs, 4 were mixed general and cardiac, 6 mixed general and neuroscience and 1 general and burns. Two units provided mixed general, cardiac and neurosurgical services, and two provided dedicated neuroscience or cardiac services. Annual admissions and bed numbers are shown in Figure 1.
Critical care bed numbers versus annual admissions per unit (units 13, 19 and 34: data incomplete).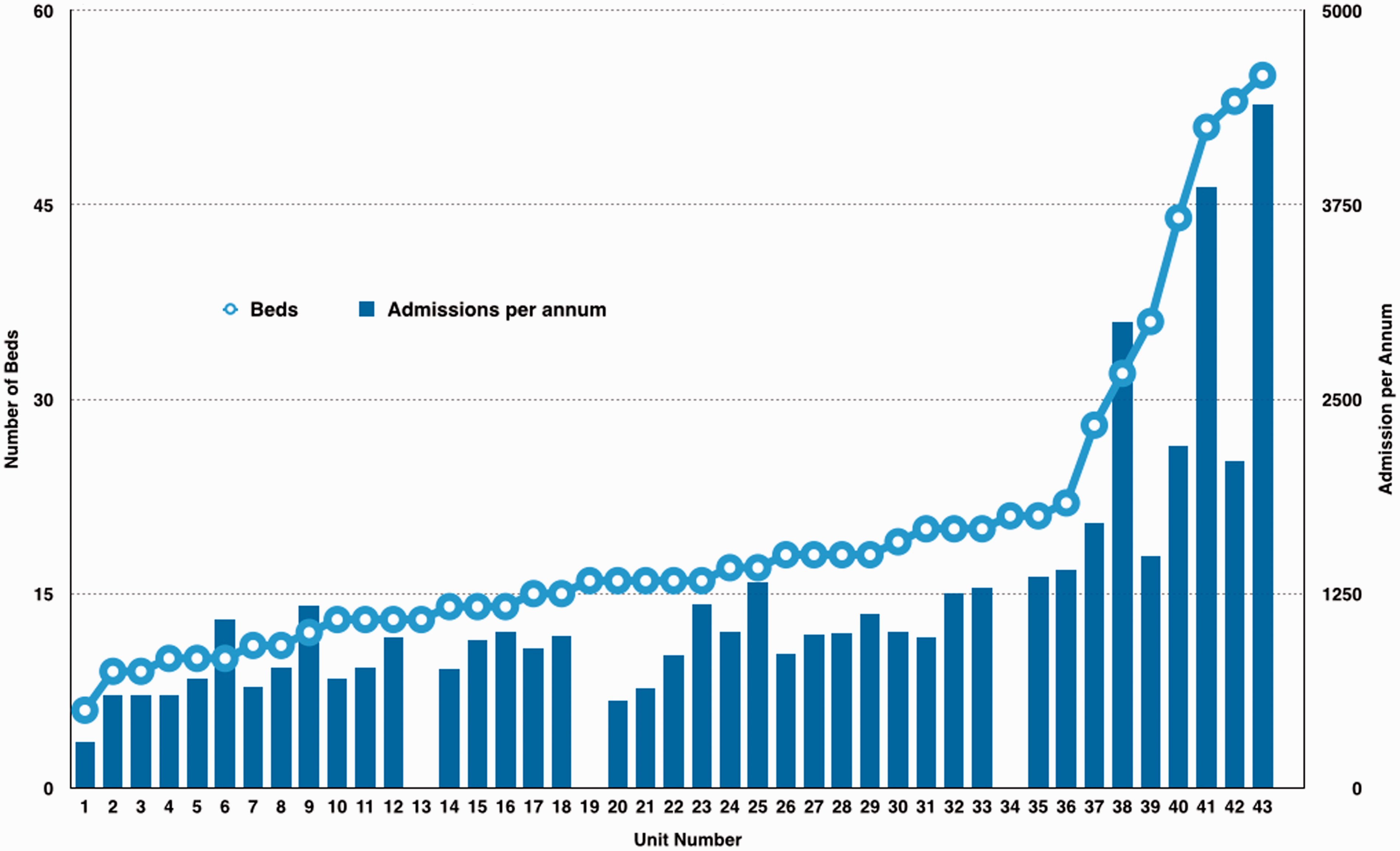
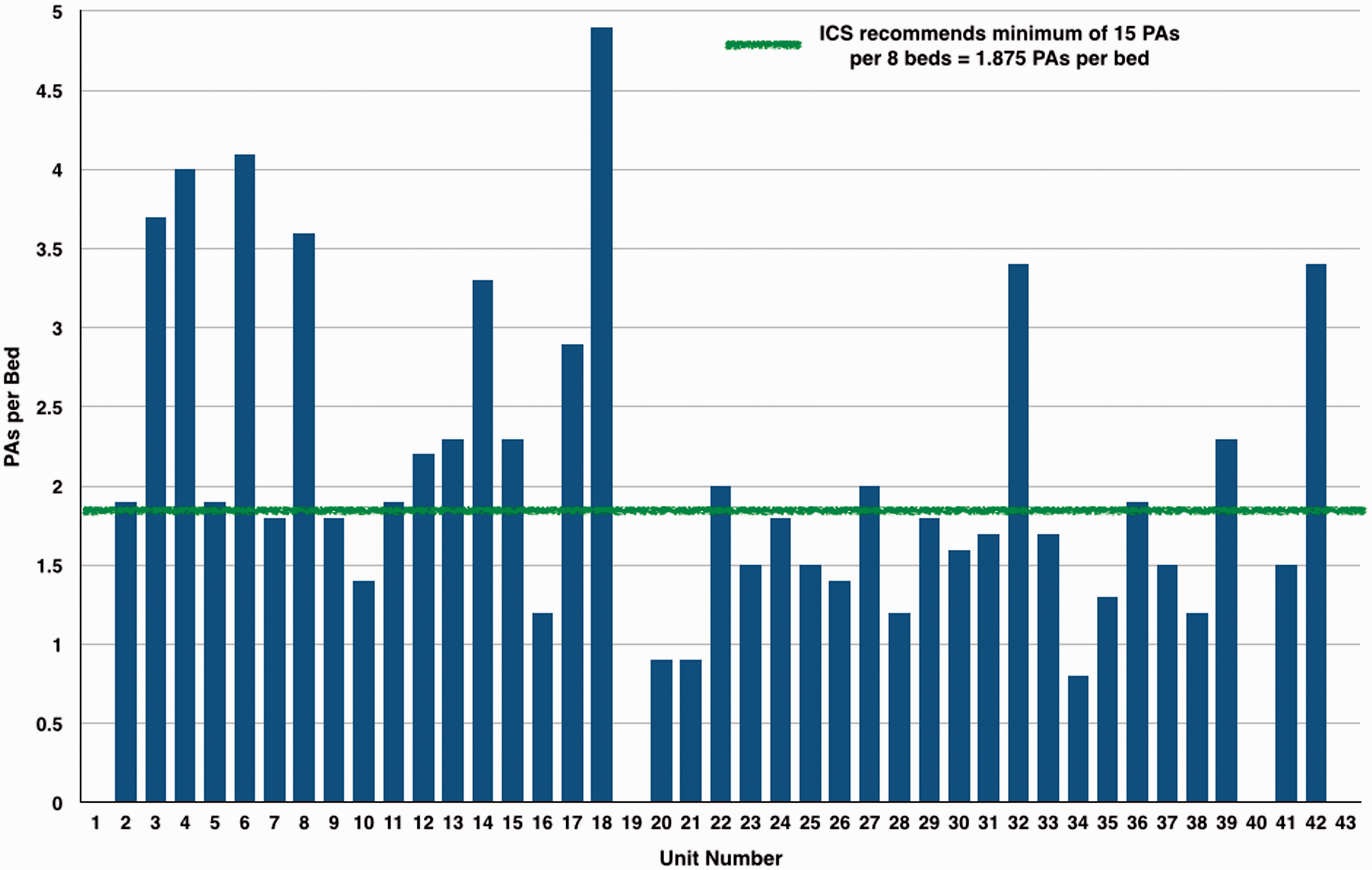
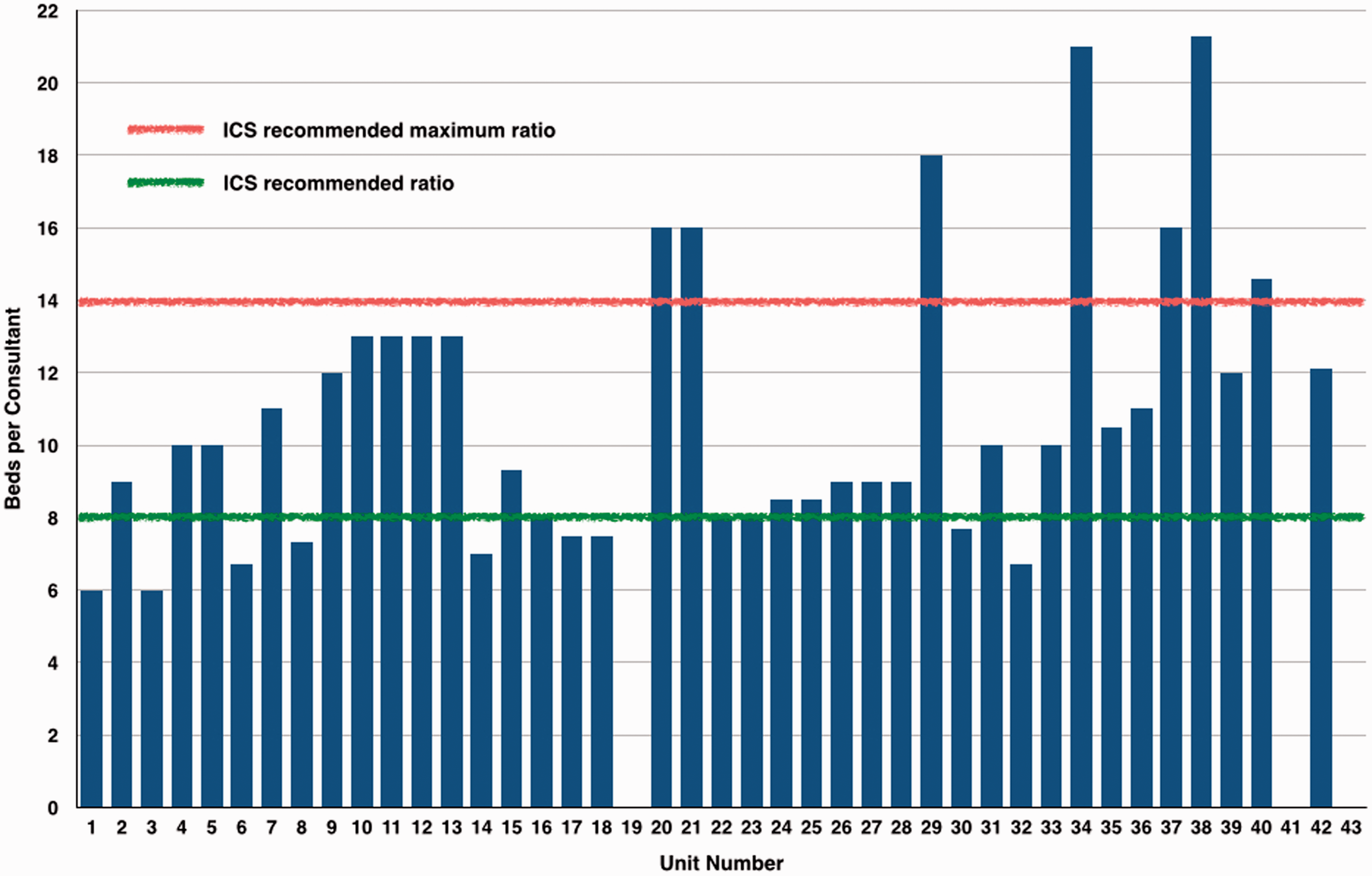
