
Abstract
Objective
The aim of this study was to determine the frequency and type of drug therapy problems (DTPs) in older institutionalized adults.
Method
We conducted a cross-sectional observational study from February to June 2016 at a 150-bed public nursing home in Croatia, where comprehensive medication management (CMM) services were provided. A rational decision-making process, referred to as the Pharmacotherapy Workup method, was used to classify DTPs.
Results
Data were prospectively collected from 73 residents, among which 71% were age 75 years or older. The median number of prescribed medications per patient was 7 (2–16) and polypharmacy (> 4) was recorded for 54 (74.0%) patients. A total 313 DTPs were identified, with an average of 4.3 ± 2 DTPs per patient. The most frequent DTP was needing additional drug therapy (n = 118; 37.7%), followed by adverse drug reaction (n = 55; 17.6%). Lactulose (14.4%), tramadol (6.7%), and potassium (6.4%) were the medications most frequently related to DTPs.
Conclusion
The high prevalence of DTPs identified among older institutionalized adults strongly suggests the need to incorporate new pharmacist-led CMM services within existing institutional care facilities, to improve the care provided to nursing home residents.
Keywords
Introduction
The absolute and proportionate increases in older populations has become an outstanding demographic trend and a serious public health issue globally, with manifold social consequences that require early planning of optimal care for older adults. According to data from World Population Prospects: the 2019 Revision, 1 in 6 people will be over age 65 years (16%) by 2050, up from 1 in 11 (9%) in 2019. 1 Currently, Europe has the highest prevalence of older adults (25%), with similar trends prevailing in Croatia. The Croatian share of the older adult population now exceeds approximately 18%, with projections of 22.6% by 2031, thus representing a rapidly aging nation. 2
Older people frequently do not receive appropriate treatment, and older residents of nursing homes are particularly at risk for poor quality of medical care. 3 Age-related changes in pharmacodynamic and pharmacokinetic properties and multiple comorbidities accompanied by polypharmacy render older people more susceptible to experiencing drug therapy problems (DTPs),4–6 making the optimization of drug use an extremely challenging and complex process. 7 DTPs occur on a daily basis and add substantial costs to the health care system, 8 exceeding the amount spent on the medications themselves.9–11 Hence, this population would benefit most from the detection and prevention of DTPs.
Most nursing homes still function under the traditional quality assurance model, merely monitoring specific aspects of care retrospectively and addressing problems on an individual basis rather than on a systems level. Therefore, within existing institutional care facilities (i.e., nursing homes), a well-established approach using comprehensive medication management (CMM) services 12 should be incorporated to improve the care of this extremely vulnerable population. Since being adopted by the United States federal government in 2003, 13 CMM has expanded and is accepted and provided around the world at different levels in all patient care practices. 8 Various studies have shown that a medication management specialist (i.e., pharmacist) can play an important role in clinical practice by working toward the prevention, identification, and resolution of DTPs.14–21
To the best of our knowledge, only a few studies to date have assessed the DTP profile of older adults placed in nursing homes22,23 using pharmaceutical care practice as a theoretical framework, as proposed by Cipolle et al. 12 Additionally, data are lacking on both prescribing patterns and DTP profiles among older people living in Croatian nursing homes. In the face of these issues, identification of DTPs is an important strategy for planning and establishing improvements in health services, as this represents the first step in CMM among older adults. Therefore, we aimed to determine the frequency and type of DTPs among institutionalized older adults, to inform the evidence base with regard to prescribing patterns and subsequently improve the care of older people.
Participants and methods
Study design and setting
The study protocol was approved by the Home’s Ethics Committee and the Ethics Committee of the University of Zagreb Faculty of Pharmacy and Biochemistry. This research followed the guidelines of the Declaration of Helsinki and Tokyo.
