
Abstract
As clinicians, we are well acquainted with using randomised controlled trials, case–control studies and cohort studies together with p-values, odds ratios and confidence intervals to understand and improve the way in which we care for our patients. We have a degree of familiarity, trust and confidence with well-performed scientific quantitative studies in critical care and we make a judgment about our practice based on their recommendations. The same cannot be said of qualitative research, and its use accounts for only a small proportion of published studies in critical care. There are many research questions in our environment that lend themselves to a qualitative research design. Our positivistic education as doctors potentially incites distrust towards such studies and, as such, they are seldom undertaken in our units. We aim to describe and discuss the differences between quantitative and qualitative research with focus being given to common misunderstandings and misconceptions. An overview of the methods of data collection and analysis is provided with references towards published qualitative studies in critical care. Finally, we provide pragmatic and practical instruction and guidance for those wishing to undertake their own qualitative study in critical care.
Two sides of the same coin
Scientific research is historically based on formulating a hypothesis, collecting objective data in a controlled manner, demonstrating repeatability, predictability, reproducibility and thus generating new laws or theories about the world around us. 1 In medicine, we have taken this accepted scientific method and applied it to elucidate clinical unknowns.2,3 As clinicians, we are well acquainted with many types of quantitative research, as we are drilled in its inner workings at all stages of medical education. 4
Quantitative research is not perfect; it cannot answer every clinical question that we can ask. The study of complex sociological phenomena relating to patient care, for example, is difficult using quantitative methods. 5 Qualitative research could have an important role to play in tackling such clinical unknowns. It is possible that it is under used as a method in critical care because, as doctors, we are grounded in the accepted scientific method and we may be unfamiliar with how qualitative research is conducted. Therefore, we may struggle to accept it as a proper way to conduct clinical research. The finding that qualitative research accounts for only a minor proportion of medical publications supports this. 6 In fact, the qualitative-quantitative debate is one that is old but by no means over. 5 Both types of purists encourage the ‘incompatibility thesis’, where quantitative and qualitative research is mutually exclusive. 7 This is no longer such a rigid construct and some have embarked upon ‘mixed methods’ studies that do just this.
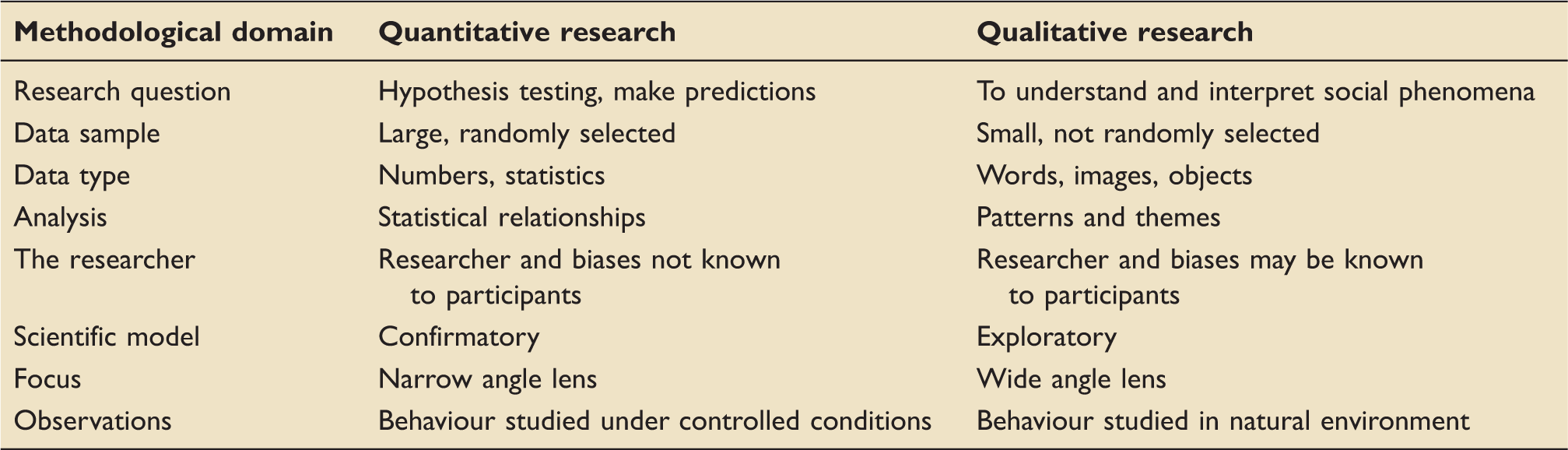
Quantitative and qualitative research methods derive from two very different historical research philosophies. 8 Positivism is the accepted scientific approach as described. It relies on a stable reality that can be observed and described from an objective viewpoint. Relationships between variables are sought and predictions from previous observations are often made. It is enshrined in our culture so much so that the scientific community often considers claims not grounded on positivistic thought invalid. 9 Interpretivism is concerned with the study of phenomena in their natural environment through observation and interaction by the researcher, who is also the instrument of measurement and analysis.
