
Abstract
Elevated cardiac troponin in the critically ill has been associated with increased hospital mortality. However, in critically ill patients with sepsis the results are heterogeneous and less easy to interpret. The objectives of this systematic review were to describe the pathophysiology, clinical relevance and prognostic significance of raised troponin in intensive care patients with sepsis. Articles were identified through a detailed MEDLINE search and additional references were retrieved from the selected studies. A growing body of clinical evidence suggests that although troponins are sensitive biomarkers with prognostic value, they are not independent predictors of mortality. However, vigilance for objective evidence of coronary artery disease is required and patients with atherosclerotic risk factors and elevated troponins may benefit from cardiac imaging. In patients with low pre-test probability for coronary artery disease and elevated troponins, therapy should target management of sepsis and optimisation of myocardial oxygen demand/supply balance.
Introduction
Cardiac troponins have been shown to be indicators of myocardial injury and are accepted prognosticators of myocardial infarction. Myocardial infarction is defined as detection and/or fall of cardiac troponin with at least one value above the 99th percentile of the upper reference limit, together with evidence of myocardial ischaemia, with at least one of the following: (i) symptoms of ischaemia (e.g. chest pain); (ii) electrocardiographic evidence of ischaemia; (iii) imaging evidence of new loss of viable myocardium or new regional wall motion abnormality. 1
Serum troponin concentrations have been associated with increased mortality in almost every clinical setting they have been examined, including sepsis. Sepsis is the physiological response to severe infection. It is defined as the presence (probable or documented) of infection together with systemic features of inflammation.2,3 Severe sepsis is sepsis-induced tissue hypoperfusion or organ dysfunction, and septic shock refers to sepsis-induced hypotension, persisting despite adequate fluid resuscitation, which may be defined as infusion of 30 ml/kg of crystalloids.2,3
Vincent et al. showed that in European intensive care units (ICUs) >34% of patients develop sepsis at some point during their ICU stay and 27% of patients with sepsis die in ICU, rising to >50% in patients with septic shock. 4
Raised cardiac troponin in intensive care patients with sepsis has been associated with adverse prognosis, but it is unknown whether any cardiovascular intervention would alter outcomes.5–9
We present an overview of the pathophysiology, clinical relevance and prognostic significance of raised troponin in septic critically ill patients.
Methods
We performed a literature search in MEDLINE from its commencement date through the end of May 2014, using medical subject headings and text words, supplemented by scanning the bibliographies of the recovered articles. We combined ‘troponin’ and ‘critical illness’ using the Boolean operator ‘AND’. We used a similar search strategy, using the terms ‘troponin’ and ‘mortality’. We combined these results with the terms ‘critical illness’ and ‘coronary artery disease’. We then combined these results with the terms ‘cardiac troponin’, ‘troponin I’, ‘troponin T’, ‘elevated troponin’, ‘critical illness’, ‘mortality’, ‘intensive care’, ‘sepsis’, ‘severe sepsis’, ‘septic shock’, ‘systemic inflammatory response syndrome’, ‘myocardial injury’, ‘myocardial depression’, ‘acute coronary syndrome’, ‘coronary artery disease’ and ‘ischaemic heart disease’. Language was limited to articles written in English.
VZ and KV reviewed and selected the relevant articles for inclusion. Differences were resolved in consensus meetings. Pre-defined eligibility criteria were used. A study was included if: (1) troponin measurements were performed in adult or paediatric critically ill patients with systemic inflammatory response syndrome, sepsis, severe sepsis or septic shock; (2) it measured troponin in septic ICU patients without coronary artery disease and (3) it evaluated a clinical endpoint (mortality). Randomised controlled trials (RCTs), prospective and retrospective cohorts and case series were eligible for inclusion. Correspondences, experts’ opinions and case reports were excluded. Studies conducted outside the ICU were also excluded. A total of 16 studies met our pre-defined inclusion criteria.
