
Abstract
Following two studies done in 2007 and 2009, a follow-up of the adherence to the suggested guidelines on drug standardisation has been performed with a suggestion for future standards that can be achieved, to complement the recently published Carter report. The Intensive Care Society (ICS) introduced recommendations for infusion concentrations of 16 medications commonly used in critical care areas. The importance being improvement in patient safety and rationalised use of available critical care resources. Five years after publication of these recommendations, a further audit has been undertaken to assess the level of acceptance and application. This revealed that 89.5% of the 133 surveyed units (representing 42.49% critical care units across the UK) have adopted the recommendations. There are further medication concentrations which could also be standardised.
Introduction
Patient safety related to medications is of concern within the critical care area. Several medications commonly used in critical care are considered as high-risk medicines, for example, anticoagulants, injectable sedatives, opiates, and insulin. 1 The intravenous (IV) route is one of the most common routes for administration of medication in critically ill patients2,3 and may compound medication errors due to the complex multiple processes 4 involved in administration.
One direct observational study determined that medication errors related to continuous infusion usage during ICU stay was 105.9 per 1000 patient days. 3 In addition to causing patient harm, injuries caused by medication therapy in critical care areas are also thought to increase the hospitalisation costs. 5
The preparation stage in particular has been reported as a medication error determinant, leading to infusion concentrations that were either under or above the prescribed concentrations. A study that observed morphine infusions in a neonatal and paediatric intensive care found that 65% of the prepared infusions had concentrations more than 10% of the expected concentration, with 6% of the samples containing twice the expected concentration. 6 Similar findings were reported in a study from an adult neuroscience critical care unit in the UK, where the majority of dopamine, noradrenaline, and potassium infusions prepared at the patient’s bedside (on-ward preparation) had differing concentrations of more than 10% of that charted. 7