Summary of differences in methodology between quantitative and qualitative research.
Epistemological and ontological positions
These are complex topics that are seldom well described or understood. A basic working introduction is provided only. Ontology is the study of being or existing.
10
There are two elementary ontological positions:
Objectivism – This conditions that social phenomena exist and have a meaning. For example, illness exists on a hospital ward and is a reality. All you have to do is count and categorise the number of pathologies or collate the early warning scores. You can then use this to monitor the impact of an intervention on the ward. Constructionism – This is the ontological opposite of objectivism. This conditions that things do not exist independently and we, as humans, construct their meaning. For example, some may argue that there is no general definition of ‘illness’ on a hospital ward as our perceptions of illness may change over time. One doctor may describe a patient as ill, but another may say the patient is actually improving and doing well. (You will no doubt be familiar with such a situation when you are reviewing a patient on the ward.)
Epistemology is the study of knowledge and our process of knowing.
10
There are two elementary epistemological positions:
Positivism – The positivistic position is the normal accepted scientific method through which objective measurements are taken to test a working hypothesis about the world around us. The researcher is the scientist. The positivistic viewpoint is that all research should emulate the physical sciences model and that anything other than this is deemed unscientific and therefore, invalid. Interpretivism – It is not possible to interpret the objective results of a positivistic study. The facts are the facts. Interpretivism accepts a constantly changing world with unstable definitions and meanings. It does not look to find pre-existing truths. The researcher is the detective and the machine of measurement and analysis.
There are thus two research paradigms
10
that are fundamental to understanding the differences between quantitative and qualitative research:
The positivist paradigm – This combines objectivist ontology and positivistic epistemology. This gives rise to quantitative methodology and a design such as a randomised controlled trial or case control study. The interpretivist paradigm – This combines constructivist ontology with interpretivist epistemology. This gives rise to qualitative methodology and a design such as ethnography, interviews or focus groups.
There is arguably a third paradigm, referred to as pragmatism. This is non-committal towards either positivism or interpretivism and instead focuses on the ‘what’ and ‘how’ of the research question. The methodology of such studies commonly employs mixed methods. 11
Methodological quality and rigour
The degree to which the findings of a qualitative study can be deemed believable or trustworthy is a question that is central to the qualitative-quantitative debate. 5 Qualitative research is commonly criticised from a positivistic viewpoint when indicators of quality for quantitative work are wrongly applied to qualitative studies. Quality should be robust and there are important parallels. For example, a full account of the sampling strategy, the data collection technique and the process of analysis should be provided in sufficient detail such that another qualified researcher could repeat it in their own setting.
Analogous terms for markers of quality in quantitative and qualitative research.

Credibility
We would normally describe confounding and bias as markers for internal validity. For qualitative research, the appropriate term is credibility.
12
Credibility can be ensured in a number of ways, such as, but not limited to:
Respondent validity – presenting the initial analysis of the study to the research participants. This enables the researcher to inform the participants what they think is happening. The participants then have the option to refute or accept the interpretation of the researcher. Triangulation – This is the process of asking different questions, using different sources and using different methodologies to gather data. Prolonged engagement – The researcher must dedicate the time needed in the field to achieve saturation of data. This may also help to compensate for seasonal effects and reduce the distortion of the environment by the presence of the researcher. Member checks – At any stage in the study, the researcher may ask the participants to read through a transcript of an observation or interview from which they have participated. Do the words match what they intended to say? Familiarisation with culture – This usually occurs prior to data collection and can be undertaken by preliminary visits. Additionally, prolonged engagement can afford familiarisation during the study. Ensuring honesty from participants – participants should be given the opportunity to refuse or withdraw so that only those who are willing are studied. There should be no right answers expected. There should be no aim to criticise individuals or organisations. Peer review – This should be welcomed and employed to refine and shape ideas, methods and analyses.