We conducted a cross-sectional observational study from February to June 2016 in Sv. Kamilo de Lellis nursing home in Vrbovec, Zagreb County, Croatia. Caritas House for older adults Sv. Kamilo de Lellis operates within Bjelovarsko - Krizevacka District and accommodates older people in need of assistance owing to changes in their health condition, as well as mobile and immobile individuals with Alzheimer’s disease and other forms of dementia living in separate residential units with 24-hour professional care. A team comprising one general practitioner (GP), 20 professional nurses, five social workers, and a psychiatrist ensures the well-being of 148 residents accommodated in 79 rooms.
Study participants
This study was conducted among 73 older nursing home residents, and patients were eligible for inclusion if the following criteria were met: a) age 65 years or more, b) taking two or more drugs as a part of their therapy, c) at least one chronic condition recorded in the nursing home service’s patient record, and d) signed a written informed consent for study participation.
Exclusion criteria were assessed in an interview and included terminal illness, and severe dementia making informed consent impossible (as evaluated by the community pharmacist–researcher in charge of their medication management).
Data collection
Two clinical faculty members, one community pharmacist–researcher and two pharmacy students comprised the team that identified patients fulfilling the inclusion criteria. Residents’ data were retrieved in a careful review of resident’s admission documents, medical records, and through interviewing the residents and nursing home’s medical staff. Supplementary information was obtained from the GP when necessary. To determine to what extent each patient’s drug-related needs were being met, standard demographic characteristics, current and previous medical diagnoses, current medication records for all medical conditions (prescription and over-the-counter medications), and medication history including history of drug allergies and adverse drug reactions (ADRs), history of relevant medication use and social drug use (caffeine, nicotine, alcohol) were collected for each resident by the community pharmacist–researcher. Additionally, hematological and biochemical analyses of blood/serum, renal function, and blood pressure were compiled for each resident, when available.
Anatomical Therapeutic Chemical (ATC) Classification codes were used to analyze the prescribed therapy. The principal diagnosis and comorbidities were coded according to the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10), 2016.
Drug therapy problems (DTPs)
Identification of DTPs was based on information about the patients’ medications, obtained by a community pharmacist–researcher at the initial consultation (before the initiation of CMM services). A community pharmacist–researcher and two pharmacy students collected the data simultaneously; thus, no inter-rater agreement was needed. All disagreements or uncertainties were presented to an expert panel consisting of a clinical pharmacist and an academic pharmacist, who addressed disagreements and reached a consensus regarding the identification of DTPs. A DTP was defined as any undesirable event experienced by a patient that involves, or is suspected to involve, drug therapy and that interferes with achieving the desired goals of therapy and requires professional judgment to resolve.24,25
The Pharmacotherapy Workup method proposed by Cipolle et al. 12 was used for the classification of DTPs. This process represents cognitive work taking place in the mind of the practitioner and is used to identify, resolve, and prevent DTPs, establish therapeutic goals, select interventions, and evaluate outcomes.
Identifying a DTP requires the practitioner to establish an association between the patient’s medical condition and the patient’s pharmacotherapy, with the purpose of determining whether the patient’s drug-related needs are being met. Patient’s drug-related needs were always assessed in the same systematic order: first, the appropriateness of therapy, followed by the safety and effectiveness of the drug regimen, and last, adherence.
To ensure adequate data collection, we used a standardized data collection form modified from the Pharmacotherapy Workup notes, 12 which consisted of demographics, current and past clinical conditions and medications, dosage regimen and duration of treatment, vital signs (e.g., blood pressure, heart rate), and renal function, when available, as well as a DTP list.
Statistical analyses
Descriptive analysis of study population characteristics included frequency distributions of the qualitative variables, and measures of central tendency and dispersion for the quantitative variables. Pearson’s chi-squared test was used to assess univariate association between the independent variables and the number of identified DTPs. Statistical evaluation of the data was performed using IBM SPSS statistical software version 24 (IBM Corp., Armonk, NY, USA). Comparisons were conducted with the significance level set at p < 0.05.