Complex calculation, difficult volume measurement, and the mixing process were reported to be factors influencing errors during preparation of IV medications. Therefore, standardising medication infusion concentrations may minimise errors related to infusion preparation, along with reducing the large number of individualised concentrations. This is also a valuable aid to safety when junior doctors move to a new post, a point made in the original survey.8,9
ICS recommendations on medication concentrations in critical care areas. 10
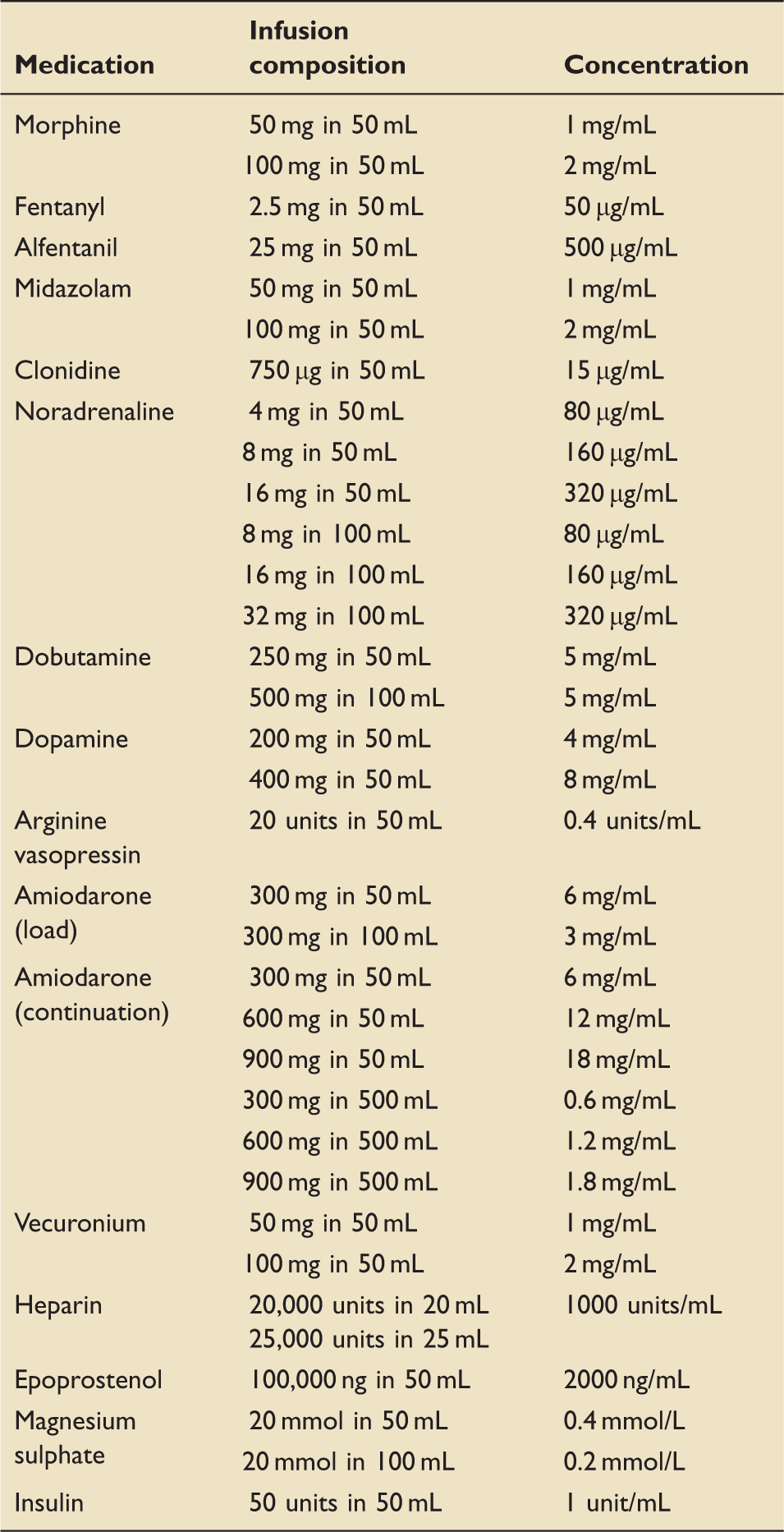
This audit study has been undertaken to identify the level of acceptance and application of these ICS recommendations within critical care units in the UK. This study has also looked at medications in critical care areas which have not been standardised by the ICS, with the intention of increasing the number of standardised medication concentrations.
Methods
An online, self-administered questionnaire was used to ask whether respondents have taken ICS recommendations of medication infusion concentrations into account when designing policies and procedures for their units. Participants were also asked whether they were using the recommended infusion concentrations for each medication listed in the ICS recommendations. If another infusion concentration was used, participants were asked to specify their alternative.
Participants were also asked to state how their medication was prepared. They were given four options: ready-to-use, ready-to-administer, pharmacy pre-prepared, or on-ward preparation. The last part of the survey queried the infusion concentrations used for five medications which have not been standardised by the ICS, namely remifentanil, dexmedetomidine, adrenaline, potassium chloride, and phosphate.
The data collection process started on the 9th June 2015 and ended on 26th June 2015. A hyperlink to access the online questionnaire was circulated via the United Kingdom Clinical Pharmacy Associations Critical Care Group message board as well as the UK Medusa Injectable Medicines Guide website mailing list. A reminder e-mail was sent out twice, on 19th of June and 22nd of June 2015. Participants were invited to ask questions about the study using the e-mail address provided.
The data obtained from the responses to the online questionnaire were statistically processed using Microsoft Office Excel spreadsheet software 2010 and IBM SPSS Statistics software version 22. Descriptive analysis was used to calculate the number of critical care units that applied the ICS recommendations, overall and for each of the medications, in their practice.