The number of consultants per unit varied from a minimum of 6 up to 33 for the larger mixed units. There was variable individual commitment to ICM in many units, but in 25 the provision of cover was equally shared between the consultants. All units specifying gender of consultants had a male preponderance to their workforce, ranging from 67% to 100%. Details of the number of Programmed Activities (PAs) required for ICU cover in each unit are shown in Figure 2, and Figure 3 shows the number of PAs per bed which demonstrates that many ICUs fall below the ICS recommended standard of 15 PAs to 8 beds. It is recommended that the consultant-to-patient ratio should not exceed 1:15 with a ratio in excess of 1:14 being considered as deleterious to patient care and consultant well being. Our survey identified ratios ranging between 1:6 and 1:21. Thirty-three of the 43 responding units had a ratio of 1:14 or better (Figure 4).
Critical care bed numbers versus Direct Clinical Care PAs to staff unit. PAs per bed. Beds per consultant.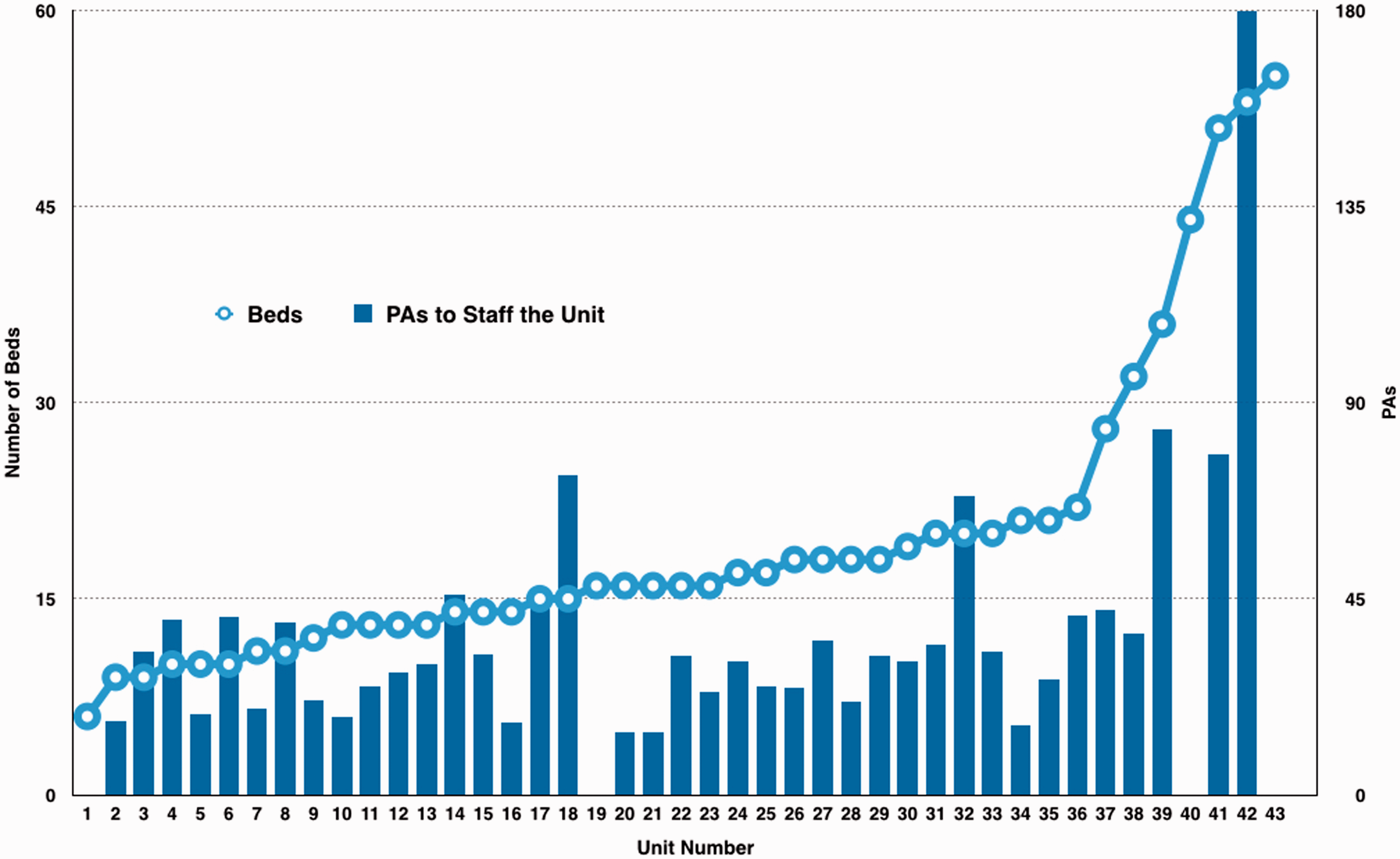
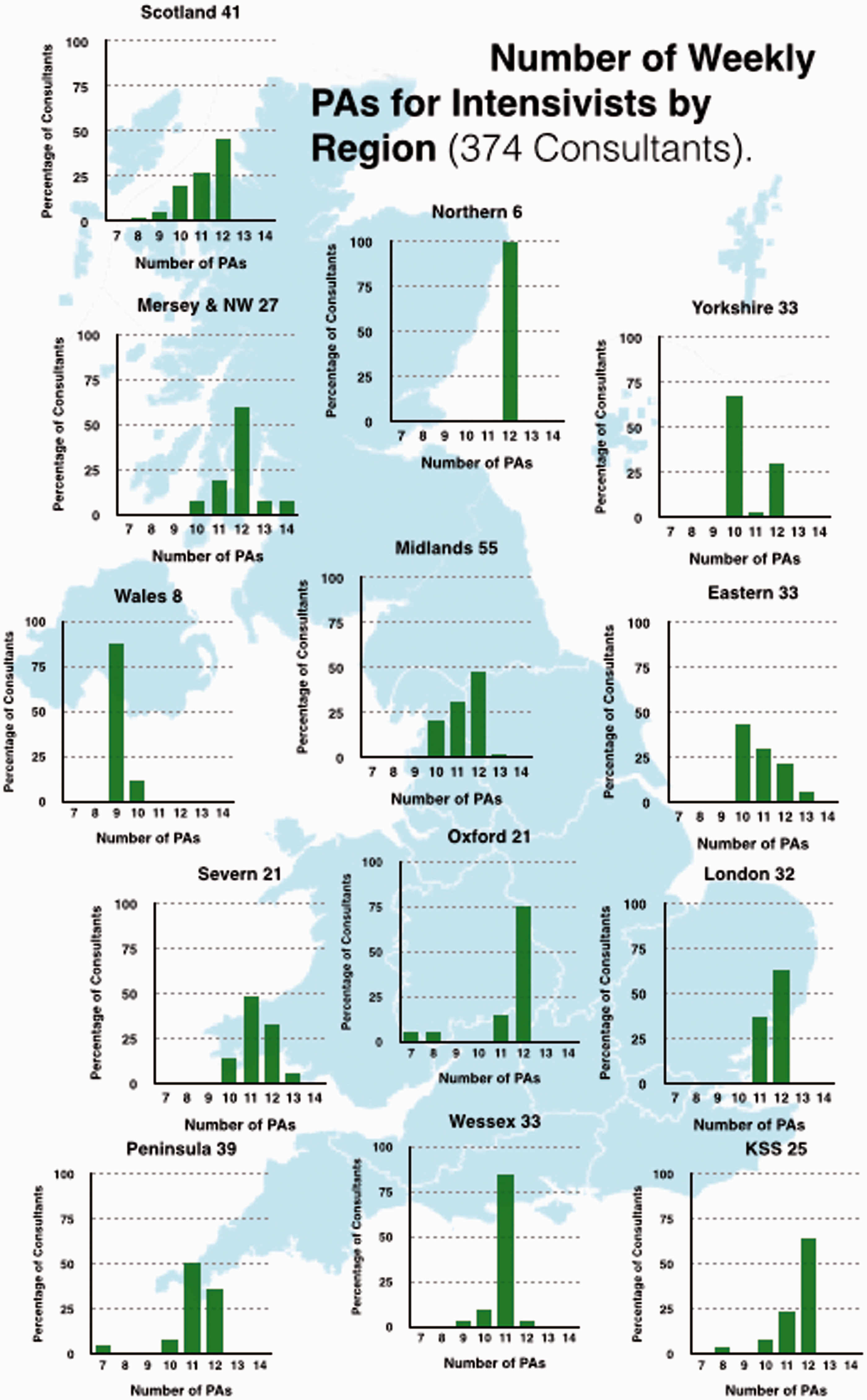
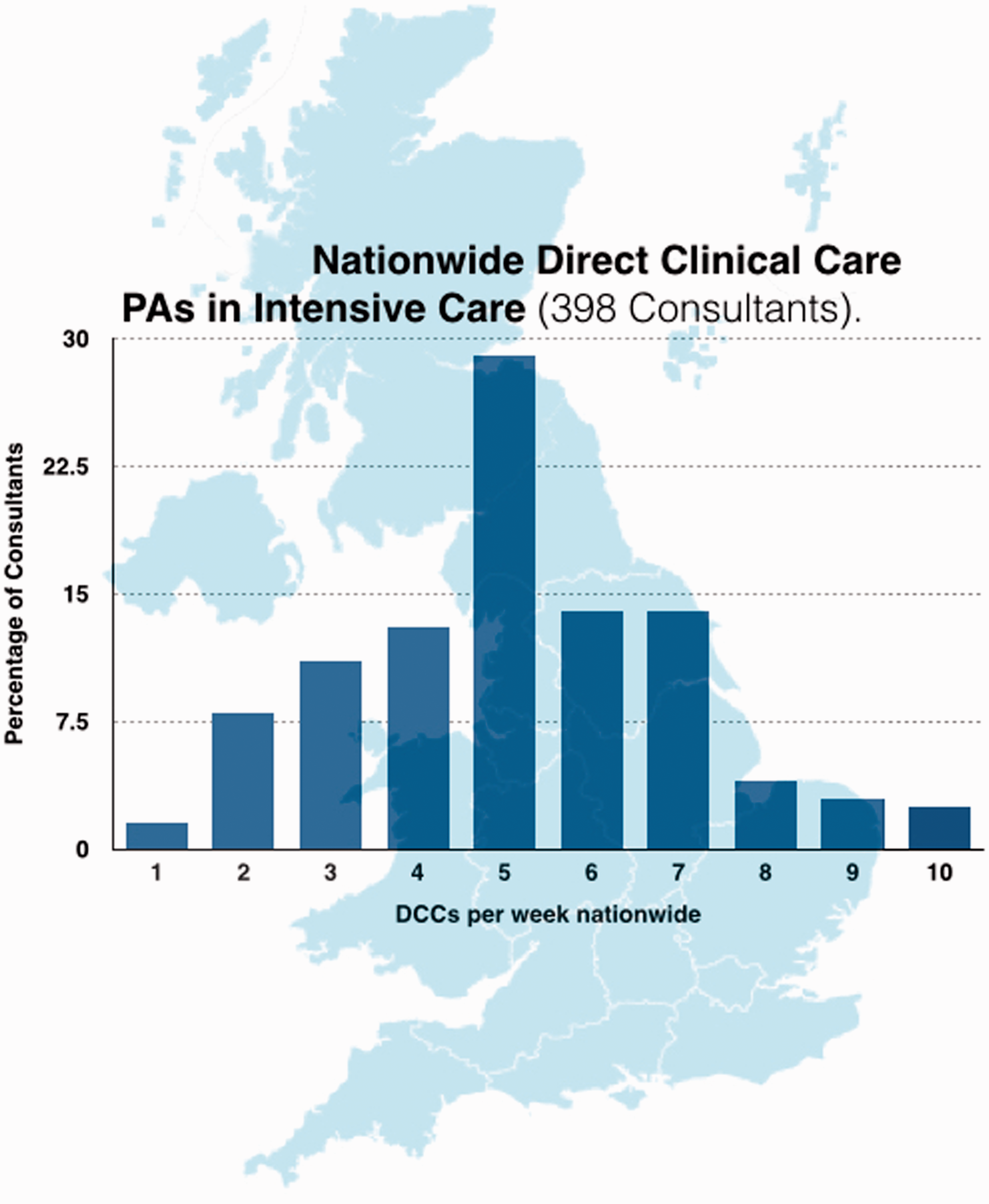
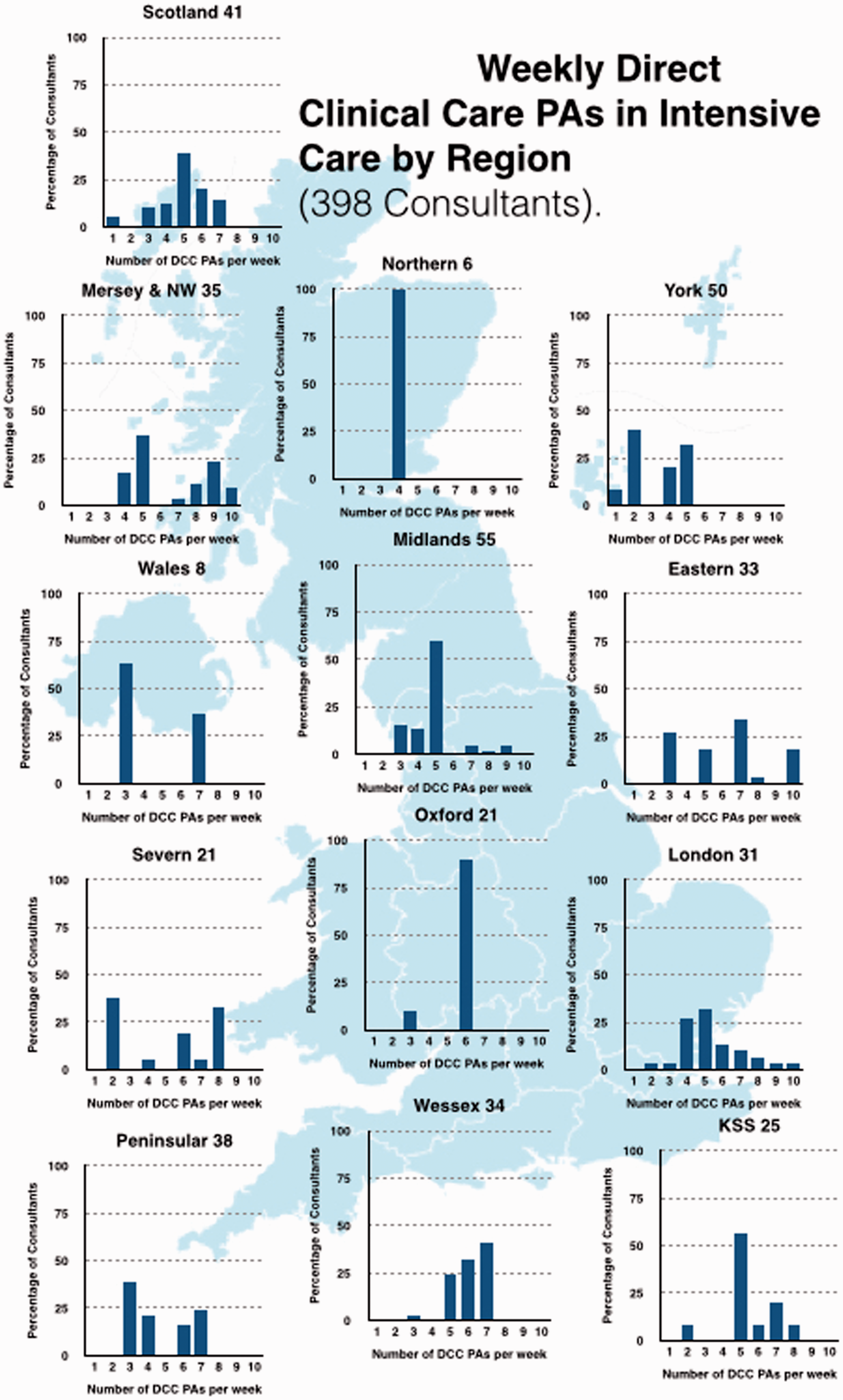
