
Abstract
Purpose
Systolic impairment is well reported in critically ill patients but diastolic function has been relatively understudied. The objective of this review was to assess tissue Doppler indices of diastolic function in critically ill patients along with any association with mortality.
Methods
A systematic review of articles in English using Medline, EMBASE, CINAHL and the Cochrane database of systematic reviews. Search terms included diastolic function, diastolic dysfunction, diastolic abnormal*, diastolic heart failure, diastolic filling, ventricular relaxation, pulmonary artery occlusion pressure, left ventricular filling pressure, cardiac dysfunction, intensive care, critical care, critically ill, critical illness, sepsis and septic shock. Only studies of critically ill adult patients (excluding post-cardiac surgical patients) whose diastolic function was assessed using tissue Doppler imaging were included. Study quality was assessed using a modified version of the Newcastle–Ottawa Scale (NOS).
Results
Nineteen studies were included, with a total of 1365 patients. All trials were observational. There was a large heterogeneity in patient populations and the methodology of tissue Doppler assessment of diastology resulting in a descriptive analysis. Patient groups included severe sepsis or septic shock (5 studies), septic shock (5 studies), systemic inflammatory response syndrome and shock (1 study), septic shock and acute lung injury (1 study), cancer and septic shock (2 studies), general ICU patients (1 study), combined medical and surgical ICU (2 studies) and sub-arachnoid haemorrhage patients (2 studies). Seventeen studies scored 5/6 on the NOS with the remaining two scoring 4/6. Fourteen studies reported on numbers of patients diagnosed with diastolic dysfunction (500/999, mean 50%, range 20–92%). Three studies found that diastolic dysfunction was an independent predictor of mortality.
Conclusions
Current data shows a large range in the incidence of diastolic dysfunction in this patient population and a variable link with mortality. Future research should focus on the definition of normal values for diastolic function in critically ill patients along with the effects of ICU therapies and consensus criteria for its assessment in this patient population.
Introduction
Maclean et al. 1 published a landmark study in 1967 on the early haemodynamic clinical course of patients with septic shock. They identified a group of patients with a low cardiac output, high peripheral vascular resistance and cold cyanotic extremities that had an associated high mortality. Since then clinical interest in heart failure in critically ill patients has focused on systolic dysfunction.
Parker et al. 2 showed that left ventricular (LV) systolic impairment was present in half of patients with septic shock. More modern imaging modalities have revealed an incidence of just over two-thirds. 3 Diastolic dysfunction in critically ill patients has been relatively under-investigated which is surprising given its significant haemodynamic consequences.
Diastole is the time period during which the myocardium loses its ability to generate force and returns to an unstressed pressure and myocyte length. In health left ventricular relaxation creates a suction effect that promotes filling from the left atrium. As diastolic function worsens this pressure gradient falls and is eventually reversed, with a compensatory rise in left atrial (and hence left ventricular filling) pressure to maintain ventricular filling.
Assessment of diastolic function in health uses tissue Doppler imaging to measure the velocity of relaxation of the left ventricular myocardium (e′). The diagnosis is refined by integrating qualitative and quantitative measures of left ventricular filling pressures as they are directly related with diastolic function in health, 4 grading function as normal or impaired (Grades I–III). This is performed by assessing the ratio of blood flow across the mitral valve during early passive left ventricular filling (E) and atrial contraction (A), the E/A ratio. Additional measure include the ratio of blood flow through the pulmonary veins into the left atrium during systole (S) and diastole (D), the S/D ratio, along with left atrial size.
Assessment of diastolic function in critically ill patients differs as the severity of pathologies (such as sepsis, hypoxia and acidosis), changes in intravascular status (from intravenous fluid therapy, capillary leak syndrome, renal replacement therapies) and the large variety of treatments (such as sedatives, vasopressors, inotropes and positive pressure ventilation) result in constant fluctuations in the loading conditions of the heart, affecting most of the qualitative and quantitative methods for the measurement of left ventricular filling pressures. 4
Tissue Doppler has been validated as a relatively preload and afterload-independent measure of left ventricular relaxation, especially when it is measured at the lateral annulus. 5 It is not completely load independent 6 and is affected by many ICU therapies including the lusitropic effects of vasoactive drugs and fluid loading. Normal minimum relaxation values are 8 cm/s at the septal mitral annulus and 10 cm/s at the lateral mitral annulus, or an average of 9 cm/s. 7 Values below these thresholds suggest diastolic dysfunction in outpatients – the normal minimum values in critically ill patients is yet to be determined.
