
Abstract
Patients who survive critical illness often report deterioration in health related quality of life. This has not been shown to improve following post-intensive care unit (ICU) self-directed exercise. The Post Intensive Care eXercise (PIX) study demonstrated improved objectively measured fitness following a supervised exercise programme following critical illness and also suggested beneficial effects on physical and mental health. The qualitative arm of the PIX study reported here utilised focus groups to explore in more detail recovery from critical illness, quality of life following hospital discharge, perceptions of the exercise programme and it’s impact on perceived well-being. Sixteen participants (eight of whom underwent the supervised exercise programme) were allocated to four psychologist lead focus groups. Themes identified after hospital discharge centred on social isolation, abandonment, vulnerability and reduced physical activity. However, patients in the exercise group described exercise training as motivating, increasing energy levels and sense of achievement, social interaction and confidence. This study adds to the sparse literature on the patient experience post critical illness. It supports the improvements in physical and mental health suggested with exercise in the PIX study and would support further research in relation to the effects of supervised exercise and rehabilitation programmes post critical illness. It recommends that future comparative outcome studies in this patient population also include interview-based assessment as part of assessment of quality of life and an individual’s functional status.
Introduction
Many patients who survive critical illness suffer from problems that adversely impact on subsequent quality of life.1–3 These include physical conditions which may lead to muscle weakness and fatigue, in addition to psychological effects such as long-term cognitive dysfunction 4 depression5,6 and post-traumatic stress disorder. 7 Survivors therefore suffer a reduced health related quality of life (HRQoL) in comparison to their pre-morbid estimate. 8 Long lasting restrictions in physical, social and psychological functioning are particularly prevalent in patients who have stayed in an ICU for more than 2 days and this population is an appropriate target for rehabilitation. 9 However, several studies have failed to demonstrate improvement in HRQoL with non-supervised exercise programmes that place the onus to exercise on the patient.10,11
This recognition led to the PIX study 1 which investigated the effectiveness of an 8 week in-hospital supervised exercise programme, on physical fitness and HRQoL, for survivors of critical illness (minimum of 3 days ventilation) following hospital discharge. The study demonstrated an improvement in objectively measured fitness, as well as suggesting small improvements in physical and mental health in the intervention group as measured by the 36-item Medical Outcomes Study Short Form (SF-36).
However, many patients report problems following hospital discharge that affect quality of life but fall out with the scope of the above standard outcome measures, such as being unable to care for themselves, poor social integration or delayed return to work.12–15 Furthermore, recovery has been found to be a dynamic process with outcomes varying at different time points.16,17 These factors, as well as the nature and timing of exercise, may explain in part, why several studies using standard outcome measures have failed to demonstrate any benefits of exercise programmes in ICU survivors.10,11
Without a better understanding of the needs of ICU patients following hospital discharge and the process by which they recover at home, interventions will remain unfocussed. Despite this, a review of the literature revealed only three qualitative studies in this area, and only one of these investigated participants’ experiences of community services.18–20 This study found general reluctance to make use of these, with counselling and support groups viewed particularly negatively, as if indicating a failure of individual will. 20
To complement the objectively measured improvements in fitness and standard health related outcome measures in the PIX study, 1 this qualitative arm utilised focus group methodology. This was in order to gain a more in-depth insight into patients’ perceptions of their quality of life after hospital discharge and their experiences of aftercare services, be it usual care or the PIX exercise intervention programme.
Methods
Design
Focus groups were chosen both for pragmatic reasons and because the group context can facilitate disclosure and the airing of a range of views. 21 A previous qualitative study of psychosocial recovery in the community following discharge home from ICU found a degree of participant reticence in discussing psychological aspects. 20
The assumptions guiding the research questions, data collection and analysis were that methods could be employed to reflect the reality of participants’ experiences, understandings, opinions and views whilst accepting that these arose in a specific social context and required subjective analysis on the part of the researcher. Methods employed to enhance the trustworthiness of the research 22 are described below.
Sample and selection criteria
Sample baseline characteristics for focus group participants versus others.