Results
Data were prospectively collected from 73 older nursing home residents, among which 55 (24.7%) were women (Table 1). The median age (overall range) was 80 (57–96) years, with 71% of residents in the age group 75 years or older. The median number of medical conditions per patient was 5 (1–9); 56.2% of patients had 5 or more conditions, and 9.6% had 8 or more conditions. Diseases of the circulatory system were the most prevalent pathology (31.9%), with hypertension the most common presenting condition (15.3%), followed by mental and behavioral disorders (24.0%), diseases of the musculoskeletal system and connective tissue (16.3%), diseases of the digestive system (11.8%), and endocrine, nutritional and metabolic diseases (10.2%). Detailed information of the study population is provided in Table 1 and includes sociodemographic and clinical data. Table 2 lists the 10 most frequent medical conditions requiring drug therapy. The 10 most frequently encountered medical indications for drug therapy represented two-thirds (67.7%) of all indications for drug therapy. Essential hypertension, gastritis and duodenitis, and polyosteoarthritis accounted for the largest proportions of patients who had uncontrolled disease: 65.8%, 39.7% and 37.0%, respectively.
Characteristics of the study sample.

ATC, Anatomical Therapeutic Chemical; ICD-10, International Statistical Classification of Diseases and Related Health Problems, 10th Revision.
Most frequent medical conditions requiring drug therapy and most frequently used medications.
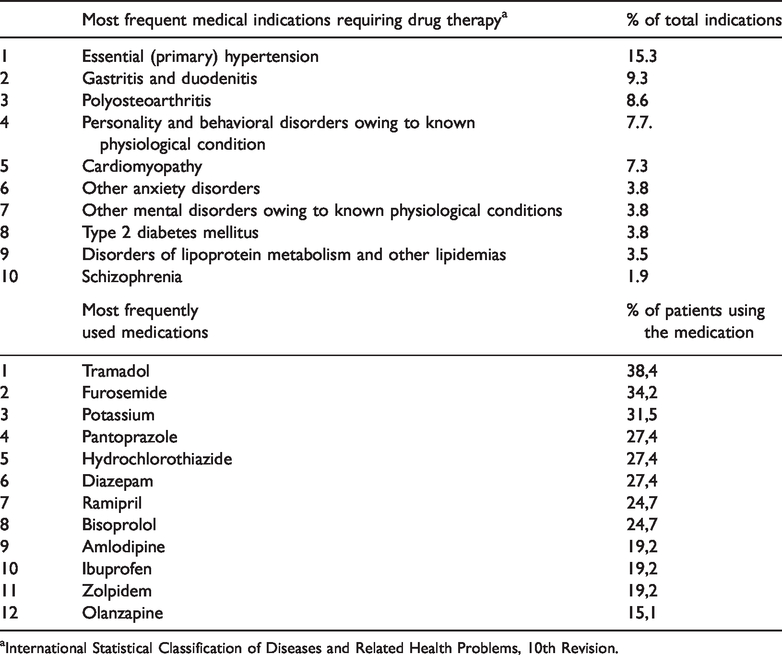
aInternational Statistical Classification of Diseases and Related Health Problems, 10th Revision.
The median number (overall range) of prescribed medications was 7 (2–16); 31.5% of residents received 8 to 16 drugs, and polypharmacy (more than four prescribed medications) was recorded for 54 (74.0%) residents. Table 2 describes the pharmacological agents most commonly used by participants to manage their medical conditions.
A total of 313 DTPs were identified during our initial visits, with an average of 4.3 DTPs per patient. Almost all patients (98.6%) had at least one DTP and 43.8% had five or more DTPs, of which 4.1% had nine or more DTPs. The most frequent DTP identified in these patients was the need for additional drug therapy (n = 118; 37.7%) to prevent or treat a medical condition, with an untreated condition being the most common cause (Table 3). Most of these DTPs involved patients who required lactulose for constipation, aspirin for secondary prevention post myocardial infarction (MI), oral vitamin D supplementation, and angiotensin-converting enzyme (ACE) inhibitors and beta-blockers for treating heart failure. The second and the third most common DTP categories were adverse drug reaction (ADR; n = 55; 17.6%) and dosage too low (n = 43; 13.7%), respectively (Table 3). The most common causes of DTPs leading to an ADR and subtherapeutic dosage were undesirable effects (n = 36; 11.5%) and an ineffective dose (n = 21; 6.7%), respectively. A complete list of DTPs along with their causes together with the most common examples are presented in Table 3. The list of the most frequent examples of DTPs in the table is not exhaustive but it contains the most representative examples.