Historically the burden of disease of heart failure in the general population was attributed to systolic heart failure, but in recent years the diagnosis of diastolic heart failure has increased. 8 Diastolic heart failure has a significant incidence and associated morbidity in outpatient populations, but has been relatively understudied in the critically ill. This is an area of importance as approximately one third of heart failure patients have little evidence of systolic failure. 8 However, when they are hospitalised with heart failure their 1-year and 5-year survival rates are the same, or only slightly better than patients with systolic heart failure. 9
The aims of this review were to assess observational echocardiographic studies performed in critically ill adult patients that assessed diastolic function and/or the incidence of diastolic dysfunction, using tissue Doppler indices and to determine whether there was any association with mortality.
Methods
Study eligibility
Observational studies that used tissue Doppler echocardiography to assess diastolic function in critically ill adult patients were considered. Outcome measures were diastolic function or incidence of diastolic dysfunction, and/or a mortality association with diastolic function/diastolic dysfunction. Paediatric studies, animal studies, studies of patients post cardiac surgery and non-echocardiographic studies were excluded.
Literature search
We performed an electronic literature search on 21 August 2014 using Medline, EMBASE, CINAHL and the Cochrane database of systematic reviews. The search terms used were ((diastolic function) OR (diastolic dysfunction) OR (diastolic abnormal*) OR (diastolic heart failure) OR (diastolic filling) OR (ventricular relaxation) OR (pulmonary artery occlusion pressure) OR (left ventricular filling pressure) OR (cardiac dysfunction)) AND ((intensive care) OR (critical care) OR (critically ill) OR (critical illness) OR (sepsis) OR (septic shock)). The search was limited to studies in the English language. No publication date or publication status restrictions were imposed.
