
Abstract
Introduction
Patients in the intensive care unit are vulnerable to myocardial injury from a variety of causes, both ischaemic and non-ischaemic. It is challenging for ICU clinicians to apply the conventional guidance concerning diagnosis and treatment. We conducted this review to examine the evidence concerning diagnosis and treatment of myocardial infarction in the ICU.
Methods
A systematic review was performed to identify relevant studies.
Results
19 studies concerning use of ECG, cardiac enzymes, echocardiography and angiography were identified. 4 studies considered treatment of myocardial infarction.
Conclusions
Regular 12 lead ECG or 12 lead ECG monitoring is more sensitive than 2 lead monitoring, regular measurement of cardiac enzymes is more sensitive than when provoked by symptoms. Coronary angiography rarely identifies treatable lesions, without regional wall motion abnormality on echocardiography. Evidence relating to treatment was limited. A potential strategy to diagnose myocardial infarctions in the ICU is proposed.
Introduction
Third universal definition of myocardial infarction. 1
MI is classified into five types: Type 1 – MI with intraluminal thrombus; Type 2 – where a condition other than coronary artery disease (such as arrhythmia or anaemia) contributes to an imbalance between myocardial oxygen supply and demand; Type 3 where MI results in death before biomarker values are available. Type 4 and 5 relate to PCI and CABG.
Cardiac troponins (cTn) are regulatory proteins of the cardiac contractile mechanism, with subtypes cTnT and cTnI. 2 Creatine kinase isoenzymes are phosphate carriers in myocytes with the –MB isoenzyme being most abundant in the heart. 3 However, as noted in the 3rd Universal definition, owing to low specificity of CK isoenzymes, cTn is the preferred biomarker. 1 A cTn increase greater than the 99th percentile of the upper limit of normal is defined as positive and the value will depend on the assay used. 1
Non-ischaemic conditions may also cause a cTn rise and should be classed more broadly as myocardial injury. Examples include: purely non-ischaemic conditions such as cardiac contusions, rhabdomyolysis, myocarditis or cardiotoxic agents and pre-dominantly non-ischaemic conditions such as heart failure, renal failure, arrhythmia and pulmonary embolism. 1 Therefore any cTn increase should be interpreted considering the pre-test probability of myocardial ischaemia.
Myocardial injury is a common event within an intensive care unit (ICU).4,5 In systematic review of 20 studies of patients who had a cTn measured during their ICU stay, a median frequency of cTn elevation of 43% was reported, which was associated with increased risk of death. 6 A review from 2012 summarised evidence showing that an elevation in cTn in ICU patients is associated with an increase in mortality. 7
The distinction between myocardial injury and MI presents a challenge in ICU and the universal definition authors acknowledge that the development of ischaemia may not be apparent in critically ill patients. 1 Patients in ICU may not be able to complain of ischaemic symptoms; electrocardiogram (ECG) changes may not be observed; the rise in biomarkers may be due to non-ischaemic causes; a regional wall motion abnormality (RWMA) on echocardiography or angiography changes will only be identified in the case of either routine surveillance, or the investigation being prompted by clinical suspicion. In the absence of chest pain, factors such as hypotension, arrhythmias or evidence of heart failure may be the prompts to search for evidence of ischaemia.8,9
The authors of the universal definition note that the relationship between underlying coronary artery disease and MI is less secure in the ICU setting than a general population, and that careful clinical judgment is required to evaluate the coronary circulation. 10 For example, in one study, two intensivists were retrospectively asked to determine the most likely cause of cTn increase in 49 ICU patients. MI was suggested in 26; type 1 MI in 10, and type 2 MI in 16. The remaining 23 were judged to have had other non-ischaemic causes of cTn elevation. 11
The significance of MI within ICU was demonstrated by a review of post-mortem examinations performed on ICU patients which showed the most frequently missed diagnosis likely to impact outcome was MI. 12
ESC guidelines for treatment of NSTEMI.
In addition, decisions regarding treatment in critically ill patients are complicated by conditions which increase the potential of iatrogenic harm from treatment: recent surgery and the presence of coagulopathy and thrombocytopenia may limit use of anti-platelets (both pre and post coronary intervention); cardiovascular instability may preclude the use of nitrates and beta blockade.