Transferability
We would normally refer to how the findings of a study can be applied to a specific or a wider population. In qualitative work, the readers make a judgement regarding how findings can be transferred to other settings. 12 It is not possible to generalise the findings of a project that is specific to a small number of individuals and environments. Instead, transferability invites readers to make connections between parts of the study and their own experiences. The reader scrutinises the detail of the project and if there are similarities, they transfer the findings to a different setting. This can only be done if the authors provide as much detail as is possible. This is analogous to providing detailed patient demographics, for example. Such detail may include, but not be limited to, the details of the participating organisations, the number of field operatives, the method and nature of data collection and the length of study. This is often referred to as the ‘thick description’.
Dependability
This refers to the theoretical situation where a project could be replicated with similar participants in a similar setting and provide similar findings. 12 In quantitative work, it is not possible to obtain validity without reliability and likewise, dependability is intimately linked with credibility. It is therefore possible to argue that you can demonstrate dependability by demonstrating credibility. Alternatively, both credibility and dependability can be assessed separately by externally auditing the methods of data collection.
Confirmability
A domain that is commonly the subject of criticism from a positivistic viewpoint. It is concerned with the degree to which the researcher biases the findings, as the researcher is simultaneously the detective and the machine of measurement and analysis. 12 Qualitative research allows for each researcher to bring a different perspective to a study. Confirmability relates to how the findings of a study could be confirmed by others. An external researcher can judge this domain by studying the project site file. An audit trail of key decisions that are made together with a justification from the researcher throughout the project can also enhance confirmability. Ultimately, researchers should be ‘reflexive’ in that they are transparent about the influence they could have on the analysis. 13
An assortment of methodologies
An introduction towards commonly employed methods is provided only. The methodological literature base is extensive and complex, however, sources of further reading are abundant.5,14
Phenomenology
Commonly employed in the psychological sciences and beyond, this method aims to understand the individuals’ experiences and the attached meanings. Interviews allow participants to answer open questions in their own words in a way that closed answer questionnaires or surveys are unable to.
Ethnography
This is a technique commonly used in anthropology where the researcher is immersed in, and may interact with, the community or culture being studied for an extended period of time. Field notes and observations are made about the environment, what is said and what is done. Complex phenomena can be analysed and broken down into their component parts or themes. Observing behaviour in which the researcher is immersed allows for the generation of insights that other methods simply cannot provide. It is time and labour-intensive and as such, teams can be successfully used to divide the burden. It is commonly used in triangulation with interviews and focus groups.
Interviews and focus groups
Commonly employed in medical studies, these aim to produce transcripts of the participant responses to researcher-lead questioning. They can be structured, semi-structured or in-depth. Most prefer the semi-structured approach where a balance is drawn between researcher freedom and the need for a high level of technical interview skill, as is required for in-depth interviewing.
Case studies
This is often confused with the more familiar medical case study publication. Case studies are loosely defined as the examination of a phenomenon within its own context using many different data sources. Within this lie many different sub-methods of study. 15 Case studies of this sort are uncommonly encountered in the medical literature.
Mixed methods
As previously described, mixed methods refers to the situation where quantitative and qualitative methods are combined in order to answer a shared research question.
Data analysis and interpretation
“Data don’t speak for themselves. We have to goad them into saying things.” 16 The data generated by a qualitative project will mainly be in the form of transcripts and field notes, although other forms such as pictures or videos may be used. This will need structuring and organising so that sense can be made of it. The research team will have to become familiar with the dataset and then go about generating codes and themes from it, before generating conclusions or new theories. As previously stated, the researchers are the instruments of measurement and analysis; no computer will be able to improve judgment. It is a manual process, however you do it.
The process is deductive or inductive, depending on where the hypothesis is defined in the research process. In null hypothesis significance testing, you start with a hypothesis and then go about collecting data to prove or disprove it. This is deductive. In some forms of qualitative research, the hypothesis comes from the data and this is referred to as inductive. From the transcripts or field notes, codes are used to ‘tag’ the data so that it can be made manageable. An example of coding is provided in Figure 1. There are many ways of undertaking coding and the best advice is to find a way that works for you, whether it be using advanced computer software or writing on printed transcripts, which is much easier.
