
Abstract
In many centres, height is used as a determinant for calculating predicted body weight. This predicted body weight is then multiplied to generate the desired tidal volume. The approach exhibits some mathematical effects: (1) any errors in height measurement are multiplied by 5.5 when generating the tidal volume (assuming 6 ml/kg); (2) any errors in height measurement have a greater impact on shorter patients. The aim of this study was to: (1) establish the current practice of setting a tidal volume in England; (2) assess the implications of inaccurate height measurements on tidal volume settings using the most common practice; (3) identify the most accurate and precise method of determining height to aid accurate application of a lung protective strategy. The six extra corporeal membrane oxygenation centres in the UK, and the 34 intensive cares with the highest admission figures were identified from the intensive care national audit and research centre database. Most frequent practice was to use of a 1-m tape on the supine patient on admission. Inaccuracies in height estimation using a 1-m tape resulted in a standard deviation of 23 ml and a spread of over 120 ml tidal volume in individual patients.There are a number of methods of estimating height in a supine patient but the most accurate appeared to be simply using a 2-m tape.
Introduction
Lung protective ventilation strategies using tidal volumes (TV) of 6–8 ml/kg are widely accepted as a standard of care for patients with acute respiratory distress syndrome (ARDS). 1 Early application of a low tidal volume strategy prior to ARDS is also gaining evidence.2–4
Significant research and resources have gone in to determining the optimal millilitres per kilogram for ventilation of high-risk patients. However, estimating the height of a supine patient is in itself a source of error. There is limited work in accurately determining the predicted body weight (PBW) of supine patients, and much of it in nutritional journals.
The formula used by the ARDS-net investigators is shown below:


Taking the example for males, bringing the 50 into the brackets and adding an ‘error’:


For Tidal Volumes of ‘6 ml/kg’


Two facts become clear:
Any error (E) in height is multiplied by 5.5 when converting to 6 ml/kg tidal volume. Any error (E) is fractional to (height (cm) – 97.5 (males) or 103 (females)), i.e. mathematically there is a much bigger error margin in shorter patients.
This formula is commonly used in critical care in the UK to determine PBW. The application of this formula to different ethnic groups is also relatively unknown.
We undertook a survey of those units with the highest admission records on the intensive care national audit and research centre (ICNARC) database and UK specialist respiratory centres with the aim of establishing current UK practice. We then tested the reproducibility of the most common practice. The final step was to find a simple solution to estimating height that would reduce human error as much as possible.
Methods
The Peninsula Ethics Committee advised that formal ethical approval was unnecessary for our project. Patient dignity and privacy were taken into account and infection control protocols adhered to in the collection of our data.
Establishing current UK practice
We surveyed six Specialist Respiratory Centres and the 34 intensive care units (ICU) on the ICNARC database with the highest admission figures. We telephoned the nurses station at each unit and asked to speak to a doctor or nurse who had responsibility for inputting admission ventilator settings for new Level 3 patients. We asked:
How they decided upon the tidal volume for each patient. If this involved multiplication of PBW, how they determined the PBW.
Assessing the precision of 1-m tapes (the most common UK practice)
Twenty regular ICU nurses were asked to each measure 20 patients using their normal technique and our standard disposable 1-m tapes. They were blinded to each other’s measurements. The spread of observations was assessed. Gold standard height is traditionally taken as standing height. Due to the supine nature of our Level 3 patients, the gold standard was unavailable.