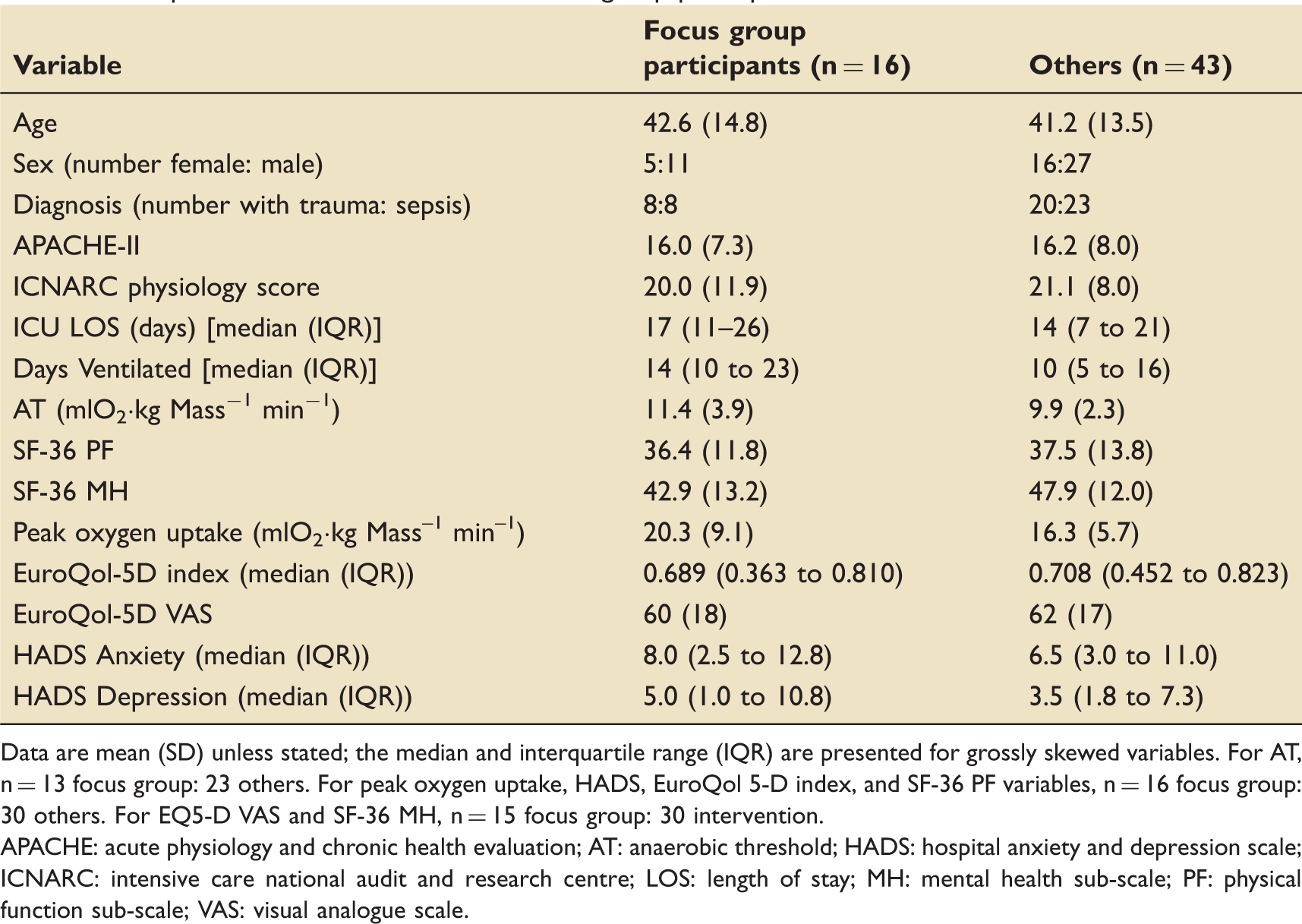
Data are mean (SD) unless stated; the median and interquartile range (IQR) are presented for grossly skewed variables. For AT, n = 13 focus group: 23 others. For peak oxygen uptake, HADS, EuroQol 5-D index, and SF-36 PF variables, n = 16 focus group: 30 others. For EQ5-D VAS and SF-36 MH, n = 15 focus group: 30 intervention.
APACHE: acute physiology and chronic health evaluation; AT: anaerobic threshold; HADS: hospital anxiety and depression scale; ICNARC: intensive care national audit and research centre; LOS: length of stay; MH: mental health sub-scale; PF: physical function sub-scale; VAS: visual analogue scale.