The difficulty in making treatment decisions in this patient group is further demonstrated by the variety of intensivists practice when managing patients with elevated cTn, but without symptoms of MI or ECG changes. 19 To our knowledge, there are no guidelines regarding the management of MI in ICU.
In view of the above uncertainties, we performed a systematic review of the available literature considering two questions:
When the clinician suspects an ICU patient is undergoing an MI, what diagnostic tests are most helpful? When an ICU patient is diagnosed with MI, what treatment is most appropriate?
Methods
Search terms used.
The search was limited to those studies in English and concerning patients over 16 years old. This identified 2811 potential papers (Figure 1). The titles were reviewed by one author (IC) according to the following criteria:
Was the study population relevant to our question? Did it concern adult patients? Did the study concern MI acquired within an ICU? Did the study consider the diagnosis or treatment of MI? Flow chart of papers reviewed.
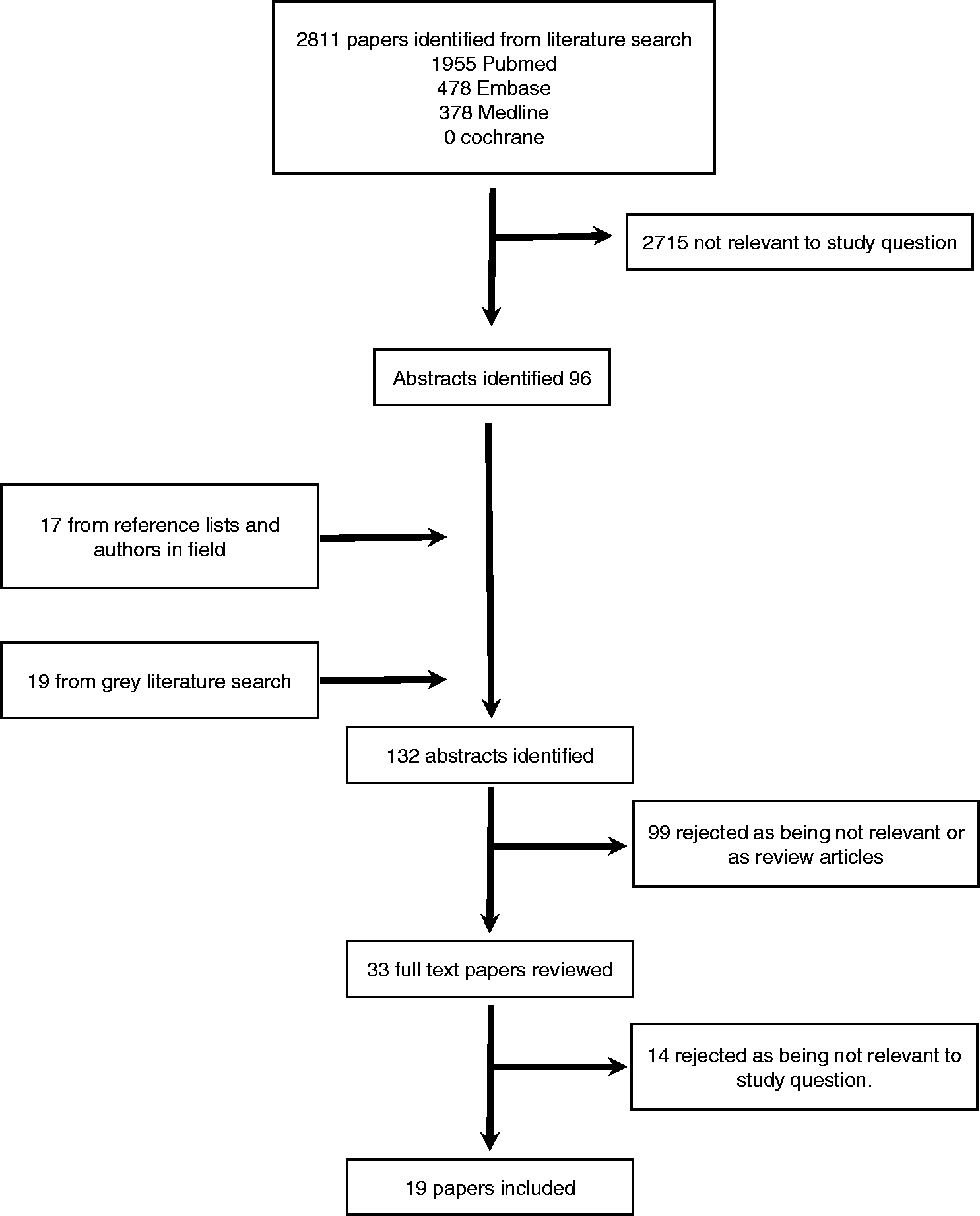
After elimination of duplicates, a total of 96 papers were identified. We reviewed references and contacted prominent authors regarding recently published articles or those pending publication, identifying a further 17 abstracts.