Study selection
Only studies that assessed diastolic function using tissue Doppler were included.
Data items
Information was extracted from each study on: (1) number and character of trial participants; (2) study type; (3) method of echocardiographic assessment of diastolic function; (4) incidence of diastolic dysfunction/qualitative assessment of diastolic function; (5) mortality association (if any) with diastolic dysfunction.
Statistical analysis
The studies varied in their methods of tissue Doppler assessment of diastolic function and had a large heterogeneity in their patient populations. Analysis was therefore descriptive.
Quality assessment
There is no current consensus for assessing the quality and susceptibility to bias of observational studies. The Newcastle–Ottawa Scale (NOS) score has been endorsed by the Cochrane Collaboration for assessing the quality of non-randomised studies included in a systematic review.
10
For this review we used a modified version of the NOS based on two major study components – selection of study groups (0–3 points), and ascertainment of exposure (0–3 points) (Figure 1). A higher overall score indicates a better methodological quality.
Modified Newcastle–Ottawa quality assessment scale for cohort studies.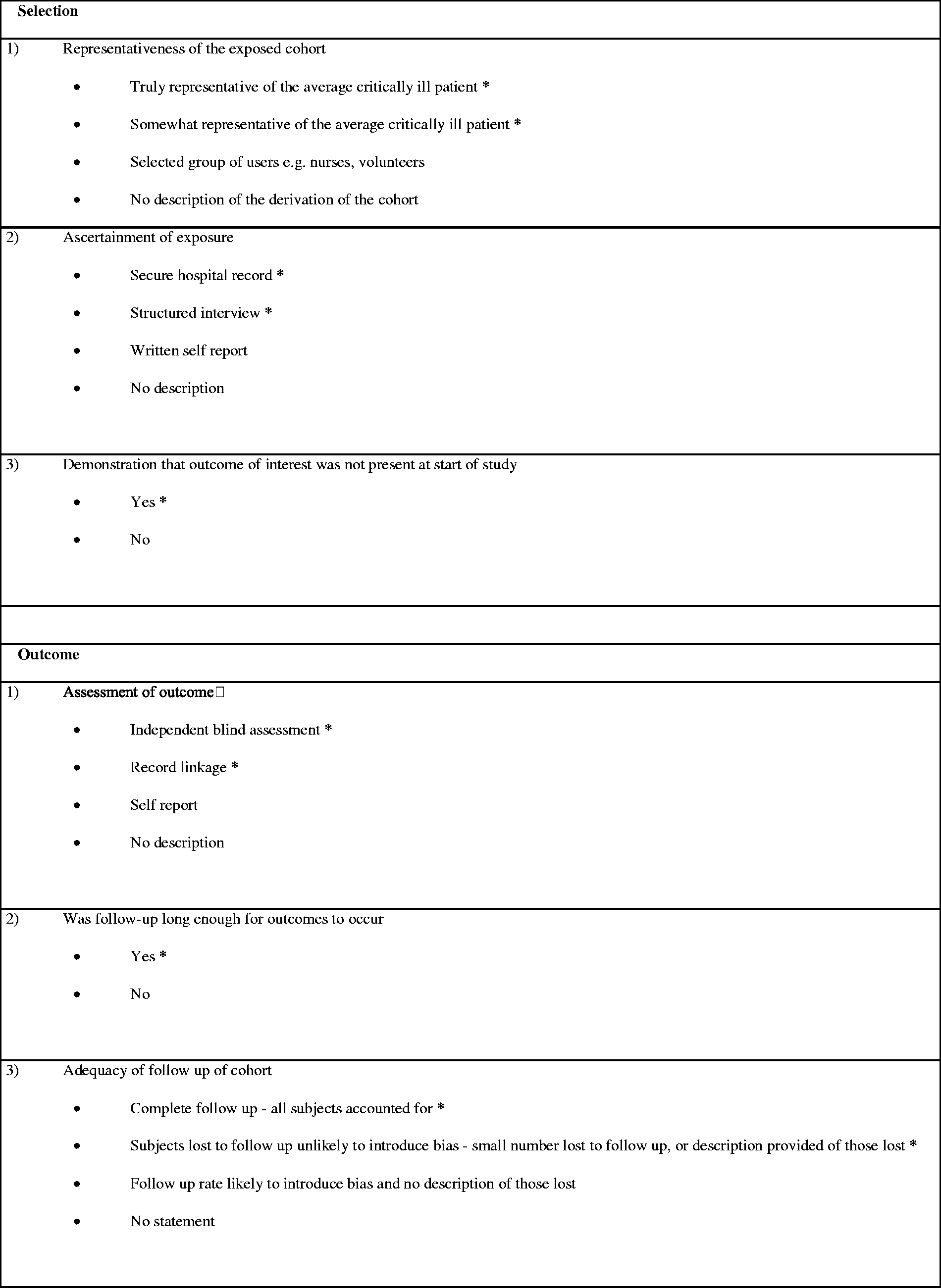
Results
The search of Medline, EMBASE, CINAHL and the Cochrane database of systematic reviews resulted in a total of 872 potential citations. Of these, 810 were excluded as they did not meet the criteria. A further 32 were excluded after reviewing the abstracts. The full text of the remaining 30 citations was examined in more detail. Eleven citations did not meet the inclusion criteria described above, leaving 19 studies for inclusion in the final review. No further studies were identified by checking the references, and no unpublished further relevant studies were obtained. These results are summarised in Figure 2.
Citation filtering process.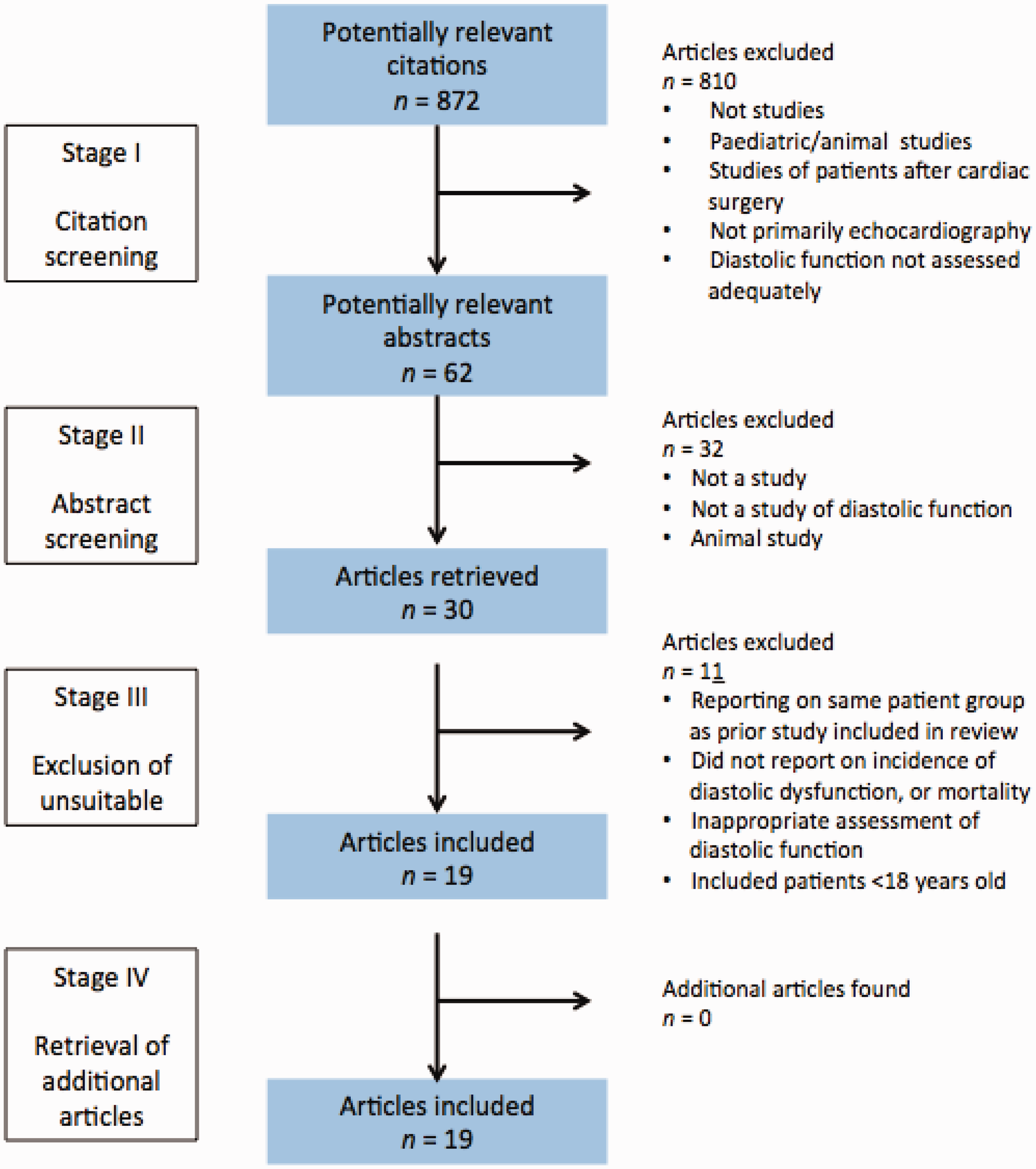
Major features of studies included in the analysis.