Results
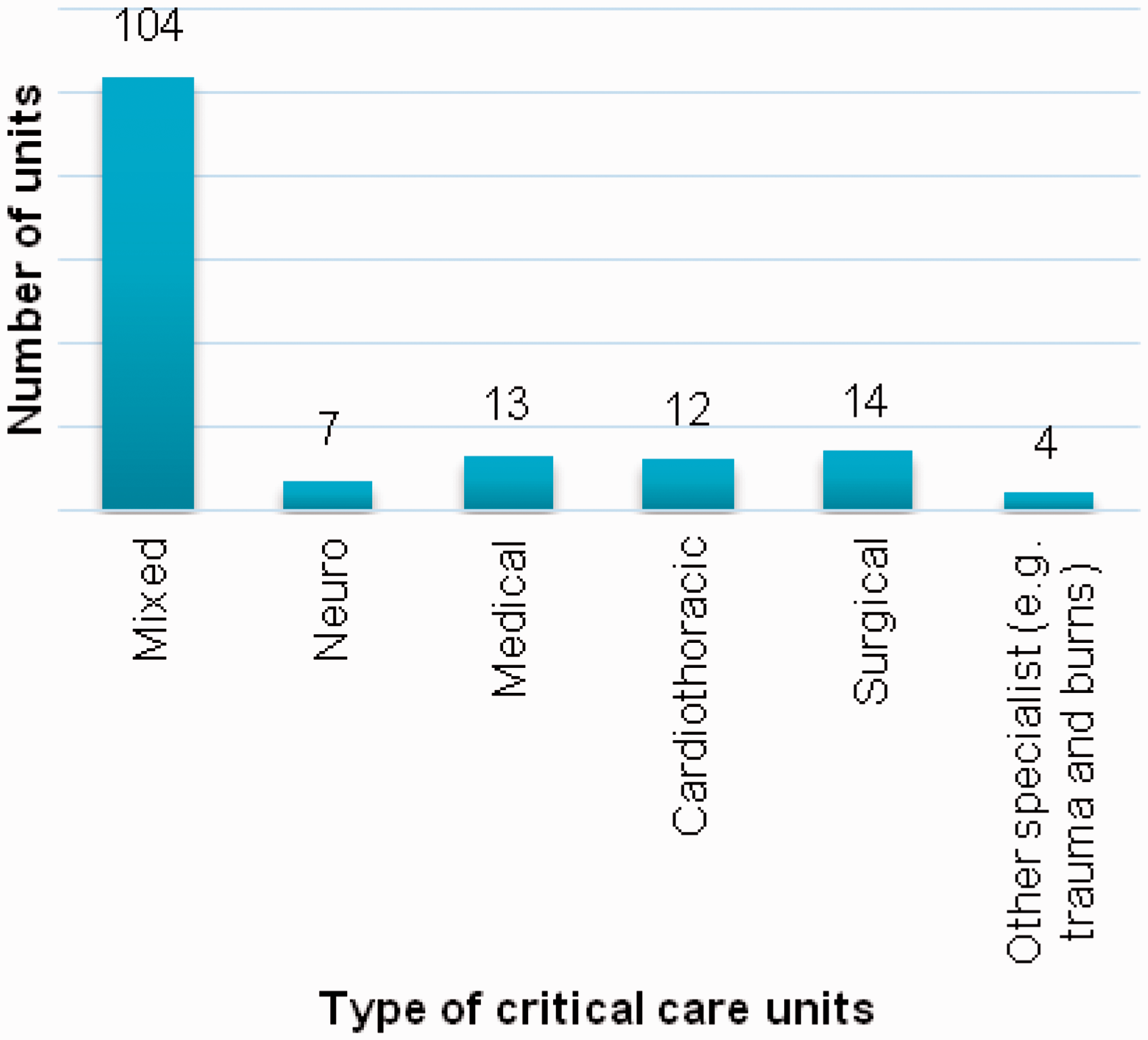
One hundred and thirty-three survey responses from 133 different adult critical care units were collected. This represented 42.49% of the critical care units across the UK. Responses were received from all parts of the UK (Figure 1) as well as from various critical care unit types (Figure 2).