A grey literature search for unpublished abstracts and conference proceedings using an internet search engine identified 19 abstracts.
These abstracts were reviewed by IC and TM. The criteria above were reapplied, and review articles, letters and comments excluded. In cases of disagreement, the full text paper was included; 33 papers were identified.
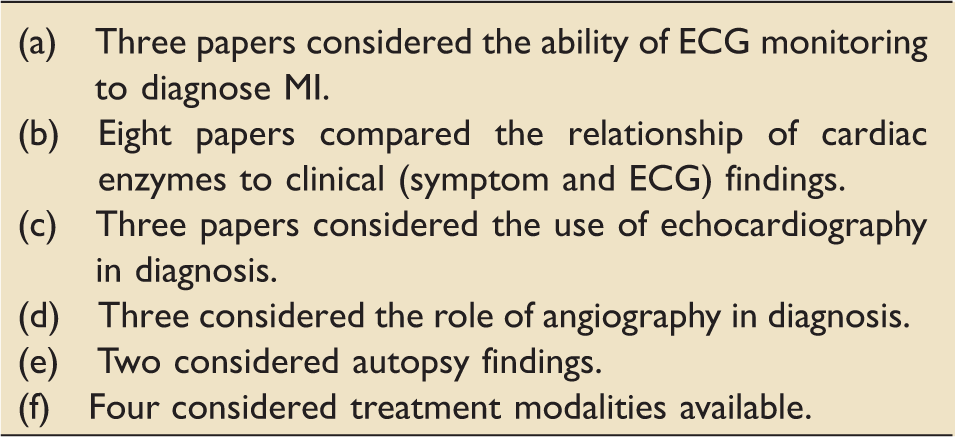
Categories of papers chosen.
Discussion
Summary of included studies

The diagnostic studies considered presented evidence for a range of different tests; ECG monitoring with a variety of lead combinations, interval 12-lead ECGs; echocardiography; functional cardiac studies and cardiac enzyme measurements.
In the summary below, the pertinent conclusions are highlighted.
Evidence concerning the use of ECG
12-lead ECGs have been shown to have several limitations.
There was limited agreement on ECG findings on separate readings by the same doctor and between experienced doctors interpreting ECGs, but agreement increased when further clinical information, such as results of cTn assays were presented. 20 This suggests that the role of single ECG in diagnosis is undermined by the difficulty in agreement between clinicians. Automated ECG interpretation software of 12-lead ECGs showed a significant false positive rate. 21
Two-lead ECG monitoring with daily 12-lead ECGs was shown to have a low sensitivity of 12%, but a specificity of 98% for detecting the first episode of ischaemia when compared to 2 minutely 12-lead ECG in post-operative vascular patients. 22
Evidence concerning the use of cardiac enzymes
Studies in this group can be divided into two categories:
1. Those that compared incidence of cTn rise with incidence of ECG abnormality and clinical findings.23–25 In these studies, patients were identified who had a cTn rise which was not detected in routine care and who lacked other features of myocardial ischaemia. a. The situation is a non-ischaemic myocardial injury. b. There has been a MI (Type 1 or 2), but either the tests lacked sensitivity, or were not performed at an appropriate time. 2. Those that compared standard ICU surveillance with a form of ‘enhanced surveillance’. Consequently, it was possible to reach additional diagnoses of MI. This was achieved by the following methods: Continuous 12-lead ECG surveillance. This also showed the rarity of clinical symptoms as only 2 out of 37 episodes were associated with clinical symptoms.
8
Continuous 12-lead ECG surveillance and daily cTn measurement.
26
Serial repetition of 12-lead ECG and cTn.
