
Abstract
Background
Low tidal volume ventilation improves outcomes in acute respiratory distress syndrome. Calculation of this volume requires knowledge of a patient’s gender, and height, which may not be available in emergency admissions, and the subsequent application of a nomogram. The objective of this study was to test the accuracy of a calibrated measuring tape that reads in mL of tidal volume when the ulna is measured.
Methods
The measuring tape was used to obtain an estimate of a subject’s tidal volume from their ulna length, and standing height was then measured (reference method).
Result
A total of 100 healthy volunteers were included. Mean tidal volume was 450 mL for males and 372 mL for females when calculated from the height. Comparing tidal volumes from the tape with those from the reference method, Bland Altman analysis showed a bias of −10 mL (limits of agreement (2SD) −74 mL to 54 mL) for males and a bias of −36 mL (limits of agreement (2SD) −88 mL to 16 mL) for females. Predicted mean tidal volumes were 5.7 mL/kg (95% CI: 5.1–6.3 mL/kg) for males and 5.8 mL/kg (95% CI: 5.3–6.2 mL/kg) for females.
Conclusions
Usage of a calibrated measuring tape produced accurate estimates of tidal volumes required for lung protective ventilation in healthy volunteers.
Introduction
Low tidal volume ventilation (6 mL/kg predicted body weight (PBW)) reduces mortality in acute respiratory distress syndrome (ARDS). Despite general acceptance of lower tidal volumes as a standard of care in ARDS uptake remains limited with multiple barriers to successful implementation. One such barrier in emergency ventilated admissions is not having prior knowledge of the patient’s height, in order to calculate the PBW. Recumbent length measurement and visual estimation are the two most commonly employed strategies to obtain height, though recent evidence suggests that anthropometric relationships may also be successfully used for this purpose.
Visual estimation of height is often used, along with a nomogram to convert the estimated height into a tidal volume. This has been shown often to be inaccurate.1,2 It has also been shown that the ventilator settings following tracheal intubation frequently remain unchanged, 3 or there may be at least a time delay in between the initiation of mechanical ventilation and the consideration of the patient’s height and thus tidal volume. A simple rapid tool for tidal volume prescription could improve this.
A recent study in a cardiac intensive care unit examined the relative ability of different methods of measurement to give the height of elective surgical patients on admission to intensive care unit when they were ventilated and recumbent. The patients had all been measured preoperatively, and thus the true height was known. Inferring the standing height from knee height (Chumlea technique), or ulna length, outperformed recumbent length measurement and visual estimation of height. 4 The length of the ulna is used to estimate height, where it is not possible to directly measure, in the malnutrition universal screening tool, from the British association of parenteral and enteral nutrition, 5 and has been shown to provide good estimates of true height. 6 Moreover, ulna length has been shown to be as good as height in predicting pulmonary function test results. 7 In one study of 507 English and Portuguese patients, the mean and SD of the difference between standing and height inferred from ulna length were 0.3 ± 2.7% of height. 8 The standard error of the height estimate was 4.6 cm.
The forearm is readily available in most ventilated patients and easy to measure. We have designed a tidal volume measuring tape for the ulna, where the length of the ulna is read as mL of tidal volume, thus removing the need for a nomogram (see Figure 1). The relationship between ulna length and height was taken from the malnutrition universal screening tool data. The relationship between height and PBW is given by Devines formula: male patients PBW = 50 + 0.91 (centimetres of height – 152.4); female patients PBW = 45.5 + 0.91(centimetres of height – 152.4).
9
The resulting PBW was then multiplied by 6 mL/kg to give the tidal volume.