Ethics approval was received from the Newcastle and North Tyneside 1 Research Ethics Committee on 16 January 2008 (Ref:07/H0906/137) and all participants provided written informed consent. The trial was registered with Current Controlled Trials no. ISRCTN65176374.
Data collection
Focus groups were conducted by a clinical psychologist (WW). In order to facilitate open disclosure no other staff members or researchers were present. Wilkinson’s guidance 21 on focus groups was adhered to, to enhance data quality and the experience of participants.
The main questions were:
How has your stay in ICU affected your quality of life following discharge? Have you any comments about the aftercare you received or would have liked to receive? What was your experience of the exercise programme and its effects? Have you any other comments or suggestions about the exercise programme? Did you carry on exercising independently after the completion of the exercise programme?
Further questions arising from the discussions were added to the schedule if they did not arise spontaneously in all groups.
Data analysis and verification procedures
Interviews were audio recorded, transcribed, re-analysed, checked for accuracy and transcripts re-read on many occasions, ensuring sufficient immersion in the data. An audit trail was kept for each stage of the analysis with appropriate peer review. Themes identified during analysis were also sent out to focus group participants, inviting their views.
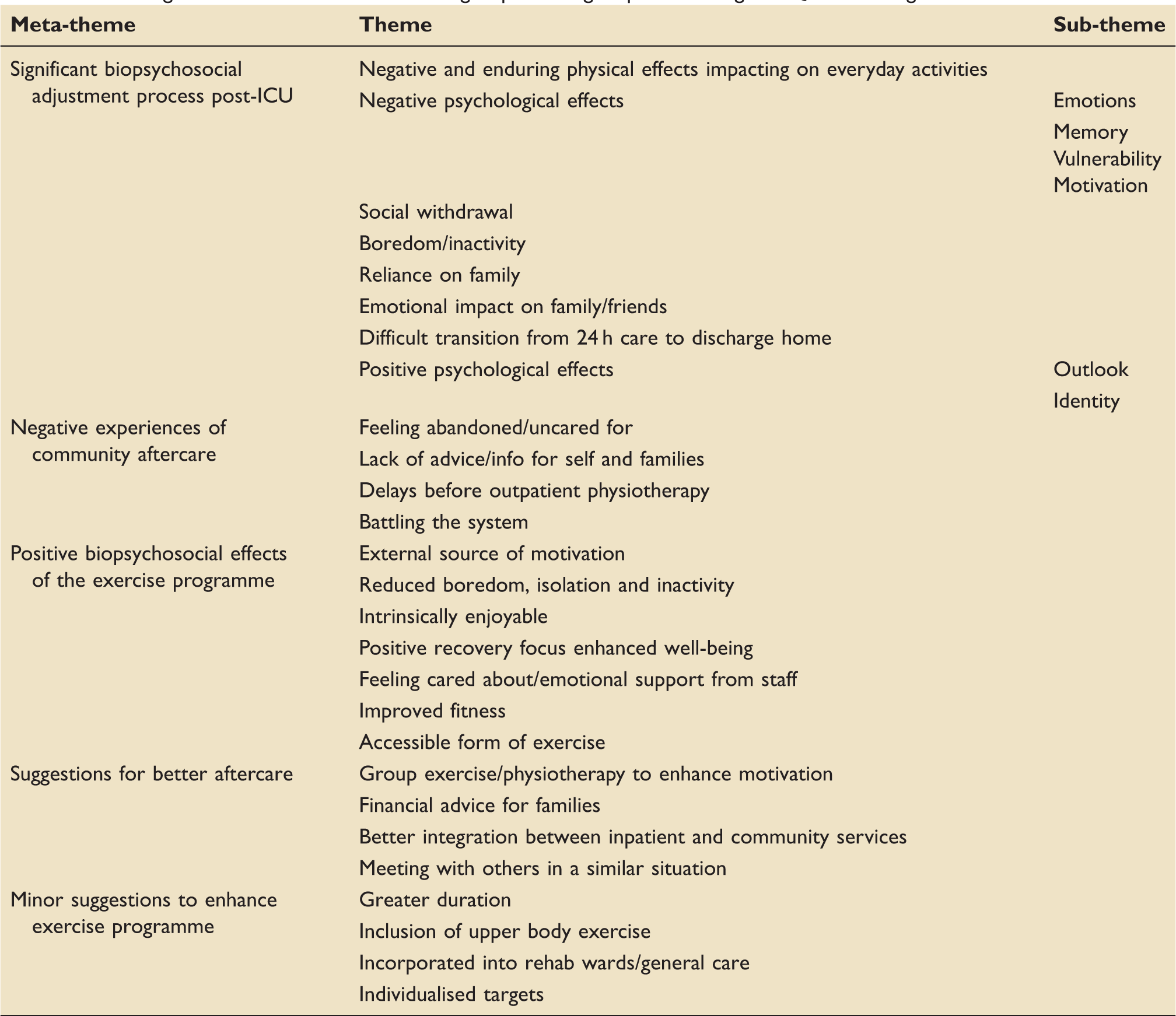
Enduring themes elucidated in the focus groups relating to post-discharge HRQoL including effects of the intervention.