27
Focused clinical assessment and daily cTn measurement.
9
If an enzyme rise is documented, without corroboration from other factors, then there are two diagnostic possibilities:
The results of these studies are shown in more detail in Table 1 and may reflect the lack of sensitivity of routine surveillance, or that the elevation of cTn reflected non-ischaemic myocardial injury. In the context of the first group of studies, it is likely that a significant proportion of the patients had ‘missed’ myocardial ischaemia, where the ECG was not recorded at an appropriate time.
In a separate style of study, Lim et al. 28 noted how the agreement between four experienced intensivists in reaching a diagnosis of MI when presented with ECG and cTn details varied extensively from slight to substantial, according to the which two of the doctors were compared.
Papers considering the use of echocardiography or angiography in diagnosis
Three of the papers in this category29–31 identified that the greater the increase in the serum cTn, the more likely there were to be echocardiographic abnormalities detected.
In the ver Elst study of patients with septic shock, an association was shown between the magnitude of elevation of cTn elevation and evidence of left ventricular (LV) dysfunction on trans-oesophageal echocardiography. Additionally, cTnI was found to be more sensitive than cTnT; seven subjects who were cTnI positive remained cTnT negative. 29
Relos showed an increased incidence of ECG change, echocardiographic abnormality, and mortality with greater cTnI increase in 869 post-surgical patients. 30
Ko et al. 31 identified 56 patients who had had an angiogram performed for investigation of coronary artery disease while on ICU; 18 out of 56 patients were identified as having coronary artery disease, of whom 9 required interventional treatment. Angiographic abnormalities requiring treatment were observed in only 9 out of 56 studies performed and were more common if patients had RWMA on transthoracic echocardiography.
In the Ruiz Bailen study, 574 patients who had an echocardiogram performed in ICU were identified; 33 had myocardial dysfunction, primarily in the basal and apical segments. These were not associated with other evidence of ischaemia and the changes all normalized during follow-up interval echocardiography. Seven of the patients proceeded to angiography, which was normal in each case. 32
Ammann et al. 33 studied 58 patients admitted to a medical ICU with sepsis, SIRS, or other severe disease (mean Simplified Acute Physiology Score II of 42); 32 had raised cTn (I or T isoform) but only two had evidence of coronary arterial disease; 23 were shown to have no coronary arterial disease (by either dobutamine stress echocardiography, coronary angiography or, in six cases by autopsy), seven were untested, and two had evidence of coronary artery disease on autopsy. Ethical considerations had not permitted the investigators to submit every patient to coronary angiography.
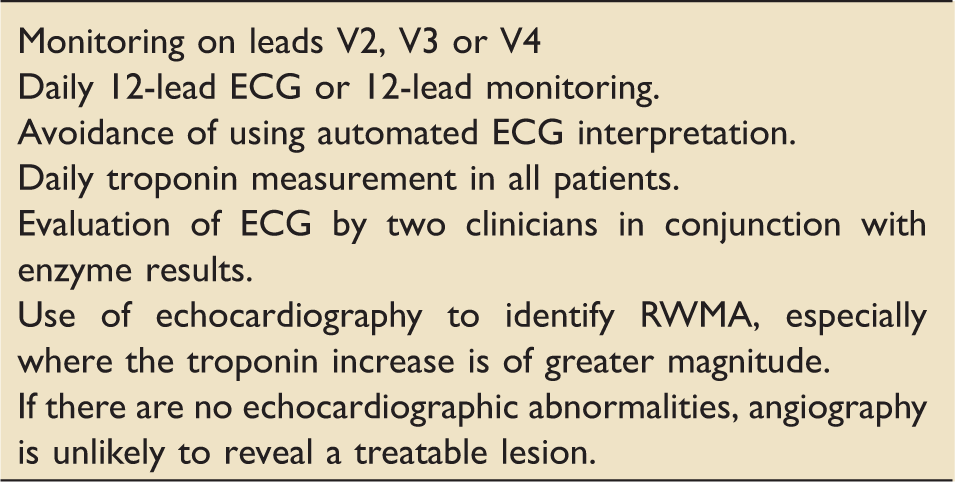
It may be concluded that the utility of angiography for patients who have had a diagnosis of MI while on ICU is questionable, with a relatively limited probability of identifying any lesions which are remedial to treatment. This should be considered in the context of the practical difficulties in arranging such tests for ICU inpatients, as well the possibility of the abnormalities which prompted angiography normalising over time.