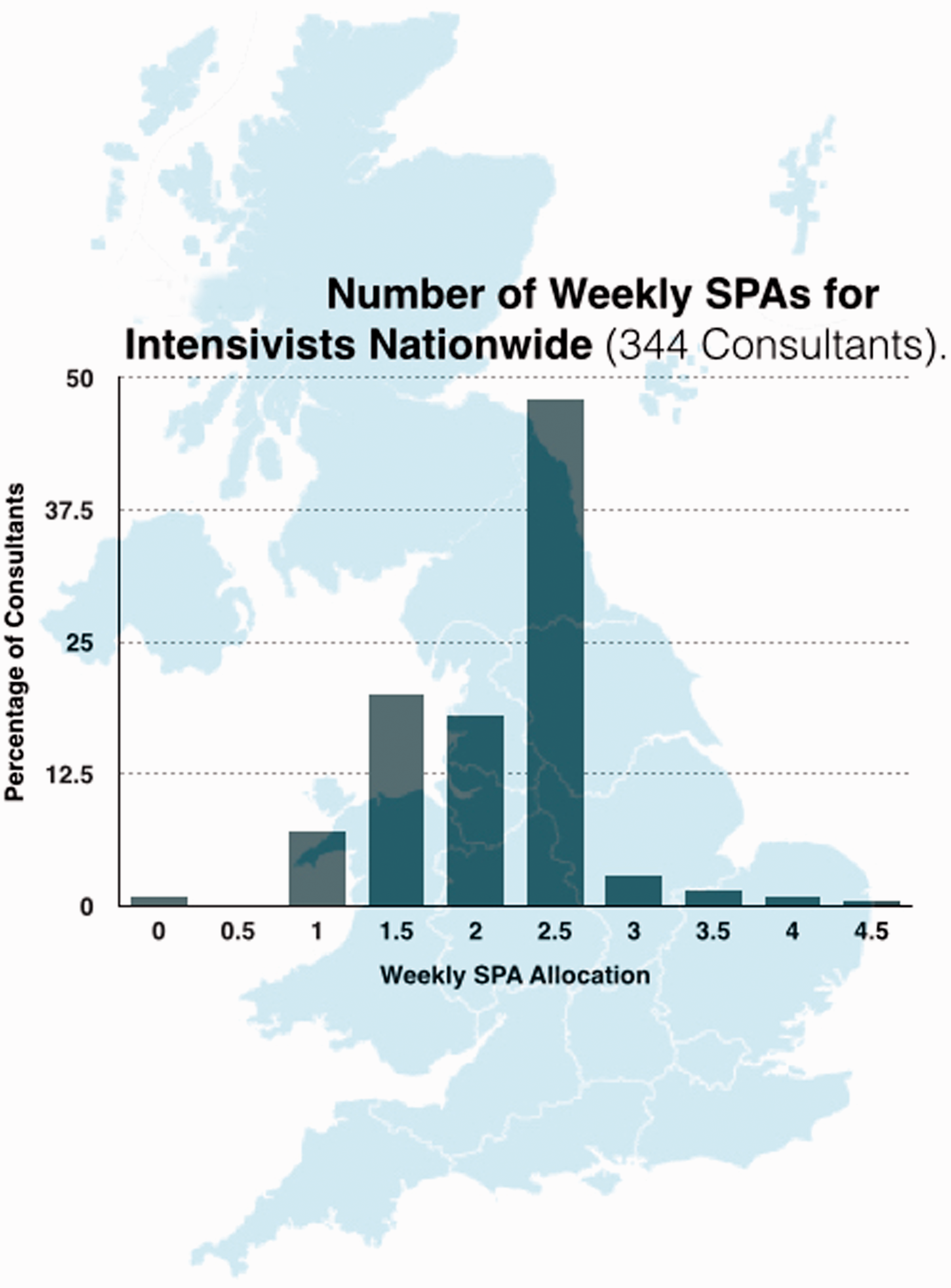
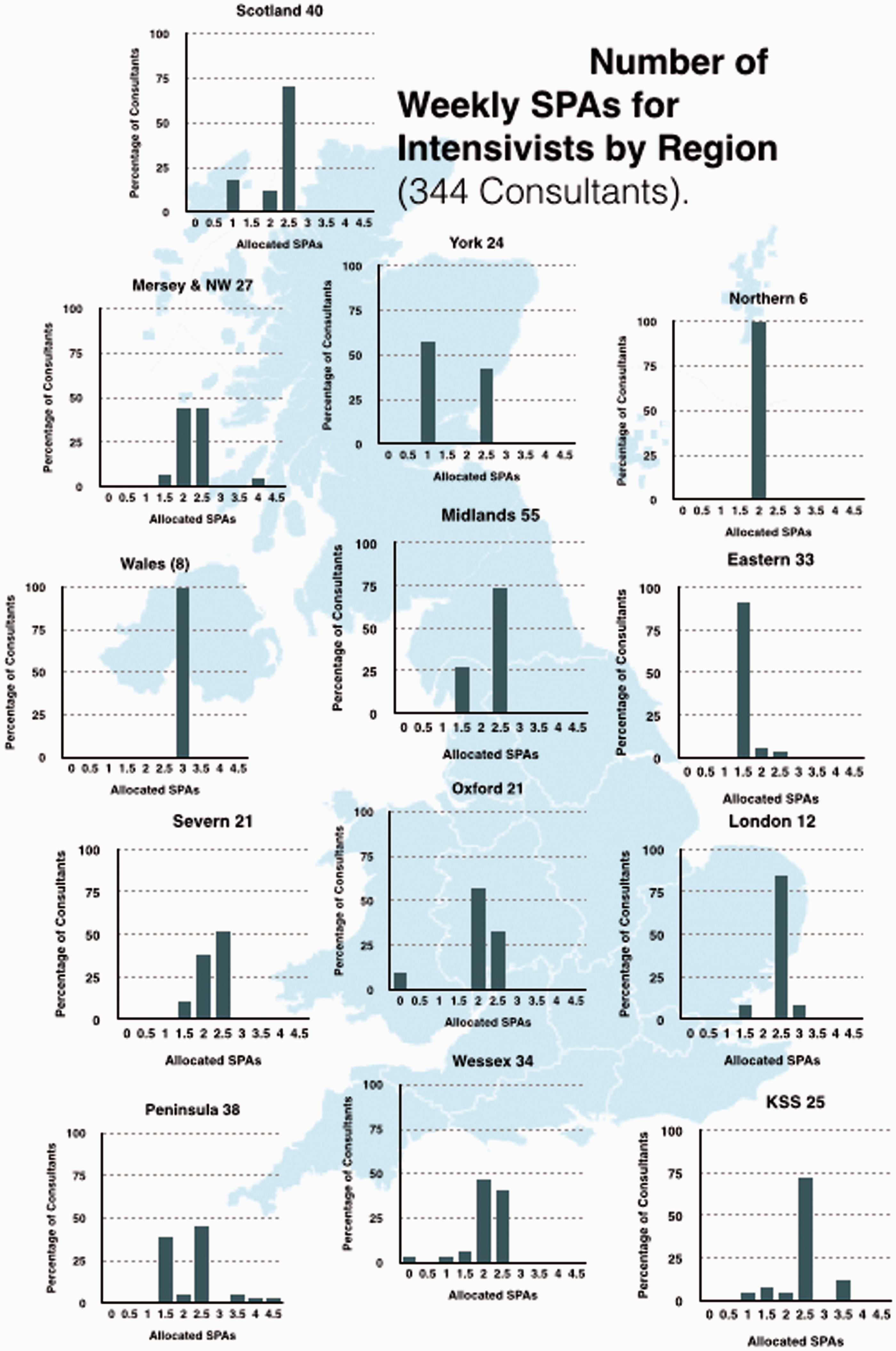
Almost all consultants working in ICM had job plans above 10 PAs in total; 42% had 12 PAs, 33% 11 PAs and 18% had 10 PAs (Figure 5, with Regional breakdown shown in Figure 6). All consultants in ICM had ‘Direct Clinical Care’ (DCC) PAs in Intensive Care incorporated into their job plans (Figure 7, regional breakdown Figure 8). Moreover 98.5% met the guideline that consultants with a daytime commitment to ICM should have a minimum of two PAs devoted to ICM and 79.4% had four or more. The average number of DCC PAs for ICM across the country was 5.14. The Standard NHS Consultant contract recommends that consultants should have 2.5 Supporting PAs (sPAs); the number reported in our survey averaged 2.13 with range of 0–4.5 (Figure 9, regional breakdown Figure 10). Three of the 43 units had compensatory rest under the rules of the European Working Time Directive as part of their contract; but none of these were trusts in which the consultant body were present for large proportions of the night. Half of the 43 trusts had annualised job plans.