Tidal volume measuring tape for males < 65 years old. Instructions: cut along the dotted lines then fold over the solid lines to produce a ruler. Measure the distance from the olecranon to the midpoint of the ulna styloid (left side if possible). Read off the tidal volume.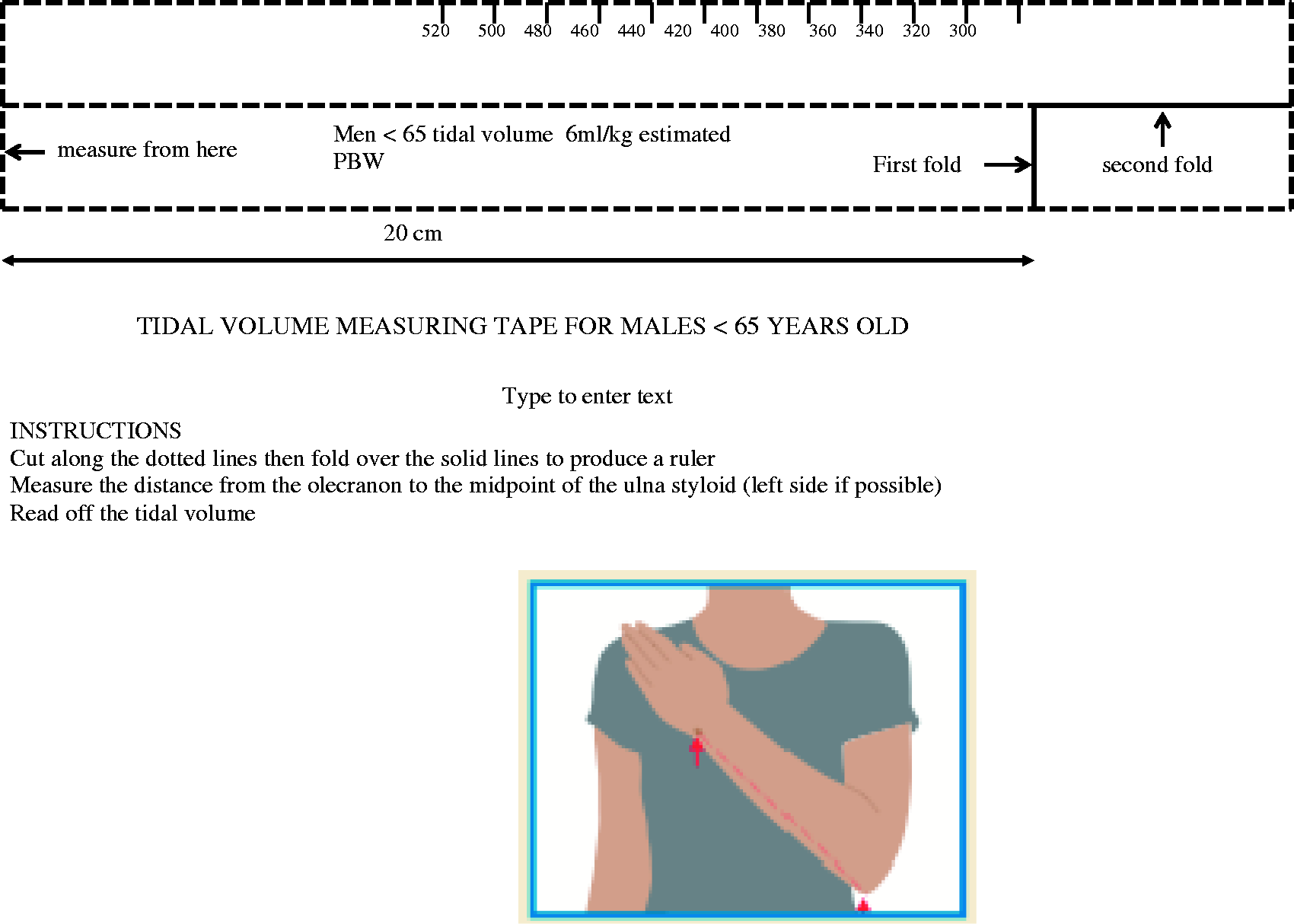
The transformations of height into PBW and PBW into tidal volume are identical for a height obtained from standing measurement and a height inferred from ulna length. The accuracy of the tidal volume thus depends on the ability of ulna length to predict height.
We believe this will allow rapid estimation of optimal tidal volume and could improve adherence to lung protective ventilation.
In this study, we tested the accuracy of tidal volume estimations in healthy volunteers.
Methods
We recruited 100 healthy adult volunteers (43 male, 57 female, all aged under 65 years of age). Our local ethics committee waived the need for full ethical approval. In the seated position, using the appropriate tape for age and gender, the left ulna was measured from the mid point of the ulna styloid to the olecranon. The tidal volume was then read from the tape. The subject’s height was measured standing upright against a wall with their shoes removed, looking straight ahead, using a seca 206 bodymeter wall-mounted mechanical measuring tape. Measurements were performed once only. No subjects were excluded.
Results
Using the tape was quick and easy, with a tidal volume recordable in under 20 s. Mean tidal volume was 450 mL for males and 372 mL for females when calculated from standing height. Bland Altman (see Figure 2) analysis showed a bias of −10 mL (limits of agreement (2SD) −74 mL to 54 mL) for males and a bias of −36 mL (limits of agreement (2SD) −88 mL to 16 mL) for females. We indexed the tidal volume difference to mean ideal body weight to give a predicted mean tidal volume per kg: 5.7 mL/kg (95% CI: 5.1–6.3 mL/kg) for males and 5.8 mL/kg (95% CI: 5.3–6.2 mL/kg) for females.
