
Abstract
Introduction
Medication errors, including infusion prescription errors are a major public health concern, especially in paediatric patients. There is some evidence that electronic or web-based calculators could minimise these errors.
Aims
To evaluate the impact of an electronic infusion calculator on the frequency of infusion errors in the Paediatric Critical Care Unit of The Royal London Hospital, London, United Kingdom.
Method
We devised an electronic infusion calculator that calculates the appropriate concentration, rate and dose for the selected medication based on the recorded weight and age of the child and then prints into a valid prescription chart. Electronic infusion calculator was implemented from April 2015 in Paediatric Critical Care Unit. A prospective study, five months before and five months after implementation of electronic infusion calculator, was conducted. Data on the following variables were collected onto a proforma: medication dose, infusion rate, volume, concentration, diluent, legibility, and missing or incorrect patient details.
Results
A total of 132 handwritten prescriptions were reviewed prior to electronic infusion calculator implementation and 119 electronic infusion calculator prescriptions were reviewed after electronic infusion calculator implementation. Handwritten prescriptions had higher error rate (32.6%) as compared to electronic infusion calculator prescriptions (<1%) with a p < 0.001. Electronic infusion calculator prescriptions had no errors on dose, volume and rate calculation as compared to handwritten prescriptions, hence warranting very few pharmacy interventions.
Conclusions
Use of electronic infusion calculator for infusion prescription significantly reduced the total number of infusion prescribing errors in Paediatric Critical Care Unit and has enabled more efficient use of medical and pharmacy time resources.
Introduction
Prescription errors are a serious and recognised safety and health problem globally in intensive care units including paediatric intensive care.1,2 Such errors may occur at any stage of prescribing, dispensing or administration of the medication3,4 although most of the errors have been documented at the prescribing stage.1,5,6 Errors at the prescribing stage can be even higher in an intensive care due to the nature of work and clinical setting. Among the type of prescriptions, continuous infusion prescriptions are more error prone since they require constant alterations and dose titrations.5,7,8 Prescribing is even more challenging in children as more complex dosing determinations are required based on age, weight, body surface area, and different drug tolerances compared to adults.3–5 Several interventions and approaches to reduce and prevent such medication errors have been tried and include computerised physician order entry (CPOE), 2 electronic prescribing (EP), 3 computer software, 9 web-based calculator 5 and educational programmes.10,11 All these computerised systems and calculators have been successfully used and are known to reduce infusion prescription errors drastically.2,5,7,9 The purpose of this study was to compare the incidence of paediatric continuous infusion prescription errors before and after the implementation of an electronic infusion calculator devised locally at The Royal London hospital, London.
Methods
Study site
The study was based in a six-bedded Paediatric Critical Care Unit (PCCU) at The Royal London Hospital, London, United Kingdom. Approval was obtained from the Joint Prescribing Group of The Barts Health NHS Trust prior to implementation of an electronic infusion calculator (EIC).
System description
We devised an EIC that calculates the appropriate concentration, rate and dose for the selected medication based on the recorded weight and age of the child. A choice of electronic formats for the calculator was considered and Microsoft Excel was chosen for its simplicity and flexibility. The options of medications to be included, dilution method, and dosage range were agreed between PCCU consultants, pharmacy and nursing staff. Formulas for calculating each medication infusion was created and validated for different age and weight ranges by two PCCU-trained pharmacists, accounting for capping at certain age and weight bands as appropriate for the medication. These were programmed into the spreadsheet for automatic calculation using inputted age and weight for the selected medications.