Number of weekly PAs for intensivists nationwide (374 consultants). Number of weekly PAs for intensivists by region (374 consultants). Nationwide direct clinical care (398 Consultants). Weekly direct clinical care PAs in Intensive Care by region (398 consultants). Number of weekly SPAs for intensivists nationwide (344 consultants). Number of weekly SPAs for intensivists by region (344 consultants).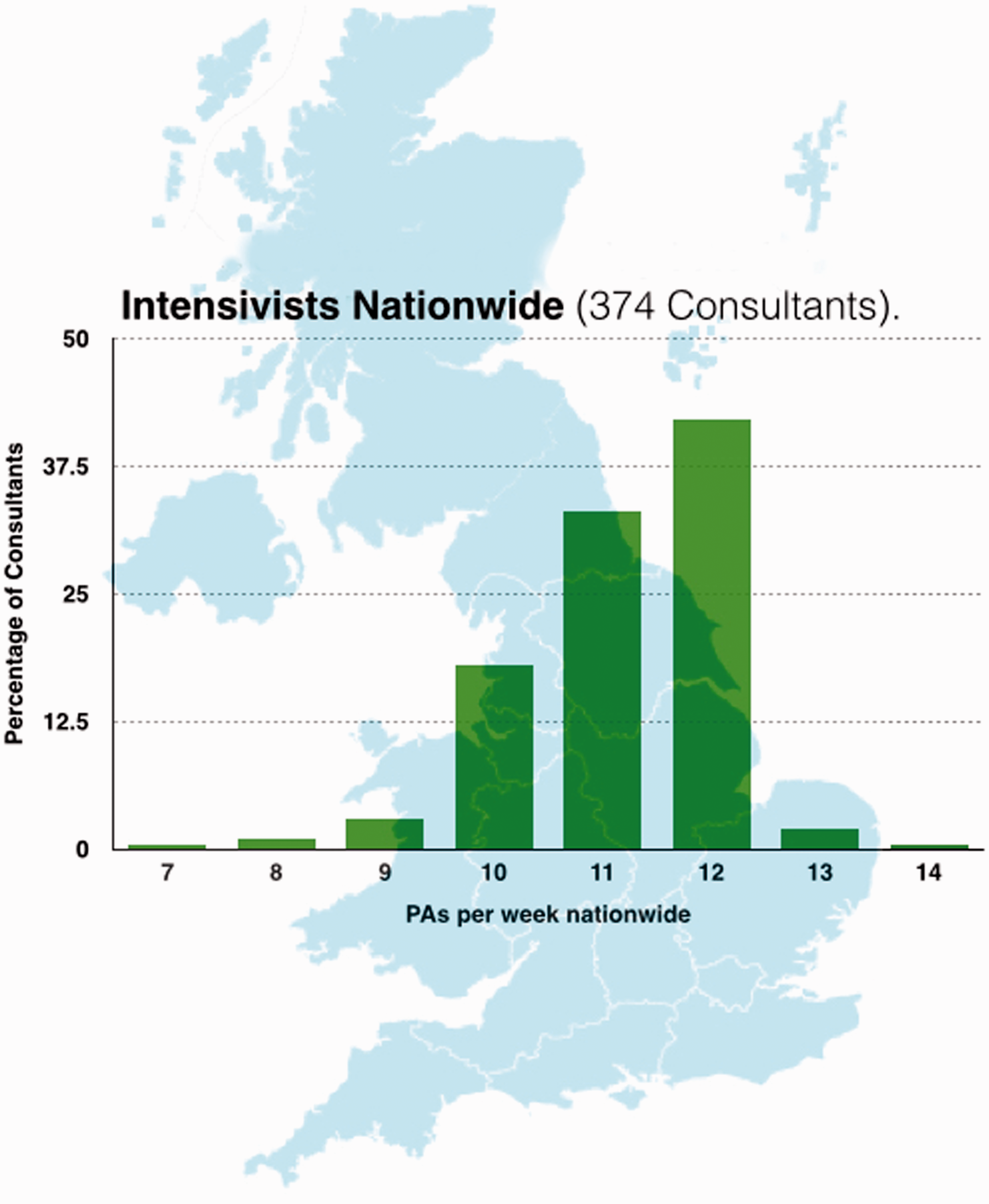
Not all level 3 units had consultants with weekend and public holiday PAs as routine. Weekend practices varied considerably across the county. The majority of trusts provided at least four hours per day, others a minimum of 6 hours left to the discretion of the individual consultants as to the split over Saturday and Sunday.
Consultant weekday on-call frequency ranged from 1 in 3 for some consultants in a London trust to 1 in 14 in parts of Northern and Wessex deaneries. The majority of on-call frequencies were 1 in 6 to 1 in 9, with weekend frequencies similar, and are shown in Figure 11. All on-calls were covered internally.
Frequency and intensity of consultant on-calls.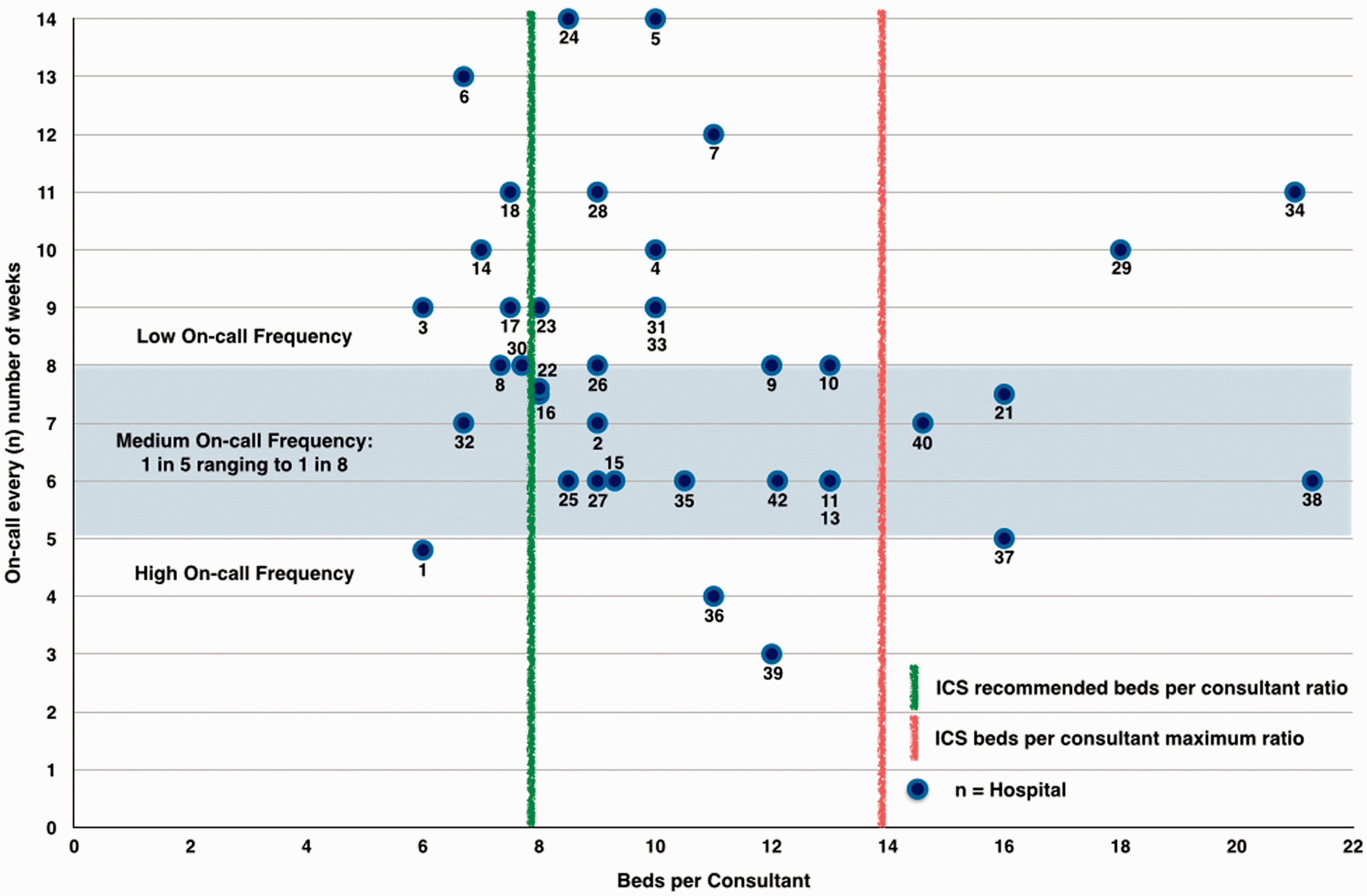
In our responses no consultants were rostered to be resident overnight; however, three separate hospitals from Yorkshire, Northern and Scotland, reported that resident consultants were an anticipated change for the near future. Six trusts had consultants rostered to be present until at least 21:00, with a further four trusts stating that consultants were often present until midnight or for large proportions of the night. Only one hospital received no PA allocation for out-of-hours advice.