Number of responses by country. Number of responses by type of critical care unit.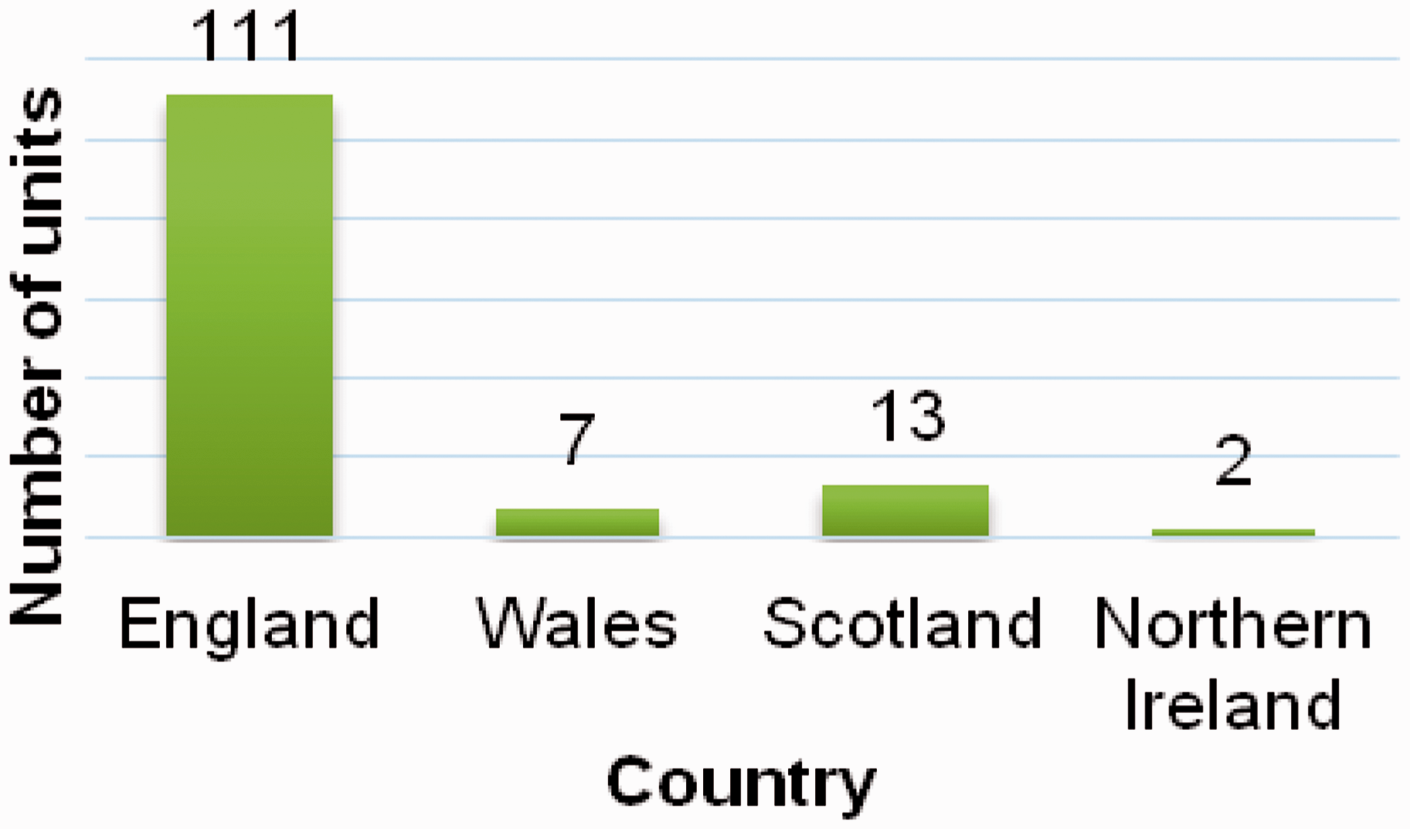
ICS recommendations on standard medication infusion concentrations in critical care areas have been adopted by 89.5% of the respondents (119 units) where the recommendations are taken into account when designing medication procedures and policies (Figure 3). Two units (1.5% of the respondents) said they did not take the recommendations into account because they disagreed with the ICS recommendations, while seven units (5.3% respondents) did not know of the existence of the ICS recommendations. The remaining five units (3.8%) do not use the ICS recommendations because of reasons listed in Table 2. The type of critical care unit is not significantly related to acceptance and application of the recommendations (χ2 = 6.373, p = 0.896).