Results
The account that follows focuses on participants’ experiences with regards to their quality of life, physical and mental health following discharge home from ICU and their experience of the intervention/usual care.
Significant biopsychosocial adjustment process post-ICU
Negative and enduring physical effects impacting on everyday activities
There were many ongoing physical problems, even amongst those reporting that they had made a good recovery. ‘I also have double vision … I can’t read … I can’t even watch telly … it’s like being in prison’ ‘I can now walk without sticks … but that’s after two years … ’ ‘I was a mechanic … I can’t do it now. I’m not allowed to drive a car or get on a plane, they won’t let me do anything’.
Negative psychological effects
Emotions
Participants explained how physical changes impacted on them emotionally. ‘It’s a bit degrading that you can’t do what you could do’, this participant having been prescribed antidepressants. ‘I’ve had a lot of anger because I’ve got facial deformities’.
Vulnerability
Some people felt unsafe and scared: ‘ … to sort of have moments on my own, … it’s just a bit scary, … you know if something happens … and there’s nobody to sort of ask’. ‘I was scared. I never used to be frightened of nothing. I was probably too cocky and too confident really, now that I’ve taken a bit of a beating’. This was linked to being confronted with their own mortality, the family of one patient already having planned their funeral.
Social withdrawal
Participants explained how their social lives had changed, e.g. ‘ … since the accident I don’t socialise as much as I used to ‘ … if you go out with friends you know, two years down the line, they don’t want to be talking about your illness’.
Boredom/inactivity
Physical limitations led to high levels of boredom for many, e.g. ‘ … that’s the worst thing about coming out of hospital, sitting doing nothing … ’ ‘ … all I had was the telly … ’ ‘Just bored all the time … I would say that’s the main thing’.
However, despite adjustment difficulties there were also instances of positive effects following the ICU experience.
Positive psychological effects
Outlook
As a direct result of having ‘ … been at death’s door and then … being given a second chance’, for some, the important things in their lives changed and were appreciated more, so that money became less important, and each moment was enjoyed more fully because ‘ … you never know when he’s {death’s} going to come knocking’. For one participant there was a feeling of invincibility, in stark contrast to the vulnerability described earlier due to ‘ … knowing what I’ve lived through … I think that nothing would touch us again … ’
Identity
Some described having become better people, e.g. being ‘humbled’, ‘having a personality change’ and being more considerate of others: ‘I … go out of my way to try and help other people … now … ’
Negative experiences of community aftercare
Many participants spoke about the difficult transition from 24 h care on ICU to finally going home with little aftercare.
Feeling abandoned/uncared for
One participant described how on arriving home ‘ … you just feel like you’re out on a limb all of a sudden’. Indeed there was a sense of feeling uncared, for example ‘ … dumped at home from a taxi with two sticks … I was just a number then’. ‘ … it felt like they just wanted a bed and had to throw me out … I just felt like … sort of abandoned really … ’.
Lack of advice/information for self and families
There was a real sense of being unprepared to go home due to not being forearmed with the necessary information, e.g. ‘ … we were kept in the dark … just to get put back into your home. No guidance for your family as to how to take care of you’. Lack of advice was noted with respect to managing patients’ conditions in addition to information about benefits.
Delays before outpatient physiotherapy
Participants mentioned timescales of 12 months before they were to receive their first physiotherapy appointment, leading one person to seek private treatment in the interim. However, the one participant who spoke much more positively about the transition home from hospital had received physiotherapy in a rehabilitation ward, enabling him to recover sufficiently prior to going home.