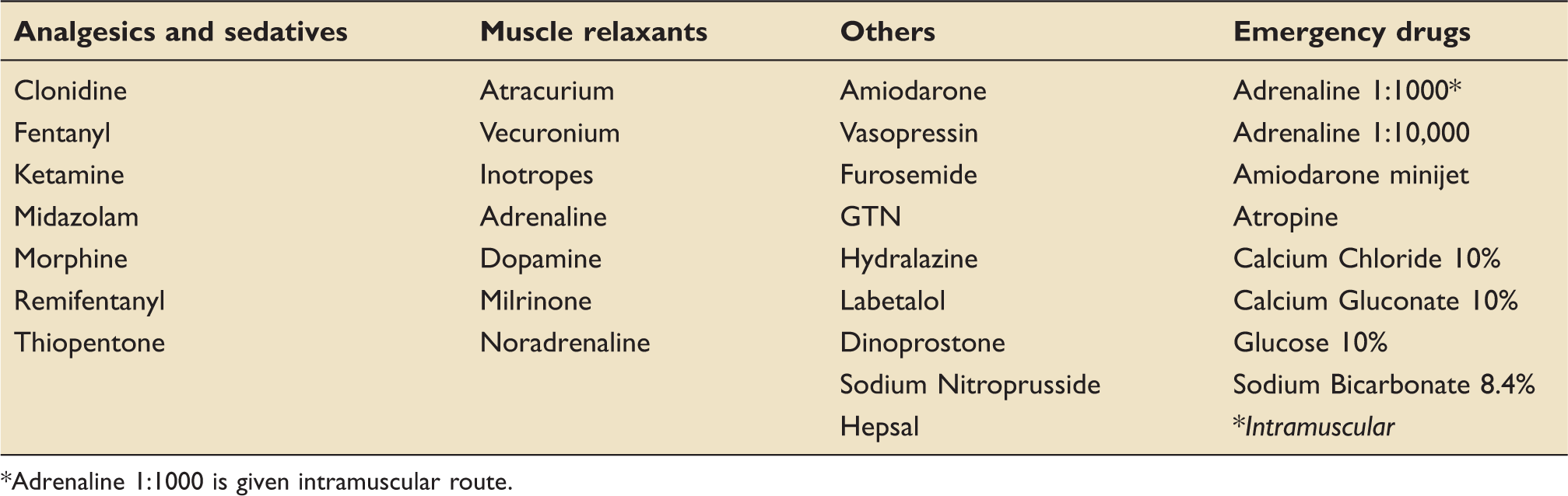
A validation and trial period of four weeks preceded implementation. Discrepancies in the formulas identified during this period were amended. Figure 1 explains the prescribing process. The prescriber is required to complete all the mandatory sections (hospital number, name, date of birth, weight, allergy information). By clicking the “submit” box, a pick list of 37 commonly prescribed medications in our PCCU is displayed. Most of the commonly used medicines (Table 1) in PCCU are preconfigured in the system. As emergency medicines are administered frequently in PCCU, we included some of the emergency resuscitation medications in the EIC although they are not administered as continuous infusions. Once all the mandatory patient demographics are entered and the required medications are selected, the EIC calculates the concentration, rate and the dose of selected medications accordingly. It then prints into a valid NHS prescription chart, accepted by the Barts Health NHS Trust. The prescriber is then required to sign the prescription. All prescribers were formally briefed and trained for using EIC by the PCCU pharmacists. Due to its simple and self-explanatory process, EIC was rapidly accepted by all in PCCU.