Alternative techniques to estimated PBW.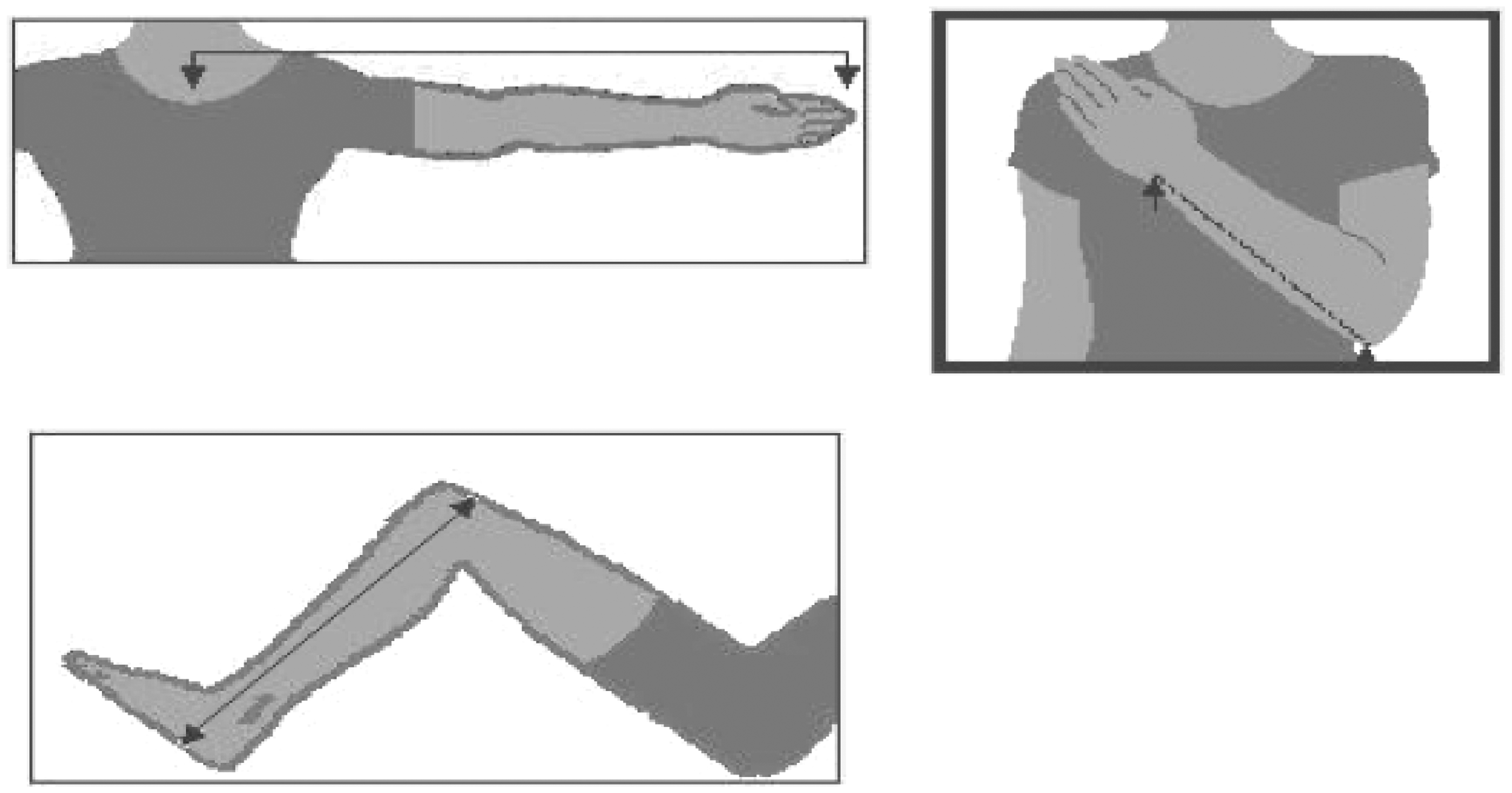
Assessing the accuracy and precision of different estimates of height in supine healthy volunteers compared with the gold standard of standing height
Four techniques were chosen (see Figure 1): Olecranon to ulnar styloid, knee to sole distance, sternal notch to tip of middle finger, and 1-m tape.5,6 Each technique has its own formula for conversion to estimate height; 21 members of our regular nursing staff measured 8 healthy volunteers using a 1-m tape and the three alternative methods. Individuals were blinded to each other’s measurements. The eight volunteers were then measured using standing height as a gold standard against which to compare the other techniques.
Assessing the accuracy and precision of 2-m tapes in patients
Twenty regular ICU nurses were asked to each measure 20 patients using their normal technique and disposable 2-m tapes, they were blinded to each other’s measurements. Standing height was also taken at a recent pre-assessment clinic.
Results
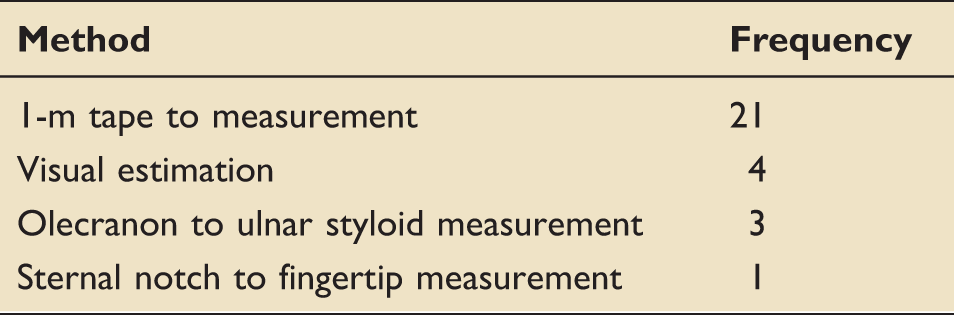
Method of calculating predicted body weight.