Acceptance of ICS recommendations on standard medication infusion concentrations in Critical Care Areas. Other reasons for not applying ICS recommendations.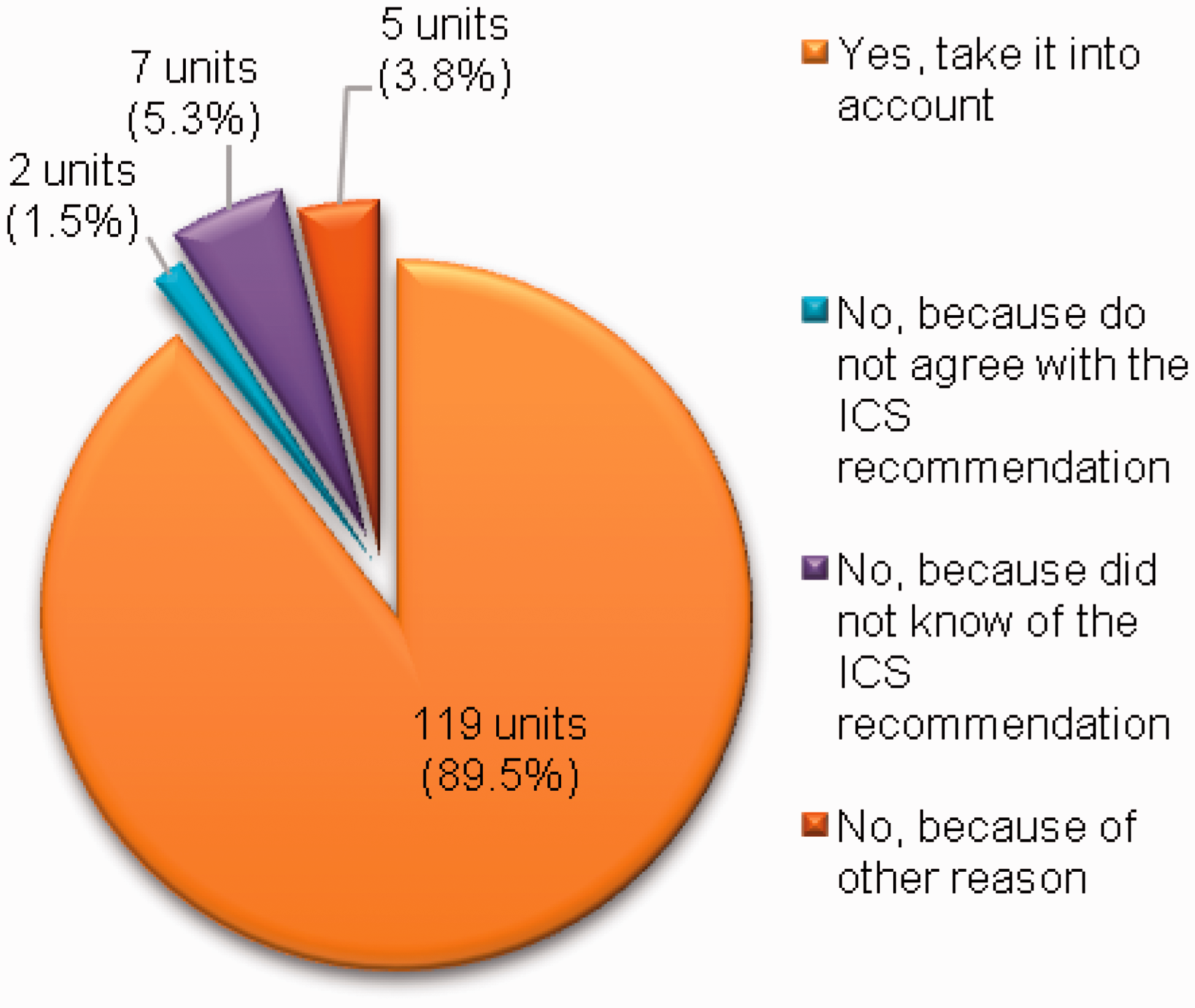
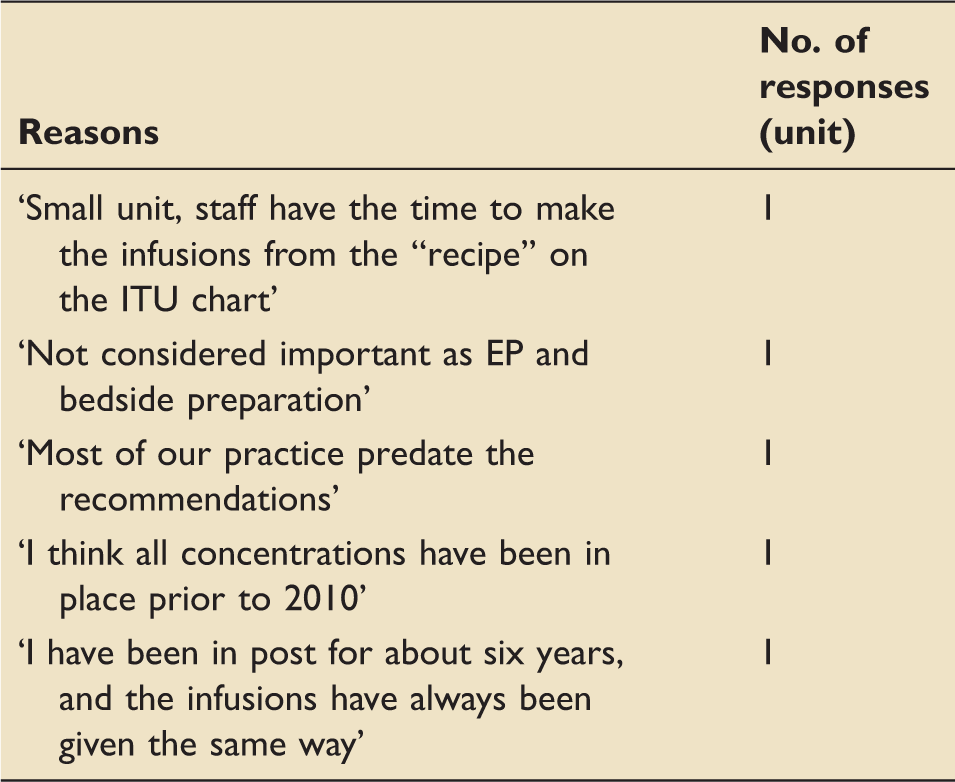
Figure 4 shows the acceptance of the ICS recommendations for each of the 16 medications, excluding the units that do not use the respective medications in their practice. Respondents using at least one of the recommended concentrations were categorised as ‘using the ICS recommendations’. Respondents