Patients from general ICUs/combined medical and surgical ICUs,13,19,25 with subarachnoid haemorrhage,20,21 patients with systemic inflammatory response syndrome (SIRS)/shock/sepsis/septic shock12,14–18,22,23,26–29 and patients with cancer and septic shock11,24 were included in the studies selected. Seventeen studies were prospective11–24,26,28,29 and two were retrospective.25,27
Thirteen studies examined on incidence of patients on mechanical ventilation11,12,14–20,23–26 with a reported range of 39–100%. All studies used tissue Doppler imaging to assess diastolic function. Thirteen studies assessed diastology in a dichotomous fashion11,13,16–19,22–26,28,29 (normal diastolic function/presence of diastolic dysfunction), five studies reported diastolic function as mean/median tissue Doppler velocities14,15,20,21,27 and one study did not assess diastolic function in a dichotomous fashion or report it as mean/median Doppler velocity. 12 Ten studies looked for an association between diastolic function and mortality.11,12,14–16,19,23–25,29 Quality assessment using the modified NOS scale resulted in 17 studies scoring 5/6, the remaining 2 studies scored 4/6. All studies failed to demonstrate that the outcome of interest (impaired diastolic function/diastolic dysfunction) was not present at the start of the study.
There was a large heterogeneity across the studies for the echocardiographic cutoff values used for the diagnosis of diastolic dysfunction. Two studies used a lateral e′ < 12,17,22 two studies used a septal e′ < 9.6,18,25 one study used a mean e′ < 9, 13 one study used a lateral e′ < 8.5, 23 two studies used a mean e′ < 8,16,29 one study used a septal e′ < 8 28 and one study used a lateral e′ < 8. 11 The other studies used composite measures – one study used a lateral e′ < 10 and E/A < 1, 26 one study used a mean e′ < 8 and/or a mean E/e′ > 13 19 and one study used a lateral e′ < 8 and/or an E/e′ > 8. 24 Due to this heterogeneity the results were not meta-analysed. We have focused on describing the studies, their results, applicability and limitations.