Discussion
Pathophysiology
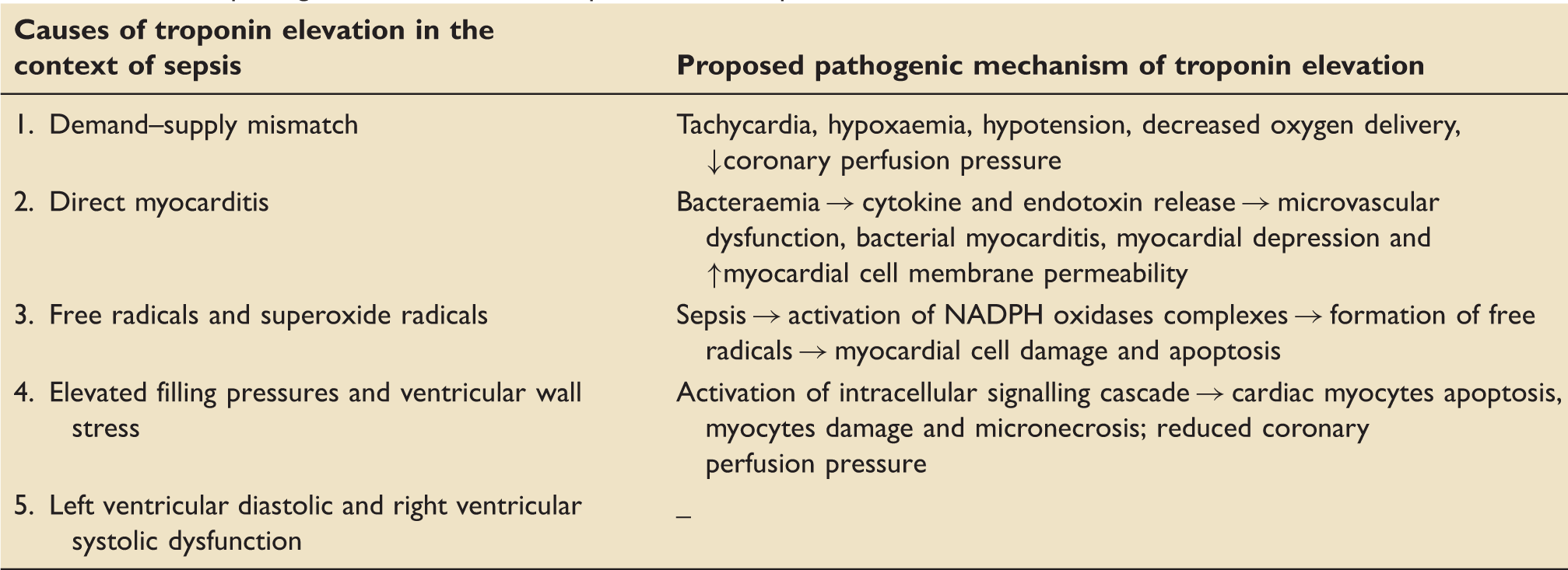
Troponin and cardiac function
Fernandes et al. described a weak correlation between raised troponin levels and left ventricular systolic dysfunction in critically ill patients with sepsis (P = 0.035). 13 Ver Elst et al. also showed that in ICU patients with septic shock, elevated serum troponin was strongly associated with left ventricular dysfunction (in 78% of troponin-positive patients and only 2% of troponin-negative patients), as assessed by transoesophageal echocardiography (P < 0.0001). 14 In the same study, post-mortem examination revealed contraction band necrosis in only 50% of patients with elevated pre-mortem troponin level and in one patient with normal troponin level, indicating that troponin release is most likely related to leakage of troponin from the cardiac myocyte membrane rather than myocyte necrosis. 14 In a study of 37 patients with septic shock, those with positive troponin had higher incidence of regional wall motion abnormalities on echocardiography (56% versus 6%, P = 0.002), lower ejection fraction (46% versus 62%, P = 0.04) and higher mortality (56% versus 24%, P = 0.04) compared to normal troponin patients. 15
Bouhemad et al. associated changes in troponin levels with changes in left ventricular dimensions over time, in surgical intensive care patients with septic shock. When increase in troponin was not associated with significant systolic dysfunction, left ventricular dimensions did not increase. Patients who were found to have ventricular diastolic dysfunction, despite showing no evidence of ventricular dilatation or impaired left ventricular ejection fraction, were identified as having the worst prognosis. 16 In a recent prospective cohort study, Landesberg et al. demonstrated that left ventricular diastolic dysfunction and right ventricular dilatation are the echocardiographic variables correlating best with troponin elevation in general intensive care patients with severe sepsis and septic shock (P = 0.001 and P = 0.0002, respectively). 17
Association between elevated cardiac troponin and CAD (diagnosed by stress echo, coronary angiography or post-mortem examination) in ICU patients with SIRS, severe sepsis or septic shock, without pre-existing CAD.