were categorised as ‘not using the ICS recommendations’ if they do not use any of the recommended concentrations in their practice.
Level of application of ICS recommended medication infusion concentrations in critical care units that use the medications. *Units that use any of the ICS recommended infusion concentrations. **Units that do not use any of the ICS recommended infusion concentrations.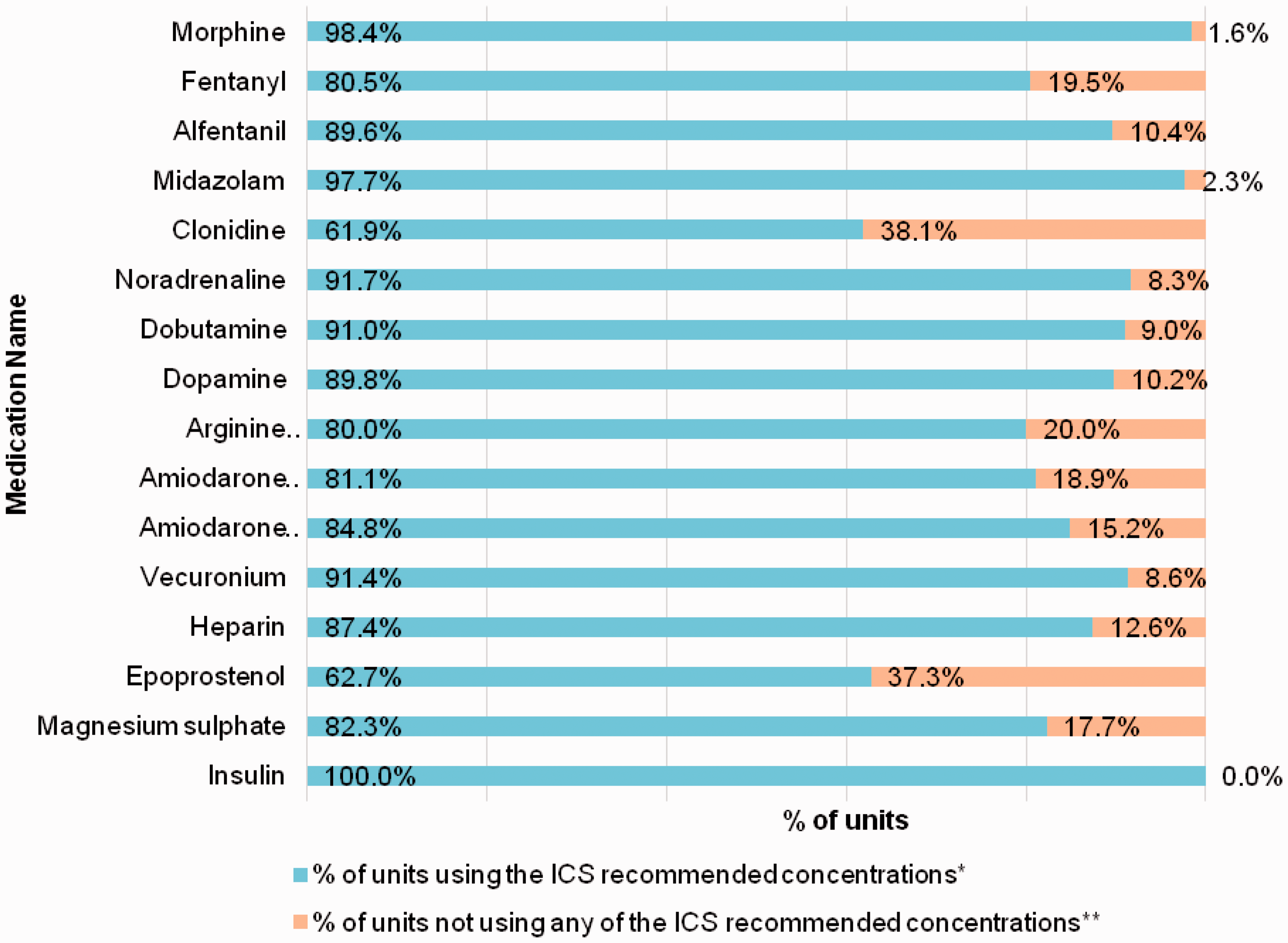
Infusion concentrations for medications that have not yet been standardised.