In general, the majority of units appeared well staffed with juniors during the day (Figure 12). On a normally staffed day, only 6 of the 40 responding hospitals fell short of the ICS standard of a 1:8 resident-to-patient ratio. The range in resident-to-patient cover ranged from a ratio of 1:1.8 to 1:21 for weekday cover and the trusts with the least daytime cover came from Mersey, Yorkshire and Northern Deaneries.
Beds per trainee during day shift on a well staffed day 6 out of 40 units exceed the upper limit of 8 beds per trainee, rising to 14 out of 40 units when including units on a ‘bad day’ – as depicted by the bars crossing the red line (units 13, 19 and 43: data incomplete).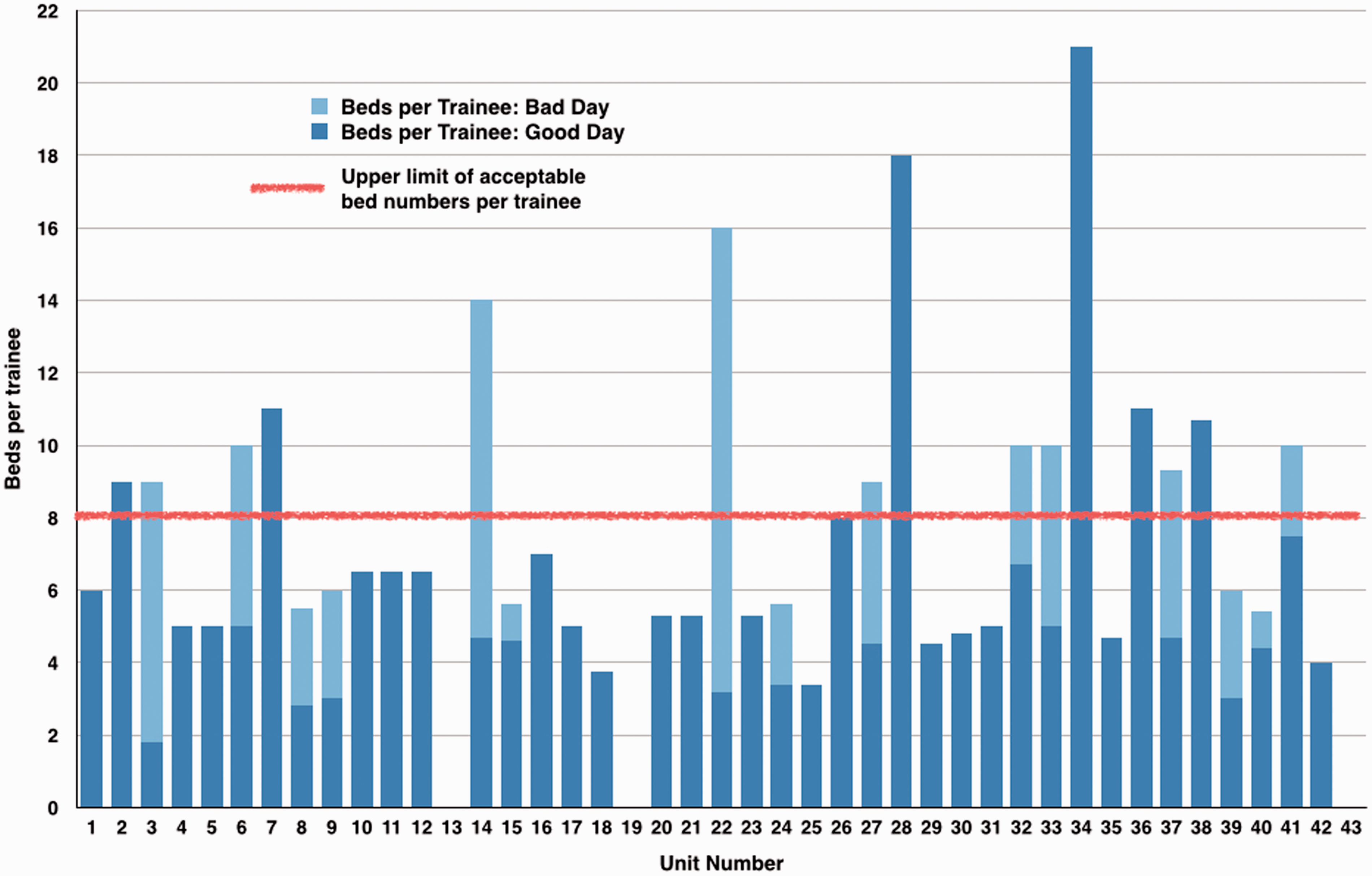
Night time cover tended to be more sparse (Figure 13). Only seven trusts had a resident-to-patient ratio less that 1:8, with 33 hospitals exceeding recommended ratios of cover. Cover ranged from a ratio of 1:5.7 to no junior cover overnight. The mean average was 1:11. Only 15 of the 40 trusts specified having dedicated Specialist Trainee cover overnight. Higher ratios did not reflect experience of trainees. Several trusts had a sole Core Trainee responsible for covering between 10 and 14 patients; however, these units were often Neurosurgical and not General Units. As per ICS guidelines ‘residents’ describes trainees at Foundation year 2 or above or Advanced Critical Care Practioners. Foundation year 1 doctors were not counted in the calculation of resident staffing ratios.
Beds per trainee during night shift overnight only 7 out of 40 units lie on or within the recommended limit of beds per trainee , as shown by the bars not crossing the red line (units 13, 19 and 43: data incomplete).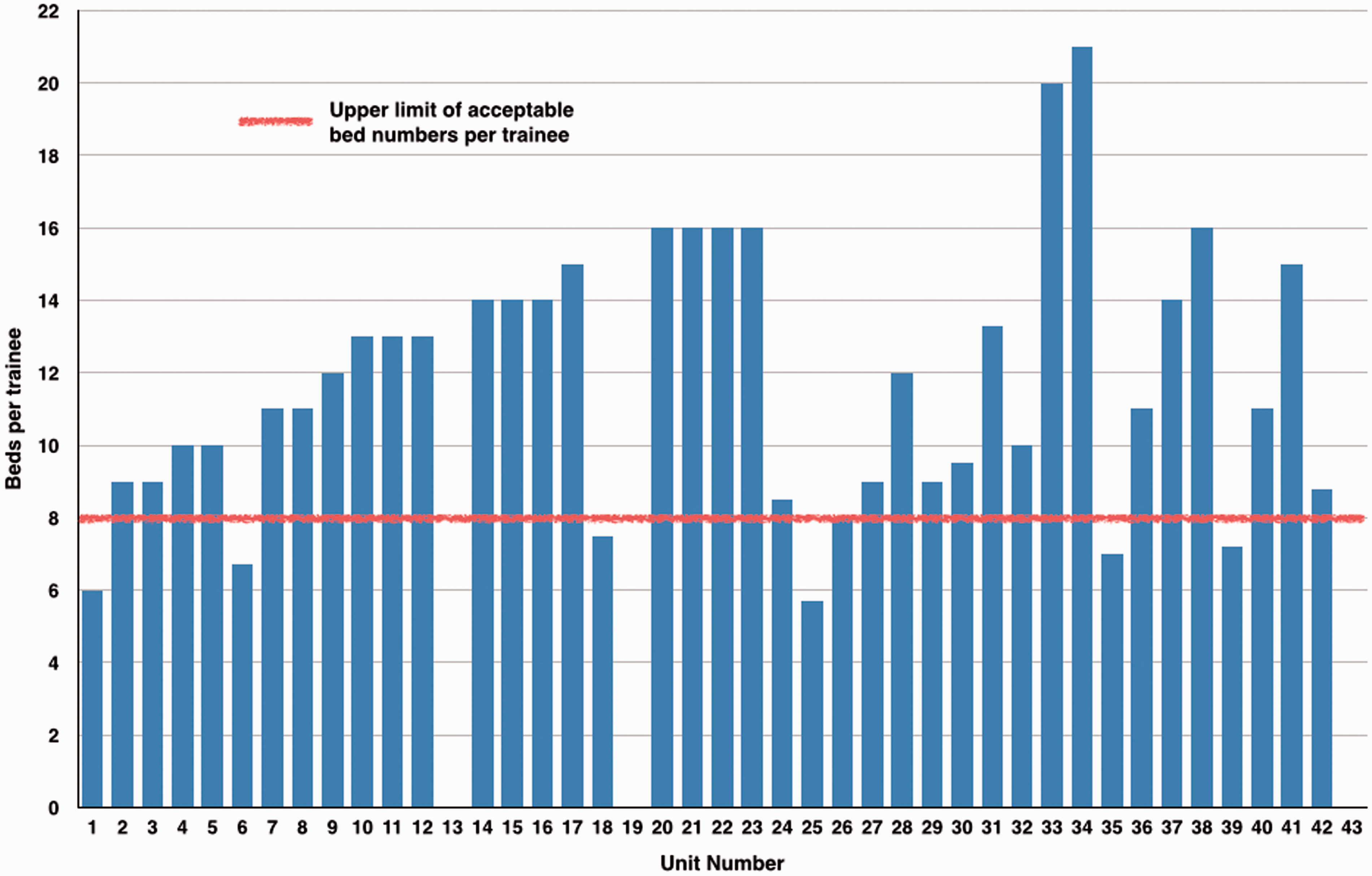
On further analysis, it is clear that despite daytime junior staffing appearing to be in line with the recommended ratio of resident to patient not exceeding 1:8, the level on many units does not meet this on all days due to variation in staff availability during the week. Looking at the same units on days when numbers are reduced due to expected rota variations, 15 out of 43 units had insufficient staff. Units also varied considerably in terms of seniority of trainee cover. In several instances, rostered doctors had responsibilities outside ICU overnight, such as maternity and theatres. Furthermore, doctors allocated to ICU may spend a large proportion of their time off the ICU attending reviews, medical emergency and trauma calls.
Scotland and West Midlands deanery already utilise Advanced Critical Care Nurse Practitioners to provide day and night care on their ICUs, with plans to recruit further nurse practitioners to meet demands as units expand or as it becomes harder to fill junior posts with doctors. Scotland and Yorkshire reported a reduction in numbers of doctors in training.
Discussion
Our survey demonstrated considerable variation in working patterns and staffing over the United Kingdom. Despite a considerable proportion of responding ICUs providing cover in line with the Intensive Care Society’s 2013 recommendations for Consultant ratios and PA allocation 3 there were notably less PAs per bed in 20 of 39 responding ICUs (Figure 3) and 7 of 43 ICUs had consultant-to-bed ratios greater than 1:8.
There are regional variations in Job Plans for Consultants, with the biggest variation from recommendations being in sPAs. The Academy of Medical Royal Colleges and The Royal College of Anaesthetists see the typical 7.5:2.5 split as being the basis for a safe contract, 4 regardless of the financial pressures on the NHS. This is supported by the BMA. 5 The minimum time required for a consultant to just keep up to date is 1.5 SPAs. 4 Notably 46% of job plans had less than 2.5 SPAs and this seemed to be an increasing problem for new consultants negotiating contracts.
There is considerable variation in on-call and out-of-hours commitment for Consultants between the units surveyed. The 2003 consultant job contract 6 outlines a high frequency of on-calls to be 1 in 1 to 1 in 4 and low frequency to be 1 in 9 or less frequent. Twenty trusts fell into a desirable medium frequency of 1 in 5 to 1 in 8.
The survey demonstrated the discrepancy between junior staffing during daytime on differing days of the week according to rota variations but more noticeably at night time when only 6 of 43 ICUs maintained junior staffing levels within the ICS recommendations. Problems with junior staffing were further emphasised in free text comments when issues with the relative inexperience of junior doctors or insufficient numbers passing through to appropriately staff units was frequently mentioned.