List of drug therapy problems, with the most common examples.

ACE, angiotensin-converting enzyme; AF, atrial fibrillation; CVI, cerebrovascular insult; HF, heart failure; ISMN, isosorbide mononitrate; MI, myocardial infarction; NSAIDs, nonsteroidal anti-inflammatory drugs; PPIs, proton pump inhibitors; SSRI, selective serotonin reuptake inhibitor; T2DM, type 2 diabetes mellitus.
The predominant DTPs associated with medications are presented in Table 4. Lactulose was the most frequently involved medicine for the DTP needing additional drug therapy (n = 45; 14.4%) owing to untreated constipation; this was followed by tramadol as the most commonly involved medicine for ADRs (n = 17; 5.4%) causing constipation. Potassium was the next often involved medicine for a dosage that was too low (n = 16; 5.1%) owing to incorrect administration. Fewer than 1% of DTPs (0.6%) were owing to nonadherence, with the main cause being that the patient could not afford the medication (aspirin for secondary prevention of an MI) or the copayments required to obtain the prescription (trimetazidine as an add-on therapy in treating stable angina pectoris). A significant correlation was found between the proportion of identified DTPs with the number of comorbidities (p < 0.001) and the number of medications (p < 0.001). DTPs and their associated medical conditions occurring with the highest frequency are listed in Table 5.
Most common drug therapy problems associated with medications.

ACE, angiotensin-converting enzyme.
Most common drug therapy problems associated with medical conditions.

MI, myocardial infarction; CVI, cerebrovascular insult.
Discussion
This study represents one of the first published research investigations to assess the DTP profiles of older nursing home residents 23 using pharmaceutical care practice as a theoretical framework, as proposed by Cipolle et al. 12 To the best of our knowledge, this is the first study in both Croatia and Southeastern Europe to evaluate the incidence and types of DTP among older adults placed in a nursing home using the aforementioned classification, thereby contributing to the evidence base regarding medication use in this extremely vulnerable group. Systematic identification of DTPs is the first step in providing CMM services, which together with resolution and prevention of DTPs, represents the central value of all medication management services. In cases involving patients with numerous, complex, and difficult therapeutic regimens, such as older residents of nursing homes, it is of utmost important to have a clearly defined patient care process. The three steps in the patient care process entail assessment, care plan development, and follow-up evaluation. The purpose of assessment is to identify DTPs. Hence, CMM cannot be provided without clear DTP identification.
The multiple medical conditions and polymedication observed in our study sample constitute important risk factors for DTP occurrence. In our research population, participants rarely experienced a single medical condition, and more than half had five or more medical conditions. Given an average five or more medications a day taken by older people, as found in a recent review of inappropriate medication use among older patients, 26 the average number of medications used per older person in our study was fairly high (seven medications) and similar to that detected by other authors.23,27–33 As indicated in other published research,34–36 these characteristics are common within the population of institutionalized older adults.
Our findings revealed a relatively high level of DTPs. More than four DTPs per patient were identified at the initial assessment of nursing home residents. This finding is similar to the rates of drug-related issues reported in previous studies.12,37 Moreover, it is likely that the number of DTPs would have been even higher had we considered an average number of follow-up visits, as analyzed in previous research.12,36,37 DTPs can occur at any time during a patient’s course of treatment and can be identified during any follow-up evaluation. It must be stated that the complete absence of pharmacists employed in or cooperating with nursing home institutions must have contributed to such a high level of unfounded drug use.