Prescribing process using electronic infusion calculator. (a) Main page of the EIC, (b) patient demographics, (c) List of medications and (d) a valid prescription. List of medications currently available on the electronic infusion calculator. *Adrenaline 1:1000 is given intramuscular route.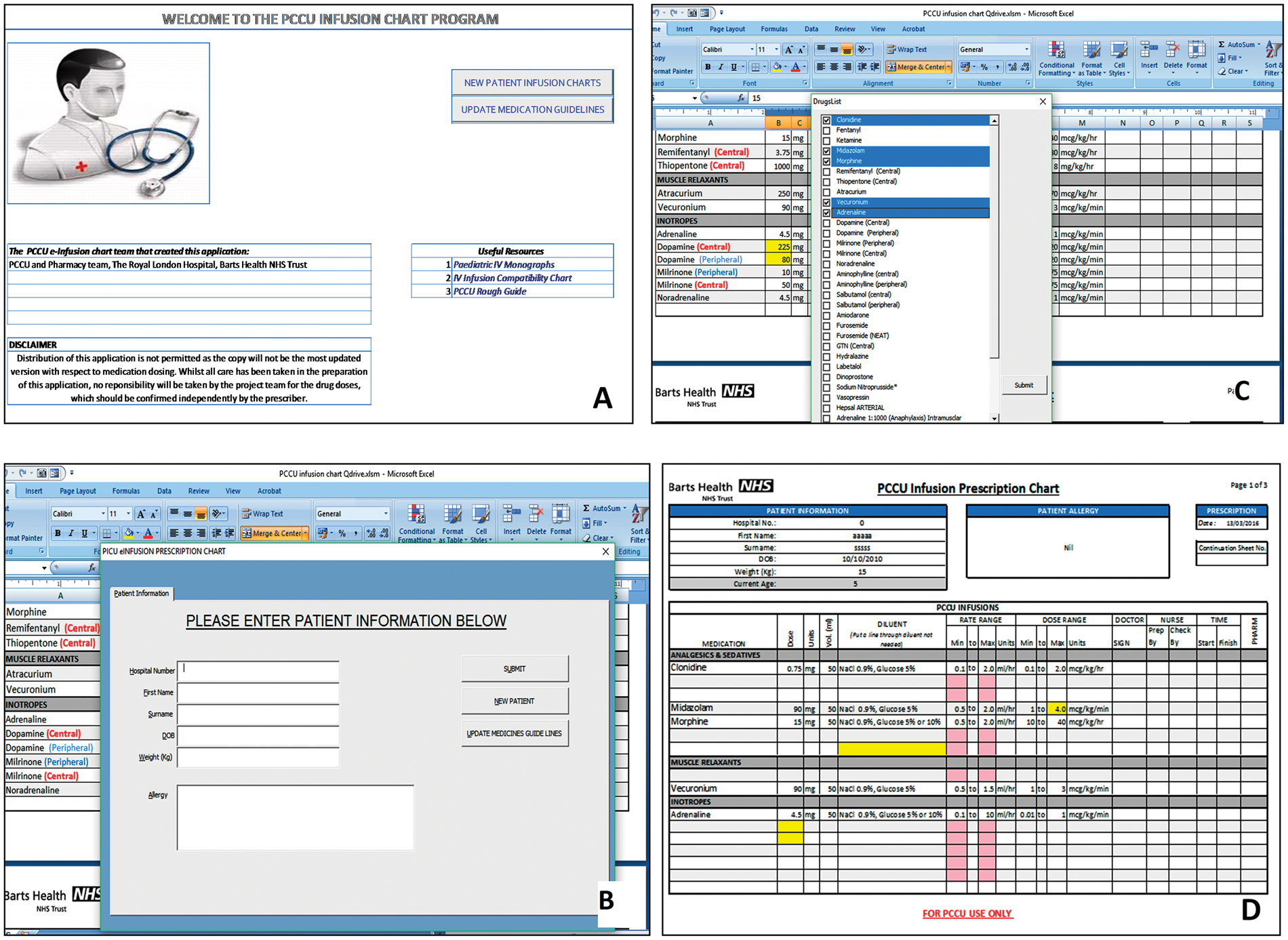
Data collection
Data were collected prospectively for two time intervals, November 2014 to March 2015 and April 2015 to August 2015. EIC was implemented from April 2015 in PCCU. During the first phase, handwritten prescriptions were evaluated and EIC prescriptions were assessed during the second phase. For the handwritten prescription, the prescriber was required to write the appropriate drug along with the dose, rate and concentration after manual calculations and then undersign it. Prescribing with EIC has been explained above. No handwritten prescriptions were generated during the second five-month period. Data on the following variables were collected onto a proforma for both the time intervals: medication dose, infusion rate, volume, concentration, diluent, legibility, and missing or incorrect patient demographics and details. Prescriptions were reviewed daily by the ward pharmacists as part of their routine duties. Data on the above variables were then collected by a named doctor and pharmacist for the study and entered into a password-protected excel sheet. All patient details were completely anonymised. Statistical analysis was performed by SPSS.