Battling the system
Many participants described having to fight for the help that they needed such as physiotherapy, equipment to enable them to complete basic tasks such as going to the toilet ‘ … everything you had to ask for basically’. One participant described how the district nurse arrived with no dressings, expecting the patient to have these. Participants were unhappy about having to take such proactive action e.g. ‘ … you should get that anyway without having to ask’. Battles to attain the correct financial benefits led one person to feel ‘ … like I’d committed a crime’. Another explained ‘It was something else that I had to contend with on top of trying to get better’.
Positive biopsychosocial effects of the exercise programme
External source of motivation
The exercise intervention was favourably contrasted with doing exercises in one’s own home as it ‘ … made you do it, you know’. ‘ … it was structured and I had to go basically … If I’d had the bike at home … I’d have … done five minutes that’s enough’. Furthermore, participants described how it got them into a routine of getting up and going out.
Reduced boredom, isolation and inactivity
Many commented on how the exercise intervention provided a welcome alternative to ‘sitting doing nothing’, e.g. ‘That’s what I liked about coming in to do the exercise group, because they give you something to do’. Furthermore, people appreciated the social element as opposed to being ‘at home relatively locked up’ and reported that it got them doing more.
Intrinsically enjoyable
The exercise intervention was described in very positive terms by almost all participants, e.g. ‘I really enjoyed it’. ‘I love it all every bit of it’.
Positive recovery focus enhanced well-being
Psychological well-being also appeared enhanced, e.g. ‘ … it sort of improved your mind a lot as well’. ‘It gave you … space to think, gave your brain a … break, instead of being sat at home thinking about it constantly’. The positive emphasis on improvement and recovery gave people ‘ … a sense of achievement … every time you went’. ‘ … you felt like you were progressing … ’ with some setting themselves targets to beat each week. It was reported to increase self-reliance rather than becoming over reliant on family and a desire to ‘look after yourself’.
Feeling cared about/emotional support from staff
Participants appreciated the research nurses and physiotherapists attached to the exercise intervention, who would ‘look after you’ by giving out water and providing encouragement and regarded as a welcome and informed listening ear outside of participants’ families. Participants described how nice it was to be remembered by staff and to be given ‘ … one to one … just focusing on you’.
Improved fitness
Participants noted that the exercise programme improved fitness levels, e.g. ‘ … it’s getting you fit as well’. which had a positive impact on activities of daily living ‘ … you can end up doing nothing for months so yeah … it was very good for that side, it actually gets you to a point that you did more … ’.
Accessible form of exercise
The exercise bikes were seen as an accessible means of getting back into other forms of exercise that participants weren’t yet ready for, such as the gym and running or venturing out into the bad weather.
Suggestions for better aftercare
Group exercise/physiotherapy to enhance motivation
Some participants in the control group suggested that being ‘ … in a class with people like myself’ where they would be ‘ … forced into motivation and forced into fitness’ because of the ‘constructive exercise’ it would offer would have been more motivating than exercising alone where the temptation may have been to ‘ … think oh, do I do something else or watch the telly’. This echoed the intervention group’s experiences as described earlier.
Discussion
The PIX study 1 found that when compared to usual care, the exercise intervention demonstrated a likely substantial improvement in early fitness (at week 9) measured objectively using cardiopulmonary exercise testing. This fitness benefit was not sustained following completion of the 8 week exercise intervention with both groups demonstrating similar improvements from baseline by week 26. This effect suggests that the exercise intervention expedited the ‘natural’ recovery process.
This early fitness improvement should expedite a patient’s return to activities of daily living in the months following hospital discharge, but the PIX study suggested only possible beneficial effects on physical health at week 9 and mental health at week 26 in the exercise group as measured by SF36. However whilst some authors have validated the use of SF-36 in the critically ill population, the validity of generic HRQoL instruments for use with survivors of critical illness has also been questioned and the development of other outcome measures developed with this patient group’s involvement, such as iterative interviews, encouraged. 12
The focus group analysis described a richer more detailed narrative of patient experience than may be obtained via standard numerical outcome measures. Themes of abandonment, physical limitation, dependency and social isolation were common, as were uncertainty as to what was safe to do. By contrast the exercise intervention improved participants’ sense of well-being, achievement and desire to progress, filling an important gap in aftercare. The intervention made several of the participants feel fitter and able to do more with increasing activity levels. The impact extended beyond physical effects, improving venturing outside the house, motivation and social inclusion.