Although it is recommended that there must be immediate access to a practitioner who is skilled with advanced airway techniques 3 the feedback was that juniors were often inexperienced with no airway experience or Core Trainee year 1 in anaesthetics with only 6 months experience. Several units also included Foundation Year 1 doctors in their staffing. The current ICS recommendation is that it is not appropriate for foundation year doctors to be left as the sole resident on an ICU. In an attempt to resolve this, some units use advanced nurse practitioners and others described plans to train and recruit more of these.
There is certainly a demonstrable demand for more intensive care beds across the country, along with a push for consultants to be available 24/7 across many specialties as highlighted in the 2012 Academy of Medical Royal Colleges document ‘Seven Day Consultant Present Care.’ 7 Certainly, it will be expected to be implemented in high acuity specialties such as Intensive Care with the expressed goal of improving quality of care for patients. The Academy recognised that these standards were unlikely to be implemented with current resource arrangements and anticipated that service reconfiguration would be required.
A further anticipated change in line with providing 7-day cover is the move towards Intensive Care consultants being resident on-call overnight. Many units already provide consultant cover until late evening, with a small proportion of consultants finding themselves in until midnight or overnight on up to 40% of occasions, in part related to patient numbers, acuity and junior staffing level.
A large proportion of units voiced active plans for expanding bed numbers or service reconfiguration including the amalgamation of different specialty ICUs and consultant bodies. Many units expressed uncertainties as to the success of implementing these changes in terms of geographical challenges and staffing. For one trust it is expected that a single consultant will be required to cover two separate units in the near future. Several units stated that although there was a recognised need to increase bed numbers, funding for both beds and staff was not available.
Several units had consultants with PAs dedicated to supporting outreach services. Staffing and supervision was variable, with some providing a consultant-led service Monday–Saturday or Monday–Friday and others providing purely nurse-led services. A few more discussed plans for further development of such services in the future but highlighted a lack of funding. This will also be an area of change for intensive care consultants to consider over the next couple of years. At present NICE 8 does not dictate that Intensivists be the preferred support strategy for individuals with a deteriorating clinical condition; but it is likely that this will become a specific recommendation in the future.
Our survey had a number of limitations. As is common with questionnaires we are aware that we did not achieve a 100% response rate, we mitigated this with repeated reminders and personal contact, which did increase the replies. It is unlikely that the remaining units would have changed the results very much in this observational survey. The ways that job plans and rotas are described varies considerably between different organisations, and in the common parlance within an organisation; for example, one persons’ ‘on-call rota’ may be a 1:4, and another could interpret it as a 1:5 depending on how annualisation is included. In this example we would have based our values on a 365-day year, and if in doubt we asked for further information, but we may have made some misinterpretations despite this scrutiny. Lastly, we have made some assumptions about the experience of junior staff. Certainly, depending on where and how this experience is gained, variations will exist between apparently similar grades around the country. We do not think that any of these considerations impact significantly on the message of our survey.
What will our working practices look like in the future? Surely PAs will have to be allocated for all work. Will more contracts be annualised and compensatory rest negotiated? As pressures grow will Intensive Care remain largely a male-dominated specialty at senior level? Will we see more beds in fewer centres, with 24/7 resident consultant cover? Will there be more advanced critical care practitioners and at what cost to the training of future consultant intensivists?
In summary, our survey demonstrates a wide variation in the workforce practices for delivering Intensive Care Services in the United Kingdom. The results of our survey give a baseline for assessing future changes, and highlight areas where variation in provision could be explored locally.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.