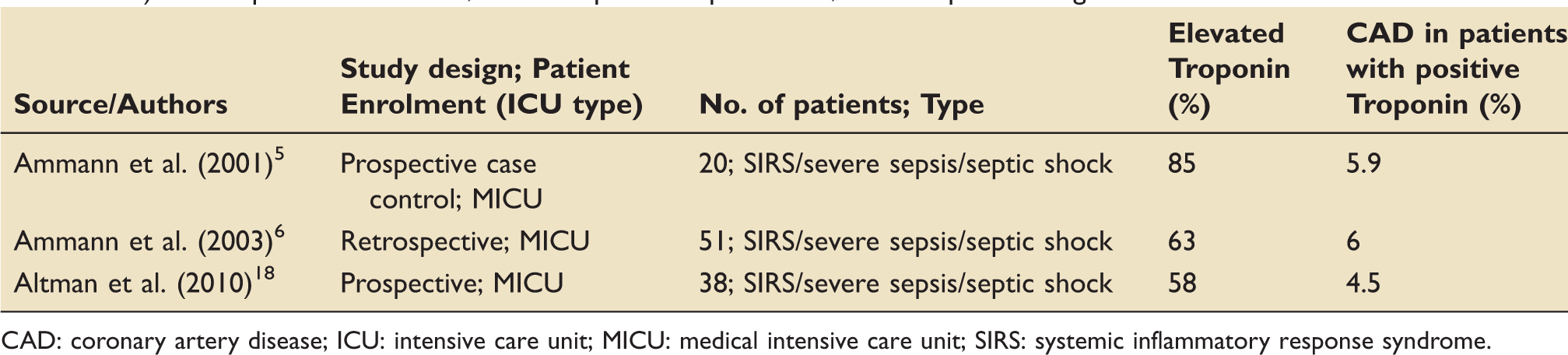
CAD: coronary artery disease; ICU: intensive care unit; MICU: medical intensive care unit; SIRS: systemic inflammatory response syndrome.
Troponin as a prognostic indicator of mortality in clinical sepsis – Evaluating the evidence
Association between elevated cardiac troponin and mortality in ICU patients with sepsis.
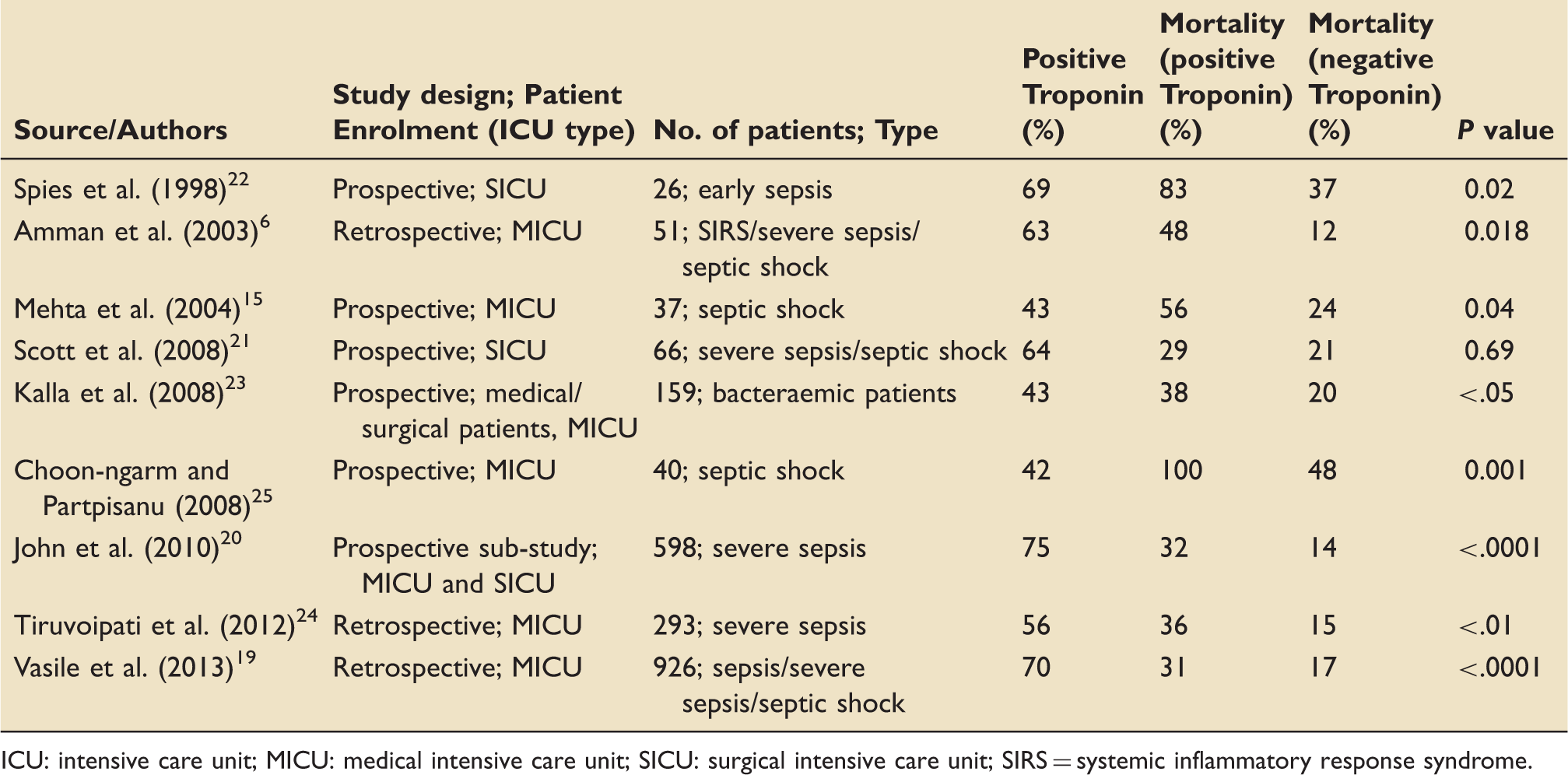
ICU: intensive care unit; MICU: medical intensive care unit; SICU: surgical intensive care unit; SIRS = systemic inflammatory response syndrome.
In a study of 926 critically ill patients with sepsis, 645 (69.7%) patients with elevated cardiac troponin levels had higher 30-day mortality (31% versus 17%, P < .0001), compared with patients with normal troponin levels. 19 After adjustment for severity of disease and baseline characteristics, troponin levels remained associated with 30-day mortality.
John et al. found that in a subset of patients (n = 598), from the Protein C Worldwide Evaluation in Severe Sepsis trial elevated troponin was associated with higher mortality.19,26 Troponin-positive patients had significantly higher 28-day mortality compared with the troponin-negative group (32.2% versus 13.6%, P < .0001). Using multivariable analysis, troponin was an independent prognosticator of mortality (odds ratio: 2.02).
Multivariate analysis – Raised cardiac troponin is not an independent predictor of mortality after adjusting for other variables.
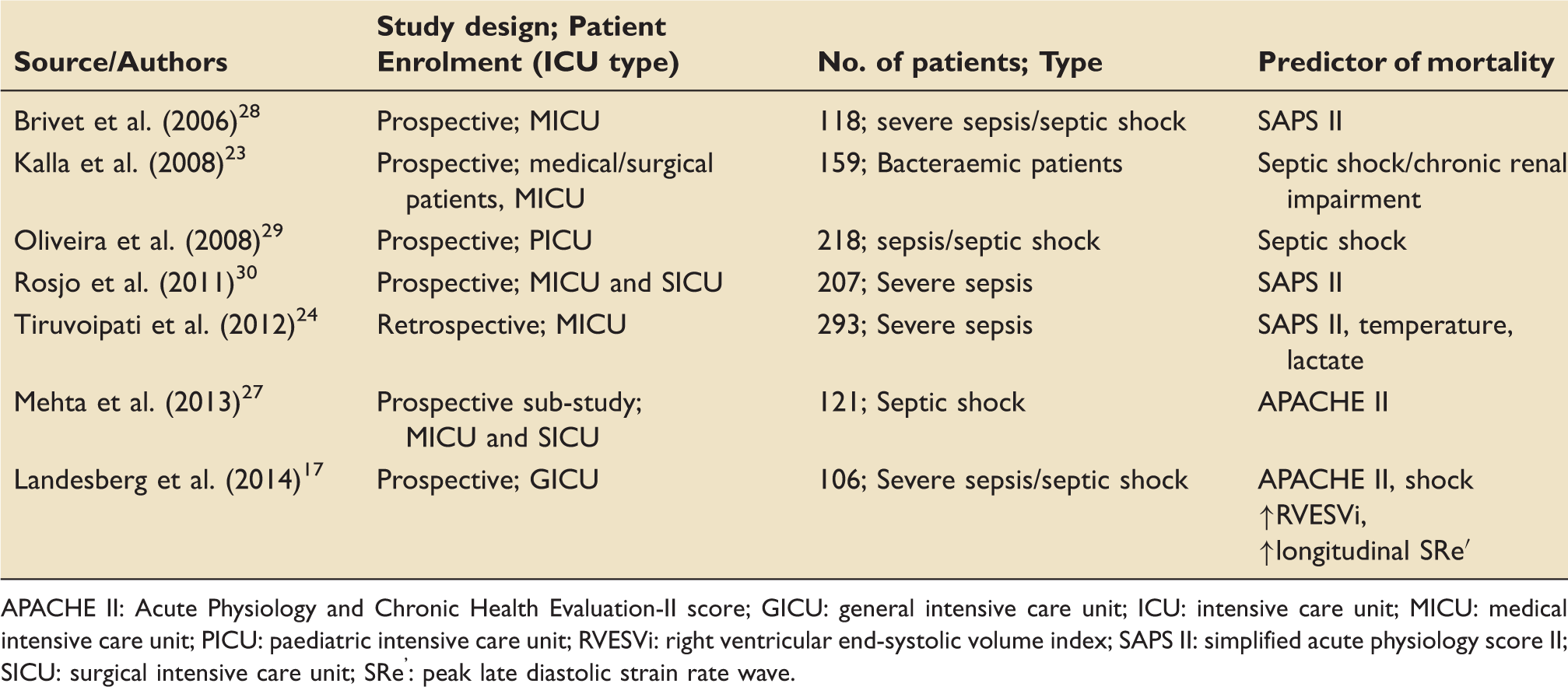
APACHE II: Acute Physiology and Chronic Health Evaluation-II score; GICU: general intensive care unit; ICU: intensive care unit; MICU: medical intensive care unit; PICU: paediatric intensive care unit; RVESVi: right ventricular end-systolic volume index; SAPS II: simplified acute physiology score II; SICU: surgical intensive care unit; SRe’: peak late diastolic strain rate wave.