Initial ventilator settings.
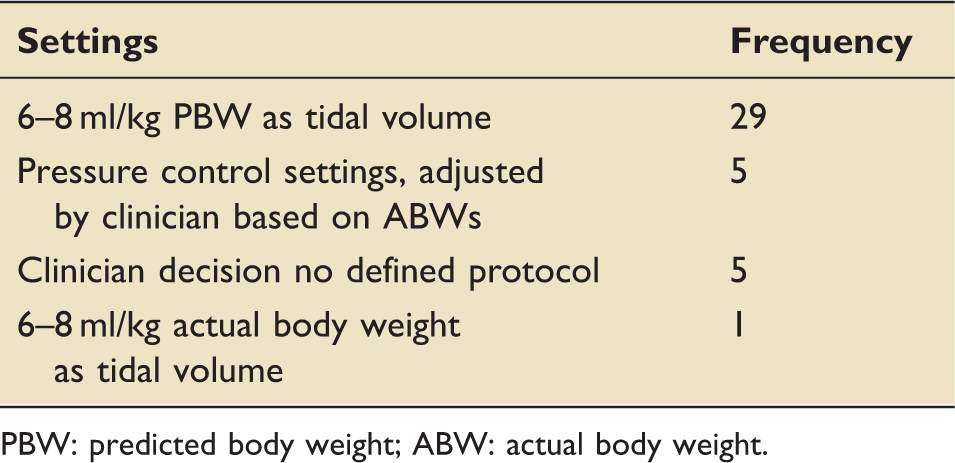
PBW: predicted body weight; ABW: actual body weight.
The majority of intensive cares in the UK use 6–8 ml per kg of PBW which they estimate using the ARDS-net formula and patient’s height. The commonest method of measuring height was using a 1-m tape. This was the technique used in the UK specialist respiratory centres that provide extra corporeal membrane oxygenation (ECMO). Some centres use alternative measuring techniques, while individuals surveyed in other units report the use of pressure control, visual estimates of height, or having no defined protocols for initial mechanical ventilation settings.
Tidal volume variation around the mean when the height is estimated with a 1-m tape
The spread of height/tidal volume measurements reveal a surprisingly high degree of variability, see Figure 2. The standard deviation was 23 ml with a number of patients having inter-observer difference of 70–100 ml.
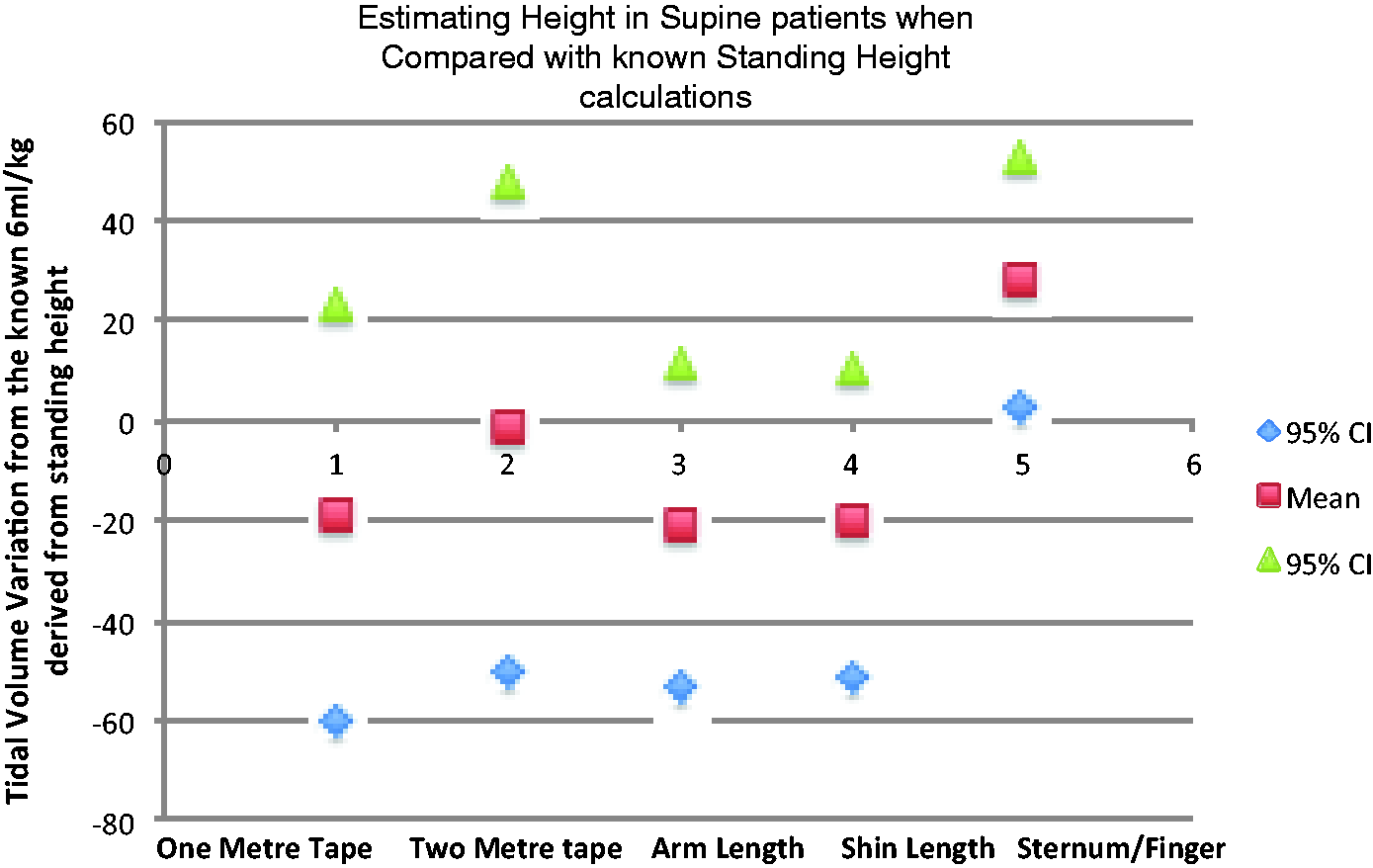
Comparison of gold standard standing height to estimates generated by a 1-m tape, 2-m tape, shin to sole, olecranon to ulnar styloid, and sternum to finger tips in healthy volunteers
When the different measures for estimating the height are used, there is little to choose between the different techniques, although the sternum to fingertip measure seems an outlier, see Figure 3. When a 2-m tape is used, the normal distribution settles around the standing height exactly, but again there is a distribution to the measurements. Of note, this normal distribution relates to measurements at the bedside, while the other measures were performed on healthy co-operative volunteers.