Results
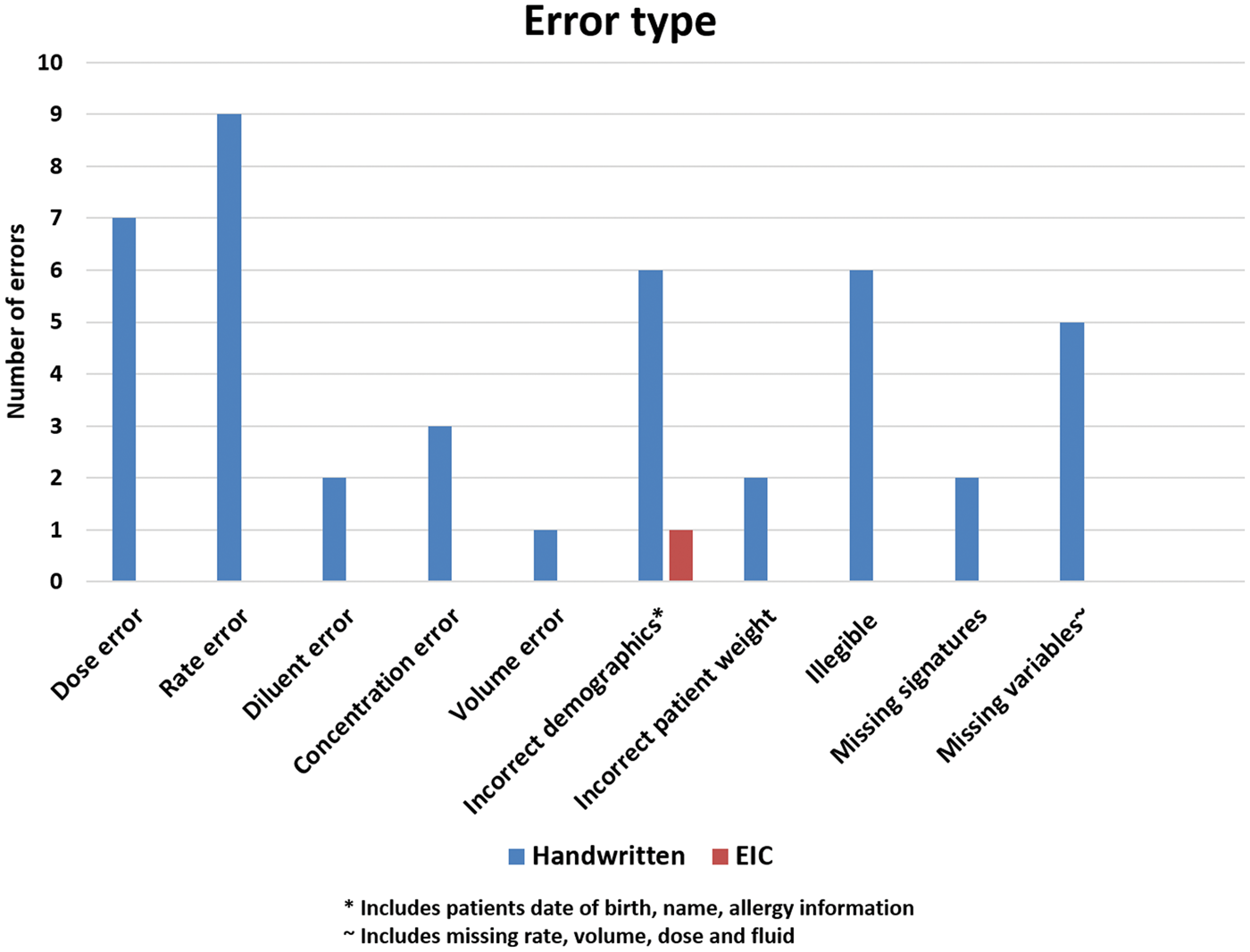
A total of 132 handwritten prescriptions were reviewed prior to EIC implementation and 119 EIC prescriptions were reviewed after EIC implementation. Handwritten prescriptions had higher error rate of 32.6% (43/132) as compared to EIC prescriptions < 1% (1/119) with a p < 0.001 (Figure 2). Figure 3 illustrates a breakdown of type of errors. Most commonly occurring errors with handwritten prescriptions were wrong rate 20.9% (9/43), wrong dose 16.2% (7/43) followed by incorrect patient demographics 13.9% (6/43) and illegible prescriptions 13.9% (6/43).