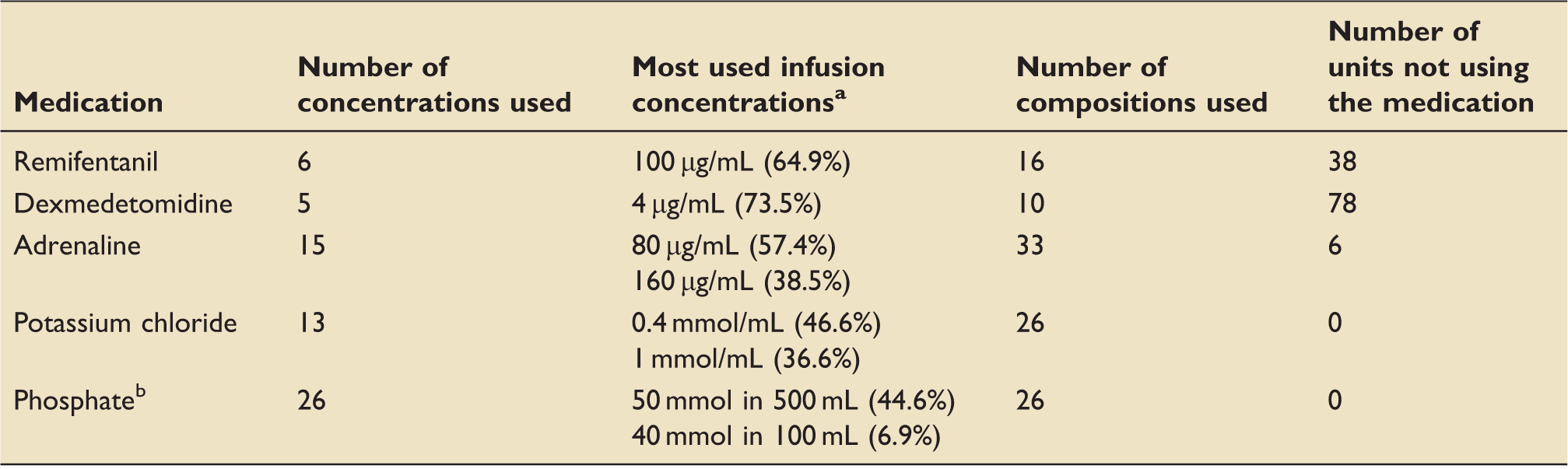
Counted from units that using the medications.
Stated in composition of infusion.
For phosphate infusion, the most commonly used phosphate preparation is Polyfusor® (58%), followed by Addiphos® (18%) and potassium phosphate (9%).
When the respondents were asked about the ways of obtaining the desired concentrations for each medication, most medication infusions in critical care areas were prepared by on-ward preparation, except for morphine (34.3% of the surveyed units prepared it from bought in ready-to-use preparation).
Discussion
A good acceptance to the ICS recommendations on standard infusion medication has been shown. A good acceptance of the ICS recommendations has been shown. The reasons for not taking the ICS recommendations into account are disagreement, ignorance, and lack of will to change. Interestingly, even though some say they are not taking the ICS recommendations into account, one unit is using the same infusion concentrations as the recommended ones, for 10 out of the 16 medications.