Graph demonstrating the magnitude of deviation from the mean TV of when using each nurses measurements. Column height represents frequency and shows a normal distribution around the mean with 95% confidence intervals approaching ± 50 ml. Comparison of mean TV generated from four techniques with confidence intervals.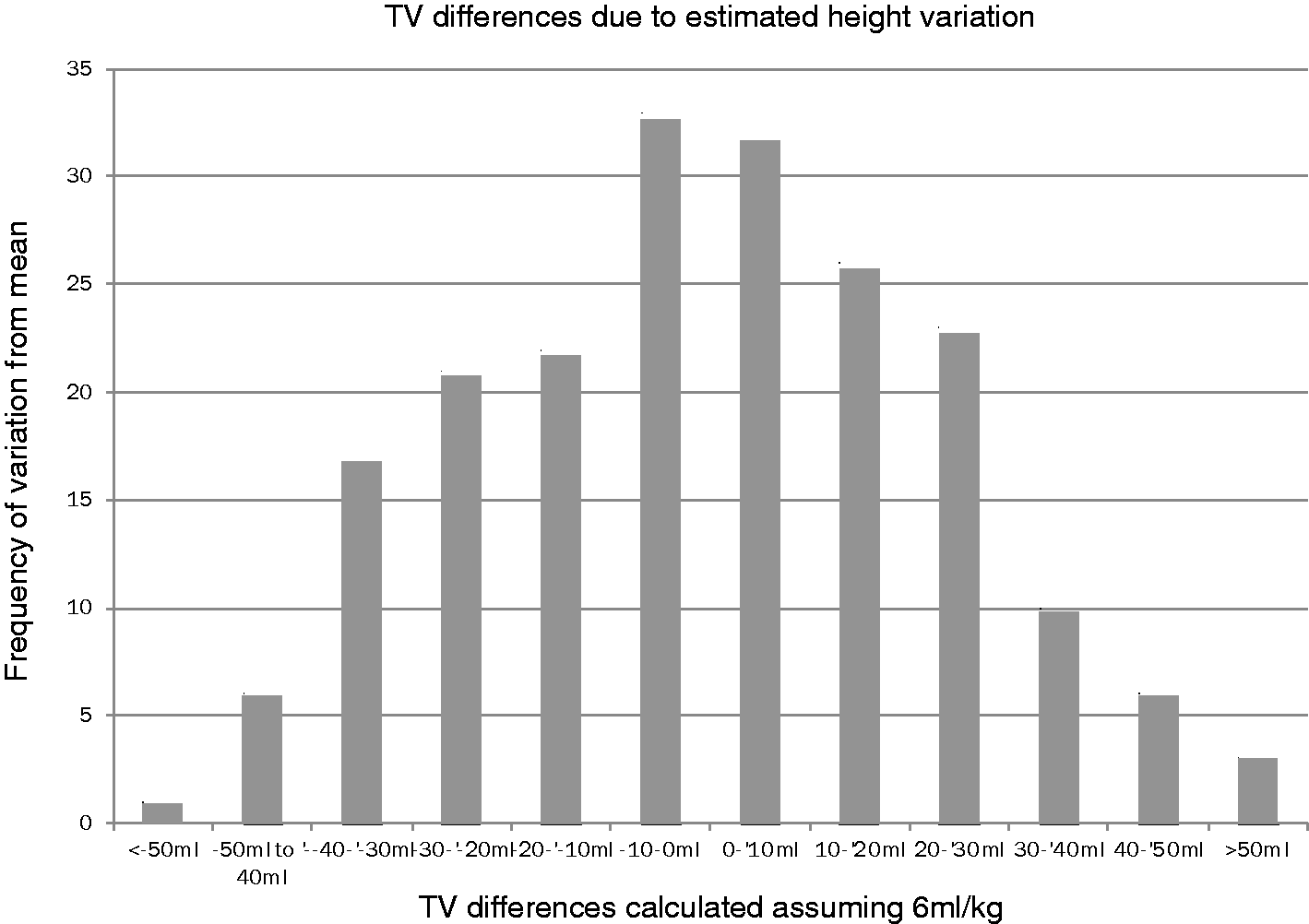
Discussion
The case for lung protective ventilation in high-risk ICU patients has been well made. The majority of busy centres in the UK have adopted a measurement technique to estimate the ideal starting tidal volume; 15 of the 40 sampled individuals reported not using a measurement technique. Visual estimates are known to be inaccurate, and using actual body weight will invariably lead to worsening ventilator-associated lung injury. Telephone questionnaires do not necessarily represent unit protocols. This was a study assessing human error and its impact on ventilator settings, and so establishing a real time ‘shop floor’ element was considered important. Others have conducted formal surveys of unit practice directed at senior physicians and aiming to discover unit protocols. 7
The degree of variability in tidal volume that depends on a simple height measurement is surprising. Unfortunately, this human error in measuring height is amplified by the ARDS-net formula and multiplication when setting a tidal volume. The importance of the height measurement should not be under-estimated as it is unlikely to be repeated during an intensive care admission and will have implications throughout that patient’s ventilation period. The measurement is also often performed ‘in a hurry’ on admission.
Our attempts to find a cheap and easy alternative have met with variable success. Some measures are intrinsically difficult. Measuring sternum to fingertip always required two people (one to hold up the arm) and often involved moving some lines attached to an arm. We have settled on using 2-m tapes, as we believe they provide the most accurate and precise measure of height. There is still potential for human error. The longer length means there is less movement error than with a 1-m tape and was more likely to be a two-person technique. With the 2-m tape there also seemed to be a greater propensity to lay the tape adjacent to the patient and stick to measuring the straight lines of the bed surface. The 1-m tape quite often resulted in measuring the contours of the patient! Ideally a mechanical method of height would be the best solution, but this has to be balanced with cost, multi-patient contact, and infection control.
A large number of our nurses took part in this study, as logistically having the same group of 20 nurses making all of the measurements was not feasible. While this in theory could increase variability, the required measurement calculation is a straight forward task. The obvious weakness with this project is of study bias. Our nursing colleagues performing the height calculation were unashamedly trying to ensure their measurements were accurate. This unfortunately raises the bigger question: how inaccurate are our estimates both in other ventilation studies and in day-to-day care?
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.