Bland Altman plot of the difference in tidal volume from the two methods versus the mean tidal volume. Male bias: −10 mL, 95% limits of agreement (−74 mL to 54 mL). Female bias: −36 mL, 95% limits of agreement (−88 mL to 16 mL).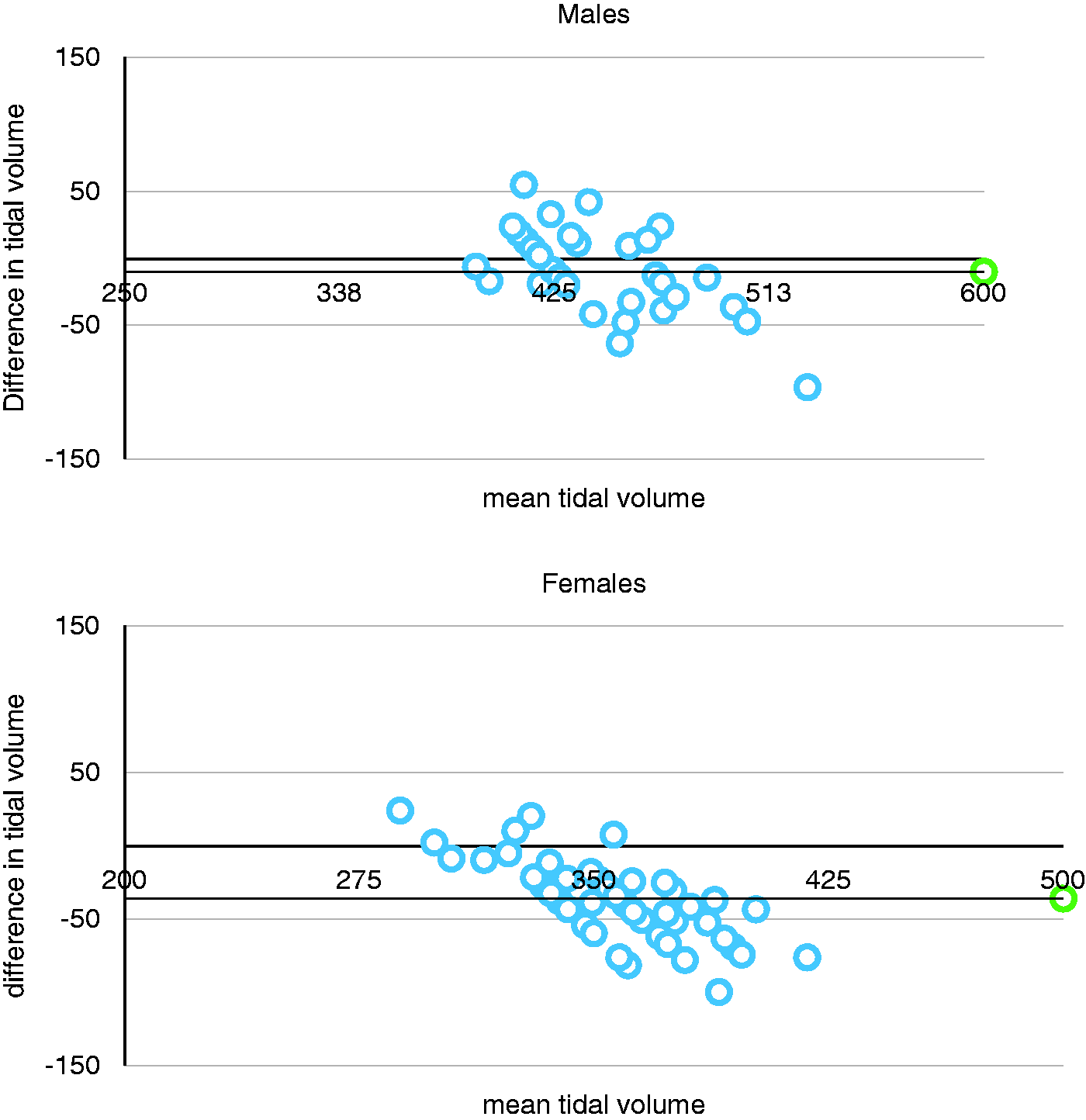
Discussion
We have shown that the ulnar tidal volume ruler gives a reasonably accurate estimation of tidal volume in healthy volunteers. If used routinely, 95% of tidal volumes would be between 5 and 6.5 mL/kg. Previous studies have suggested that usage of the ulna to estimate height for the prescription of tidal volume would improve accuracy compared with visual estimation and recumbent length measurement. 4 We have simplified and speeded up this process.
Our tape was tested in a mixed group of 100 healthy volunteers. We did not identify sub groups including ethnicity which could potentially affect accuracy. 10 The tape is different for the age group over 65, and we were unable to test it in our volunteers (all <65 years old).
Currently, a variety of methods are used both to estimate height and estimate tidal volume.
In recent ventilation studies, the control group tidal volumes are often significantly above 6 mL/kg despite protocols specifying this target.11,12
Our tape is very easy to use, and we believe that it is sufficiently accurate to be used clinically. Further studies are required to quantify how accurate it is when used in more diverse populations.
We have designed the tape so that it can be accessed by anyone. The PDFs (A4 or A3) can be downloaded at http://tinyurl.com/TidalTapesA4 and http://tinyurl.com/TidalTapesA3. Care must be taken when printing to ensure that the printer is set to actual size (the dimensions of the tape are alongside and should be checked).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.