Policies and procedures in place predating the recommendations, if required have been changed.
The most encouraging result is the high level of acceptance and application of standard infusion concentrations for morphine, fentanyl, alfentanil, midazolam, heparin, and insulin, which are high-risk medications commonly involved with IV adverse drug events in critical care areas.1,5 This finding indicates that the majority of UK critical care units have made efforts to minimise medication errors for high-risk medications, with the help of standardised infusion concentrations derived originally from the 70% acceptance used in the second survey of 2010 which resulted in ICS recommendations that the 16 drug concentrations fitting this parameter should be adopted nationally.
Using the 70% acceptance as general agreement, remifentanil infusion concentrations cannot be standardised yet. Meanwhile for dexmedetomidine, even though the most commonly used infusion concentration is used by 73.5% respondents, the medication itself is only used by less than half of the respondents; however, as such it does fit the predetermined criteria for standardisation.
Previous national infusion surveys9,11 showed a divided opinion for adrenaline, phosphate, and potassium chloride infusion concentrations. The National Injectable Guide suggested the concentrations of 80 µg/mL, 160 µg/mL, and the concentration of 320 µg/mL for adrenaline IV infusions. The results for adrenaline showed that concentrations of 80 µg/mL are used by 57.4% respondents, concentrations of 160 µg/mL by 38.5% respondents, and 320 µg/mL 19.7% respondents. Some units are using more than one of the mentioned concentrations. Alternatively, other units are using other concentrations alongside the recommended ones such as 80 µg/mL with 40 µg/mL. Standardisation here is potentially feasible.
Meanwhile for phosphate infusion, the concentrations seem to be determined by the type of phosphate preparations used in each unit. For example, the units that used Phosphate Polyfusor® are typically using the infusion composition of 50 mmol in 500 mL, 50 mmol in 50 mL, and/or 100 mmol in 500 mL. In units that prefer to use Addiphos®, 40 mmol phosphate in 100 mL is the commonest infusion concentrations. Addiphos® comes as 40 mmol phosphate in 20 mL vial, requiring dilution.
This figure supports the previous survey, 11 where 19% of the respondents chose to continue using Phosphate Polyfusor®, while the others supported the proposed concentration of 20 mmol phosphate in either 50 mL or 100 mL. Five years on as the situation has not changed, could separate standard infusions be designed for the two different commercially available preparations?
Most respondents using potassium chloride chose 0.4 mmol/mL (46.6%) and/or 1 mmol/mL (36.6%). The difference from five years ago balancing out as previously 66% of the participants supported the use of 0.4 mmol/mL concentration (20 mmol in 50 mL, 40 mmol in 100 mL), while 29% preferred 2 mmol per mL. 11 Is it safe in these circumstances to suggest two infusion concentrations?
From the results of this study infusions for almost all of the 16 medications are prepared by on-ward preparation. This means reconstitution or dilution ward staff before administration is required. A study found that even with standardised infusion concentrations deviation between the intended and actual infusion concentrations for amiodarone or noradrenaline is greater if the infusions are prepared at the patient’s bedside. 12 This dose variation may lead to adverse drug events.1,13,14
Once again the need for ready-to-use or ready-to-administer preparations has been highlighted. To date, morphine, fentanyl, midazolam, dobutamine, heparin sodium, magnesium sulphate, and insulin are available in the recommended concentrations as ready-to-use vials or ampoules. Noradrenaline is available from NHS Special-order Manufacturers.
It is hoped that a sub-optimal response rate in this study does not affect the representative value of the results. 15 The eclectic nature of the respondent critical care areas should help counterbalance this.
Further work on improvement in error reduction and reduction in adverse events after introduction of standardisation would greatly help in support of these audits.
Conclusion
Five years after its introduction, the ICS recommendations on standard infusion medication concentrations in critical care areas have been applied and accepted by most critical care units across the UK.
We should endeavour to encourage more trusts to adopt these standards as the introduction of ready-to-use preparations will reduce patient morbidity and mortality and cost. The Carter report of February 2016 16 has recommended Electronic Prescribing and Medicines Administration systems, which will rely on standardisation to achieve a cost saving. Standardisation also reducing cost related to variance and procurement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.