It is unclear whether raised cardiac troponin has no prognostic value in sepsis or whether differences in timing and frequency of troponin measurement and criteria for positivity in various studies account for these conflicting results. Patient heterogeneity (medical versus surgical patients, patients with varying degrees of sepsis severity, patients requiring varying inotropic/vasopressor medication, undiagnosed coronary artery disease, study population included/excluded patients with coronary artery disease, patients with highest mortality were excluded in some studies) may also play a prominent role.
Most studies were underpowered and although they resulted in statistical significance, they might have overestimated the magnitude of small effects. Finally, the susceptibility of observational studies to selection bias and their inability to control for unknown factors may account for the variation in results, and so explain the heterogeneity.
Elevated troponin: The intensivist approach
A nationwide US survey among 310 intensivists, regarding their treatment strategies for intensive care patients with elevated troponin without typical features of acute coronary syndrome, showed that 76% of intensivists would start either aspirin or clopidogrel, 47.4% would start either low molecular weight heparin or unfractionated heparin, 48.9% would start high dose statins, 68.7% would start beta-blockers and 37.6% would use angiotensin-converting-enzyme inhibitor. In addition, 72.7% of the intensivists said they would request cardiology consultation and 51.3% said they would refer these patients for coronary angiography, once stable. 32 As demonstrated by this survey, a wide variety of opinions exists among intensivists regarding the management of ICU patients with raised troponin, most probably due to lack of relevant guidelines and absence of randomised data on the role of the above agents in such patients. 32