A crude example of how a qualitative interview transcript is coded.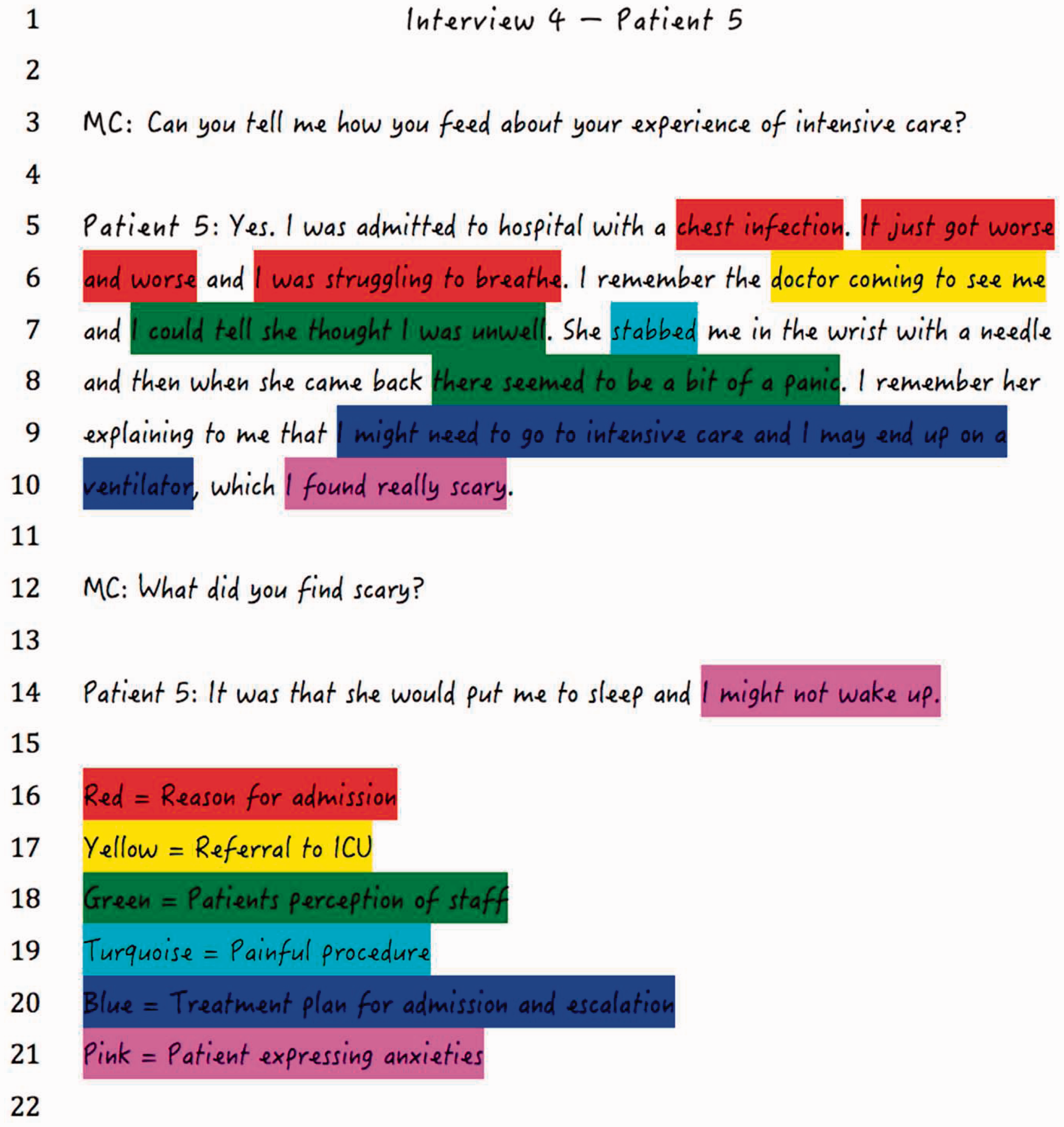
You can decide what code you want to use by cross-referencing with material that is already know (called an ‘a priori’ code) or by using your data to make a code (called an emergent or grounded code). These codes, together with the text that has been tagged, can then be used to develop themes. Themes can be grouped together as sub-themes and a thematic hierarchy is formed. Quotations can be used to illustrate your chosen themes.