Number of continuous infusion errors pre EIC (handwritten) and post EIC implementation. Categorisation and distribution of errors according to error type.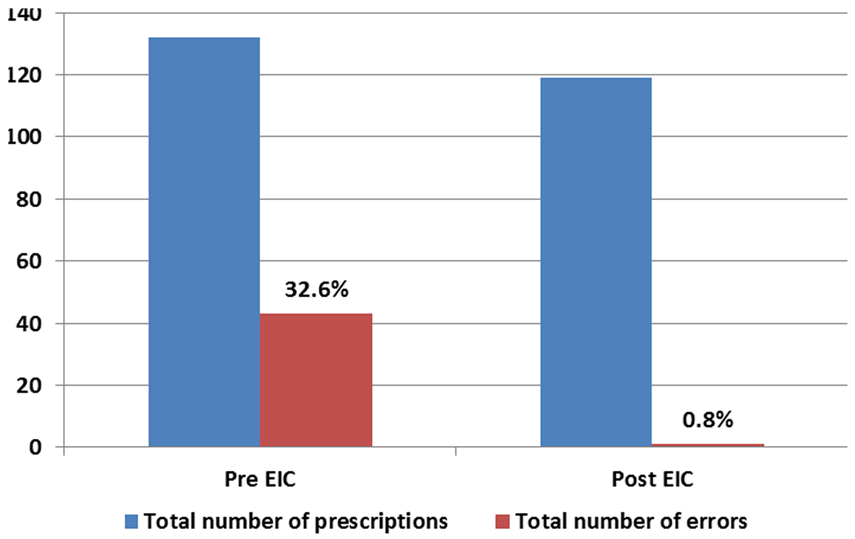
EIC prescriptions had no errors on dose, volume and rate calculation as compared to handwritten prescriptions, hence warranting few pharmacy interventions. The only error on EIC prescription was due to incorrect data input.
Discussion
EIC was started as an initiative to reduce the infusion prescription errors in PCCU. A previous study on prescription errors, conducted in our unit (local unit audit, 2014), revealed an extremely high error rate (35%) among continuous infusion prescription including most serious errors like an accidental 10 times drug dose plus errors related to concentration, omissions, legibility and calculations. As a result, we wanted to use a system that could reduce or potentially eliminate continuous infusion prescription errors. Many computerised systems have been used effectively in intensive care units and have shown promise.2,5,7,9 But, most of these commercially available prescribing systems are expensive, network-dependent and includes different prescription types in one system (general prescriptions, parenteral nutrition calculator and infusion prescriptions).2,5,9,12 We therefore developed a cost-effective drug calculator particularly focusing on continuous infusion prescriptions. EIC automatically calculates the dose, concentration and rate of infusion based on the prescribers’ input of patient details and medicine, thus eliminating majority of error types. All patient demographics including age, date of birth, weight and allergy status are mandatory requirements. EIC has an inbuilt interlink between the age and weight of the child, thus enabling a safety check on the dose of the medications. EIC thus provides more accurate prescriptions than handwritten prescriptions in terms of completeness and legibility. It also enabled efficient use of prescriber time since the time taken to prescribe using EIC was less than the time taken to prescribe manually, as described by the prescribers and nurses in a user satisfaction survey. The user satisfaction survey conducted during the trial period also revealed that PCCU staffs were more satisfied with EIC rather than handwritten prescriptions, due to ease of use and completeness of the prescriptions. This overwhelming acceptance by PCCU staff led to successful implementation of EIC during the second phase of the study, when all the infusion prescriptions were EIC generated.
Further advantages of EIC include minimal effort to set up, low cost compared to established commercial systems,2,7,9 the ability to update to newer versions, addition of new drugs to the preconfigured list and non-Internet dependence. As EIC is saved on the local PCCU drive of paediatric critical care network, it can be assessed for prescribing from any computer in the hospital. Such an EIC can be without doubt incorporated in most of the departments where continuous infusion prescriptions or intravenous infusions are more commonly and often used, like the high dependency units, emergency departments and intensive care units at district general hospitals.
Our study has established that by using EIC, infusion errors are drastically reduced to an extent that in EIC prescriptions the only error detected was due to incorrect data input. Potential adverse infusion error due to wrong patient demographics (particularly date of birth) is the only limiting factor of our EIC. Unfortunately, eliminating such errors is beyond the scope of EIC, since patient demographics are entered manually by the prescriber into the system. Therefore, utmost accuracy is still required while entering patient details.
Conclusion
After the inception of EIC for continuous infusion prescription, total number of infusion errors in paediatric critical care unit significantly reduced. It has also enabled more efficient use of medical and pharmacy time resources as reported from the user satisfaction survey. Our study, though small, provides data to support the use of such electronic infusion calculator for continuous infusion prescription in paediatric intensive care setting.
Footnotes
Acknowledgement
We are thankful to the paediatric pharmacy team and paediatric critical care team of The Royal London Hospital, London for their support and contribution.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.