The intervention’s positive recovery focus contrasted with some messages communicated to patients by both family members and doctors. Many participants were keenly aware that they had nearly died as family members needed to share how their illness had impacted on them. It has been pointed out that the patient’s lack of memory for the illness in ICU can make for unrealistic expectations of recovery 24 – a potential harm of ‘not knowing’25,26 and so the focus of critical care has changed from well-meant attempts at overprotection to various strategies to inform patients such as patient diaries. Although there is some evidence of the utility of these approaches, 27 methods of communicating information about near mortality to patients warrant greater consideration as some participants in the focus groups linked their feelings of vulnerability to discussions that had emphasised their near death. This finding led one of the study doctors to change their practice as a result, by conveying information to survivors from critical illness in a more positive and motivating way.
In contrast to the vulnerability expressed by those aware that they had almost died, the exercise intervention’s focus on recovery enhanced some participants’ perceived ability and desire to care for themselves. This provided a counteraction to initial feelings of dependency and institutionalisation following their stay on ICU, which has also been noted by others.28,29
It was also clear that participants from the intervention group greatly appreciated the care they received from the research nurses and physiotherapists. This was in stark contrast to the theme of feeling abandoned/uncared for by services after discharge.
In contrast to previous negative studies on effects of exercise post-ICU,10,11 the PIX study showed a positive increase in objective fitness following the intervention. This may be due to the supervised nature of the exercise programme. The focus group data lend support to this hypothesis, and to the modest suggested increases in physical function and mental health identified by the SF 36, as participants identified improvements in physical fitness and attached great importance to the external source of motivation derived from the intervention. It seemed that getting out of the house and having at least one other person expecting and observing their activity was crucial for exercise adherence which fits with previous research.30–32 Some people continued with independent exercise whereas others admitted to struggling to maintain it, wishing that the intervention could have continued for longer.
The motivating and positive socially inclusive effects of exercise described in the focus groups may in theory extend into other aspects of life, such as encouraging self-caring and earlier return to work. At 6 months post-discharge 25% of post-ICU patients still required help with activities of daily living and 33% had experienced a reduction in employment with associated increase in financial dependency on the state. 33 Interventions aimed at improving this level of independent functioning post critical illness should be a focus of ongoing research.
Strengths and limitations
This is one of very few qualitative studies examining the post-ICU patient experience utilising interview techniques. As such it describes problems of aftercare, anxiety, lack of motivation and lack of social integration and the positive experiences of supervised exercise programmes giving a deeper insight into recovery than may be obtained using only numerical outcome measures.
Whilst the results suggest favourable opinions of the exercise intervention overall, in focus groups, dominant participant voices can increase social conformity, and it is possible that the focus group participants represented a positively biased self-selected group. However, baseline characteristics were similar for both focus group and non-focus group participants. The small sample size of 16 was limited primarily by logistical issues but is within the guidelines of acceptability. 34 However, data saturation may be achieved in a larger study and it follows that these findings are not easily generalisable to the general ICU population.
Conclusion
This study provides important additions to the sparse qualitative research into the quality of life and recovery process post hospital discharge for critical illness survivors and describes themes of abandonment, uncertainty and social isolation as well as participant’s perceived benefits of a supervised exercise programme. These extended beyond an earlier return to physical fitness in the intervention group and encompassed many psychosocial benefits that would not have been apparent from the quantitative outcome measures alone, such as lack of social integration. It emphasises the importance of aftercare services, suggesting that there is considerable scope for improvement, and that broader psychosocial needs that should be taken into account when designing interventions. This study supports further research into the benefits of exercise and rehabilitation programmes post critical illness. In order to gain a more in-depth understanding of the different ways in which individuals negotiate the recovery process, it is recommended that individual interviews should also be incorporated into future definitive interventional studies on quality of life following critical illness.
Footnotes
Acknowledgements
This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number PB-PG-0407-13274). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. The following individuals are acknowledged for making a substantial contribution to the manuscript or providing support for conduct of the study: Louise Cawthorn, Keith Hugill, Susannah Howard and Victoria Goodridge (patient recruitment and follow up, data collection and administration); Alan Batterham (data analysis); Lynn Williams (patient psychological support); Alistair Fale (patient identification).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded with a grant of £217,000 by the National Institute for Health Research (NIHR) Research for Patient Benefit (RfPB) Programme; grant reference number PB-PG-0407-13274.