There is no one method for analysing data, although thematic analysis and grounded theory appear commonly in medical literature. There are many commonalities and overlaps within all methods of analysis. Grounded theory, developed in the 1960s, is a commonly cited inductive method and refers to a way of generating new theories to explain phenomena from data. There are many definitions and variations of grounded theory, owing to its evolution and rich history. Confusion is caused by authors commonly referring to work employing a thematic analysis as using grounded theory. This common misunderstanding is typically due to a poor knowledge of its defining principles. One such principle is that the relevant literature is not consulted prior to embarking on data analysis. This, in theory, avoids the analysis being influenced by previous research. In addition, grounded theory can only be used for certain forms of sociological questioning. Data are simultaneously collected and analysed followed by more collection and analysis until it is possible to draw conclusions.
Thematic analysis, however, is a flexible method that can be used to analyse most types of sociological data. The aim is to summarise the data but not necessarily with an ultimate aim to develop a new theory. Some would argue that grounded theory is a method with philosophical underpinnings whereas thematic analysis is simply a method. The mechanics of how the data are analysed is largely similar.
The practicalities of your own project
The prospect of setting up your own qualitative project in critical care need not be daunting. There are, however, some points for consideration.
Designing the project
The research question posed needs to lend itself to a qualitative design. In general, a question that looks to examine how people deal with and interact with other people is suitable. Finding such unanswered research questions in critical care should be straightforward enough. Once this has been decided, the importance of liaising with a local university social sciences department cannot be overemphasised. This will enable the method to be selected and refined. Expertise can also be sought with regards analysis.
Getting access
One of the barriers to this type of research being conducted in our units could be that we appear to be a closed community. Just as we may find qualitative research confusing and intimidating, sociologists may find our community and environment the same. More collaboration between clinicians and the social sciences community could enable a more open approach to answering important questions that can improve care. In addition, there is the problem of permissions. It can be difficult for insiders to examine their own environment through the looking glass of an outsider. Likewise, it can be difficult to gain access and permissions as an outsider wanting to look in on another organisation.
Ethical approval
There is a grey area with regards to the ethics of a qualitative research project in critical care. This will ultimately depend on the design of the project, and who is being studied. Liaising with the local research ethics committee (LREC) will be key. In 2011, GAfREC guidelines recommended that studies limiting involvement to NHS staff, or requiring access to a care organisations premises or facilities, but not involving patients or service users, be exempt from LREC review. 17 Therefore, if you plan to interview and observe staff members, LREC review is not needed. If, despite this, you believe that your project raises ethical issues, a local university ethics committee may consider your protocol and give a favourable ethical opinion. This can be reported in the method.
Collecting the data
The major challenge is that data collection and analysis is time consuming, labour-intensive and complex. This can be mitigated with adequate funding and arguably, this type of research costs significantly less than wet-lab based research. There are three areas that need to be considered when planning the project timeline:
Downtime – Just as in many other types of clinical research, not all the time assigned to data collection will be used in this way. Just as a study regarding patients with upper gastrointestinal haemorrhage is dependent upon patients presenting with this complaint, a qualitative study regarding end of life decisions is dependent upon having such situations to observe. Transcribing – You may want to take short hand observations whilst ‘in the field’ and write these up at a later stage. You may record your interviews and wish to transform these into anonymised transcripts. The time required to perform this task is colossal. Data-analysis – A rough guide is that for every one hour of interview or observational work, five is needed to analyse the data. The data does not speak for itself and a computer programme cannot produce the answer. Whilst it is true that computer programmes are available to assist with analysis, the coding process will continue to be manual. It is, however, an intellectually demanding and incredibly rewarding process.
How much data?
Enough data are needed to reach theoretical saturation. Saturation is when further data collection ceases to add any understanding to what has already been gained. It may be difficult to predict how long it will take to reach this point and therefore, the research timeline can be interrupted.
Interpretation
A collaborative approach can enhance the ability to draw conclusions from the data.