Autopsy findings
These studies demonstrate the discrepancy between clinical suspicion of MI and pathological diagnoses.
Berlot et al. 34 investigated the 600 autopsies performed on ICU patients in a single unit over a 10-year period. Evidence of MI was found in 75 cases; 25 patients had evidence of coronary artery disease and 50 did not and may therefore be concluded to represent type 2 MI. Of the 75 cases, 55 had been investigated clinically, but a diagnosis of MI was clinically confirmed in only 11. Additionally, during the time period, eight patients were clinically suspected of having suffered an MI, but no post-mortem evidence was identified.
In the ver Elst study of 46 patients with septic shock, autopsies were performed on 12 patients, seven of whom were cTn positive. One cTn positive patient had evidence of MI, while a cTn negative patient had an LV free wall rupture. In the 10 other post-mortems performed, there was no evidence of MI or inflammatory infiltrate. 29
Treatment modalities available
A subgroup analysis of the TRICC study showed no difference in mortality of 357 patients with cardiovascular disease, or the subset of 257 patients with acute or chronic coronary arterial disease, when randomised to either a restrictive Hb (7–9 g/dl) or liberal (10–12 g/dl) transfusion strategy. This was the only randomised study included. 35
There was no other convincing evidence identified regarding treatments for patients having suffered MI on ICU.
The Lim 2006 cohort identified seven patients who had an MI during the ICU stay. Patients were managed according to the judgement of the treating physician. No difference in mortality was noted according to whether the patient had received anti-platelet, anti-coagulant treatment, β blockade or nitrates. However, the use of vasopressors and inotropes was an independent predictor of ICU mortality. 36
A separate cohort study by the same author identified that patients identified as having an MI were more likely to receive conventional treatment for MI. However, there was no difference in mortality between those who were identified with ischaemic disease and those who were not. 27
Conversely, Relos’s retrospective cohort of 869 patients considered the impact of the treatment used in patients suspected of having had an MI. They found that where cTn rise was greatest, the use of B blockers and aspirin were associated with decreased hospital mortality. 30
Conclusion
In reviewing the evidence regarding diagnosis of MI in intensive care, it is clear that a different strategy is required than in patients presenting with chest pain. Patients rarely present with symptoms of ischaemia8,9,31 and when tests only are used in response to symptoms, signs or clinical suspicion, diagnosis of MI is frequently missed.8,9,26,27
Single 12-lead ECGs were shown to have a limited role owing to lack of sensitivity and lack of agreement both between different interpreters, and the same interpreter on different occasions. Regular 12-lead ECGs have improved sensitivity to 2-lead monitoring.
It is possible to increase the sensitivity of regular monitoring for detecting MI used in many ICUs (e.g. clinical signs, 2-lead ECG monitoring, 12-lead ECG on demand and cardiac enzymes as prompted by suspicion of ischaemia) by several methods: continuous 12-lead ECG surveillance; regular 12-lead ECG and regular cTn measurement unprompted by clinical suspicion.
Echocardiographic abnormalities were more common the greater the increase in cTn, and in one study were associated with increased likelihood of angiographic abnormality. However, lesions requiring interventional treatment remained unusual.
Suggested strategy for monitoring and diagnosis of MI.
Regarding treatment, when a diagnosis of MI is made in an ICU patient, it remains unclear whether the conventional anti-platelet, anti-anginal and interventional treatments (see Box 2) are appropriate or beneficial. In cohort studies, there has been no evidence of reduced mortality in patients who were treated with conventional anti-ischaemic regimes compared to those who were not. However, we were not able to identify any randomised trials conducted in this area, and it remains an area for future research opportunities. No study in intensive care has considered the relative benefit of treatment in type 1 or 2 MI. Early liaison with cardiologists and admitting teams with careful consideration of likelihood of test results representing myocardial ischaemia and risks and benefits of treatment to the individual patient will remain critical in this area.
Footnotes
Acknowledgements
The authors would like to acknowledge: Eva Thackeray, librarian at Royal Preston Hospital; and Colette King, librarian at Central Manchester Foundation Trust for their assistance with the search strategies.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.