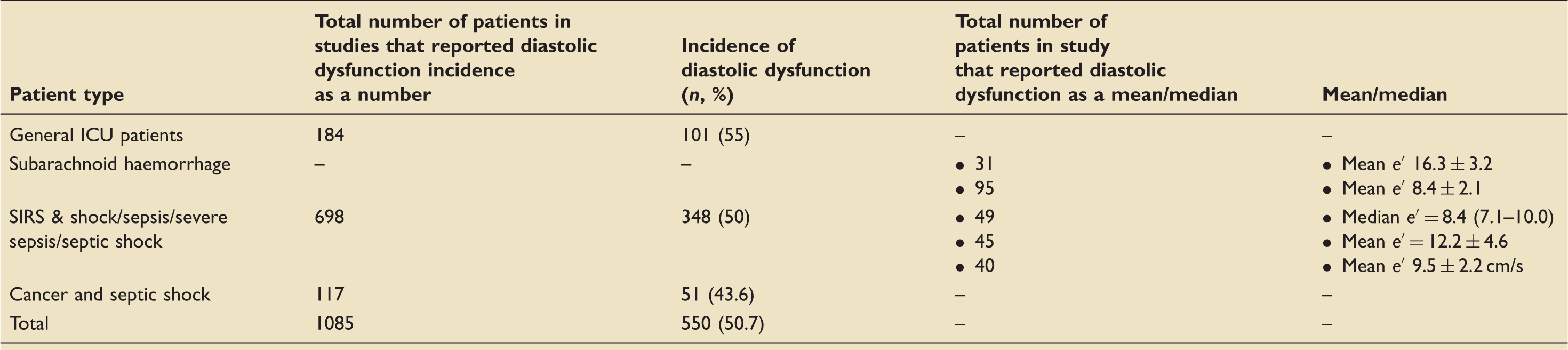
Incidence of diastolic dysfunction
Incidence of diastolic dysfunction/mean and median values of diastolic function.
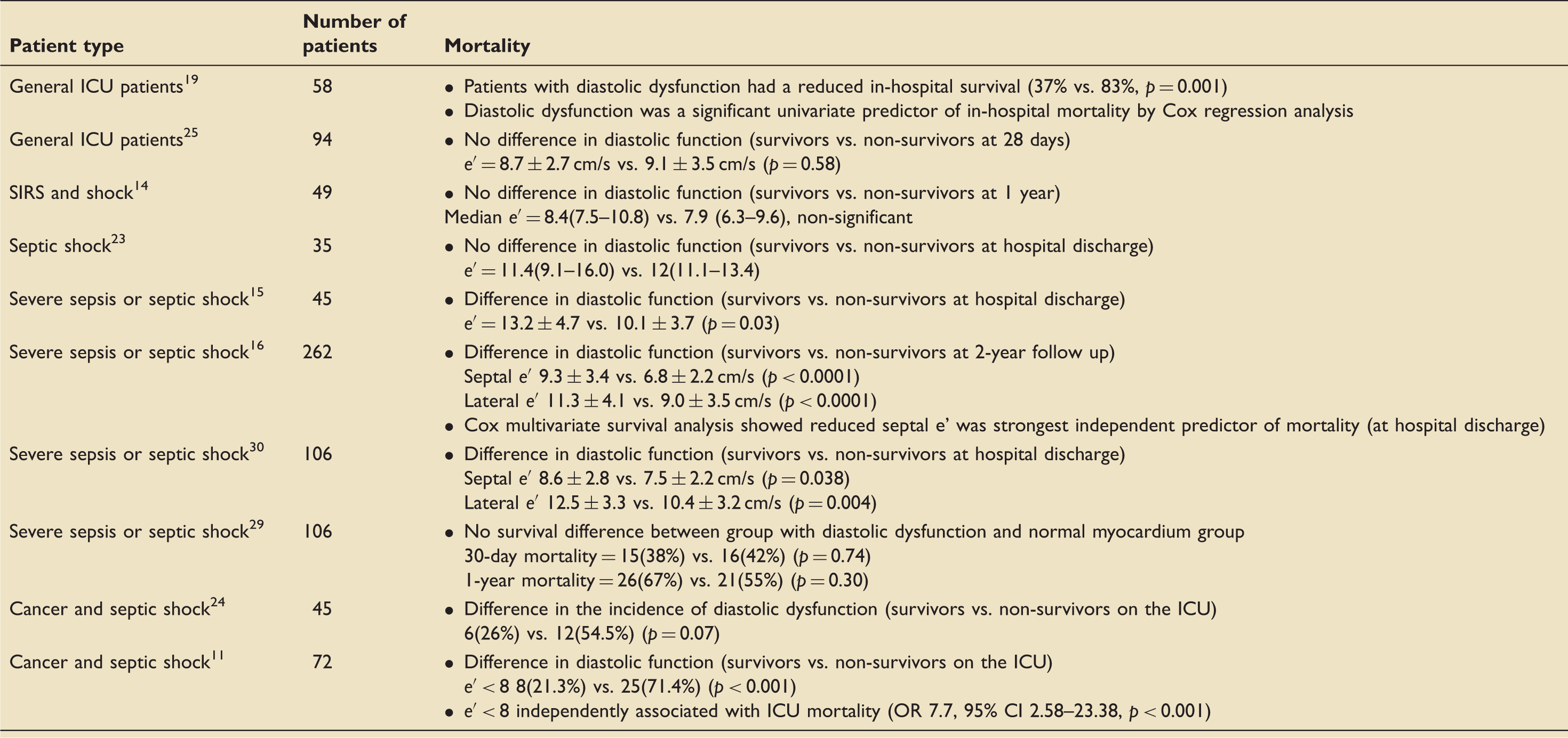
Association with mortality
Association of diastolic dysfunction with mortality.