In congruence with previous research that used the same methodology,12,20,38 the most commonly encountered DTP categories in our study were the need for additional drug therapies to manage patients’ medical conditions, as well as patients receiving inadequate dosages of medication to provide therapeutic benefit. These results suggest that the main DTP in our population of older adults was the underutilization of effective medications, as previously reported by Oliveira et al. 36 and other authors. 20 This finding is contrary to the presumption that a key role of pharmacists is to reduce the number of medications and medication costs for patients. When a pharmaceutical care practitioner collaborates closely with a physician and a patient, an increase in medication use usually occurs. Additionally, to ensure that each patient is receiving an efficacious drug product, a sufficient dosage must be provided, as subtherapeutic dosages might expose patients to the risk of ADRs without achieving positive clinical outcomes. Nevertheless, that patients are receiving inadequate dosages of medications to provide a therapeutic benefit is frequently encountered in practice, mainly owing to clinicians’ fear of producing an ADR as a consequence of high dosages or simply owing to clinical inertia in cases where up-titration is needed.
ADRs occurred more frequently in our study than previously reported,12,20,36 which could be partly explained by the type of study participants, namely, older institutionalized adults simultaneously using multiple medicines with drug interactions. In addition, use of an unsafe drug product for a certain patient (e.g., thiazides in a patient with gout) or drugs causing an undesirable effect (e.g., tramadol causing constipation, benzodiazepines leading to falls) further contributed to a high rate of ADRs in this sensitive age group. Noncompliance was the least frequently encountered DTP, most probably because study participants were institutionalized and provided with their therapy by nurses who administer medications to patients. Hence, patient adherence was very high, probably owing to nursing services responsible for packing and administering medication, as previously reported. 39
In line with other reported experiences among institutionalized older people,35,38 those medical conditions associated most frequently with a DTP involved diseases of the circulatory system, constipation, and mental and behavioral disorders, accentuating the conditions seen by pharmacists on a regular basis.
Although pharmacists’ effectiveness at reducing the number of DTPs in nursing home settings has long been noted,40–43 it seems that there is room for improvement; particularly, the pharmacist’s current role, if any, is largely to supply medicines to care homes. 44 Currently, in the vast majority of countries worldwide, the role of pharmacists in nursing homes is lacking or is insufficient and incomplete, at best. This must change in a such way that pharmacists have an embedded role in care homes, as a part of a multidisciplinary team, with overall responsibility and accountability for medicines and their use. 45 Previous research has shown that the best way to address this issue is through the introduction of CMM services within those primary care clinic structures that are most in need of pharmacist services.46–49 A nursing home is an ideal setting for initiating such a service considering the high proportion of DTPs in older polymedicated patients and the relative accessibility of establishing this service in such a setting. Compared with other settings, all residents of nursing homes are situated in a single location and are receiving care from one or several GPs, thus simplifying the collaboration that needs to be established between health care professionals.
Several limitations in this study must be acknowledged. The study sample was relatively small, thereby adversely influencing the generalizability of the results. However, the studied nursing home is the only one of its kind in Croatia to have addressed a research topic about which so little is reported. In addition, certain laboratory tests such as potassium and creatinine levels, as well as vital signs (e.g., blood pressure, heart rate) were unavailable in patients’ medical charts, which might have influenced the DTP analysis. In addition, data on how long patients were using a certain medicine (e.g., tramadol, benzodiazepines, ACE-inhibitors) was lacking, rendering DTP identification insufficient. Pharmacist access to medical records is necessary for optimal service; therefore, a lack of access to patient data made DTP identification incomplete, and it is very likely that the prevalence of DTP might be underestimated. Finally, this study yielded data on DTP profiles without providing data on interventions to resolve DTPs or on clinical outcomes of the included residents. Hence, it is pivotal to design and carry out studies providing complete CMM services, as systematic identification of DTPs along with resolution and prevention of DTPs represent the central value of all medication management services.
Conclusion
The high prevalence of DTPs identified among older institutionalized adults strongly suggests the need to incorporate medication management services within existing institutional care facilities, to improve the care provided to nursing home residents. The nature of DTPs associated with the most frequently encountered medical conditions points to areas in which further pharmacist training is required, to develop knowledge and skills needed for the delivery of services essential to the welfare of care home residents.
Footnotes
Acknowledgements
The authors would like to thank Jelena Kurija for her help in collecting the data in this research study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.