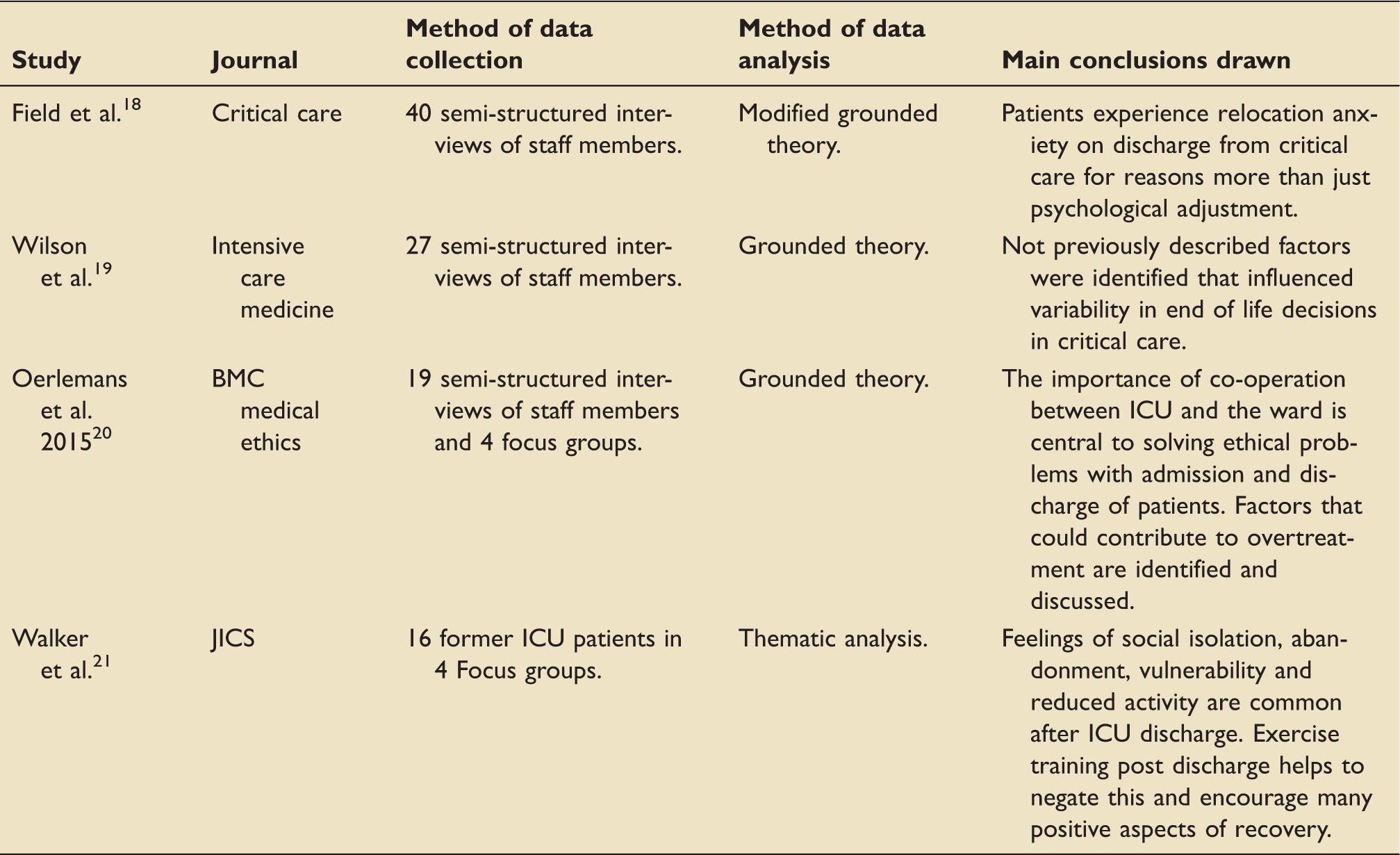
Recent examples of qualitative research in critical care
An example of recently published qualitative studies in critical care.
Conclusion
“Research is to see what everybody has seen and think what nobody has thought.” 22 Despite being initially applied to biochemistry, this quote by the Nobel laureate biochemist Albert Szent-Györgyi can relate to experienced clinicians being well placed to use their own environment to formulate research questions that can be investigated using qualitative methods. We argue that qualitative research is under used as a research tool in critical care despite the endless permutations of clinical questions that can be asked. Our positivistic education in medicine is only part of the reason, and this is changing, with social science topics at medical school being introduced. The fact that qualitative methods are seen as difficult and inaccessible and that any project would be time consuming and hard work cannot be escaped. Just like any other research, the method has to be mastered and data needs to be rigorously collected and analysed. We would argue that the rewards of being able to deeply understand an observed phenomenon that cannot be studied quantitatively is ample compensation, more so when this can improve the way we look after our critically ill. Has the time come for more qualitative research to be performed in our units? We would argue, yes.
Footnotes
Acknowledgments
The authors wish to acknowledge the Department of Critical Care Medicine, Central Manchester University Hospitals, Manchester, UK and the Faculty of Health and Medicine, Lancaster University, Lancaster, UK.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.