Conclusion
Non-thrombotic troponin elevation is probably multifactorial and a common finding among critically ill patients with sepsis. It might be that myocardial dysfunction accounts for troponin elevation and could potentially explain the troponin’s association with mortality. Alternatively, raised troponin may indicate a more fulminant disease process.
There is no guideline on the appropriate approach and management of septic critically ill patients with elevated troponin. However, vigilance for objective evidence of acute coronary syndrome, prompt management of sepsis and optimisation of myocardial oxygen demand/supply balance are of paramount importance.
Utilisation of cardiac troponins as a sepsis screening tool and addition of troponin to sepsis bundles could be helpful in prognostically stratifying critically ill patients with sepsis, so that early evaluation (by echocardiography or angiography) and management is appropriately initiated. It would stand to reason that septic patients with high pre-test probability of coronary artery disease and very high troponin levels (above 10% of the co-efficient variance) undergo cardiac investigations during their ICU stay. However, we believe that cardiac troponins form one part of a much larger diagnostic, prognostic and therapeutic puzzle.
Adequately powered RCTs are needed to determine the role of therapeutic (antiplatelets, statins, inotropes, etc.) and diagnostic (echocardiography, coronary angiography) strategies in an intensive care patient population with sepsis and positive troponin results, and whether these patients should have formal cardiac investigations once they recover from their critical illness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.