Discussion
Assessment of diastolic function in critically ill patients is challenging. Most of the traditional echocardiographic indices are affected by the loading conditions of the heart that are constantly changing in critically ill patients as a result of the illness, organ failures, supportive therapies and treatments. This review only included studies that used tissue Doppler imaging. It is a relatively preload and afterload-independent measure but is still affected by many common therapies such as fluid loading and vasoactive drugs. The 19 studies included in this review show a large heterogeneity in their patient populations and the methodology of tissue Doppler assessment of diastolic function. This is reflected in the large range of the incidence of diastolic dysfunction of 20–92%.
Only three of the studies found that diastolic dysfunction was an independent predictor of mortality. Six of the 10 studies found an association between impaired diastology during critical illness and mortality and one study found an inverse association. There was a large variability in the timings of the echocardiograms during the critical illness and some studies used hospital discharge data making it difficult to ascertain whether diastolic dysfunction persisted beyond ICU discharge and whether it was linked to post ICU mortality.
The mean incidence of diastolic dysfunction in this review is identical to the historical incidence of systolic dysfunction in patients with severe sepsis/septic shock (50%). 2 However, newer imaging modalities such as speckle tracking have revealed that the incidence of systolic dysfunction in this patient population is higher at just over two-thirds. 3 Application of these more sensitive techniques could potentially reveal an increased prevalence of diastolic dysfunction in critical illness.
Our review has several limitations. There is no current consensus for assessing the quality and susceptibility to bias of observational studies (a recent systematic review identified 86 tools 31 ). A pragmatic approach was used for the assessment of the quality of the 19 studies included in this review. None of the studies specifically quantified diastolic function in patients prior to ICU admission. Systematic pre-ICU echocardiographic assessment would, however, be difficult as critical illness is usually an unforeseen event. Several studies declared no prior history of heart failure, and most studies excluded patients with known heart disease, coronary artery disease or valvular disease. Another limitation was a lack of consistency within and between the 19 studies for the timing of the echocardiograms during the patient’s ICU stay.
Many of the studies used different tissue Doppler cutoff values for the diagnosis of diastolic dysfunction. This is likely as a result of historical changes in consensus guidelines used for the assessment of diastolic function, 4 coupled with a changing evidence base for the application of these values in critically ill patients. Although tissue Doppler imaging is the current echocardiographic gold standard for assessing diastolic function in critically ill patients, it is not completely load independent 6 and is notably affected by vasoactive drugs that are very commonly used in this patient population. Additionally normal values for diastolic function have not yet been defined in this patient population.
We only included studies that used tissue Doppler for the assessment of diastolic function, but we allowed several studies that used composite measures that include assessment of the pulmonary capillary wedge pressure (PCWP) to assess diastolic function. One study used a mean e′ < 8 and/or a mean E/e′ > 13, and another study used a lateral e′ < 8 and/or an E/e′ > 8. The E/e′ ratio has been shown to correlate with the PCWP in critically ill patients. 32 The addition of the E/A ratio to the tissue Doppler velocity is unnecessary, and could also have led to an underestimation of the incidence of diastolic function in this study.
Conclusions
This review found an incidence of diastolic dysfunction using tissue Doppler imaging of 20–92% in 1365 patients. Three studies found that diastolic dysfunction is an independent predictor of mortality in this patient population but this must be interpreted in the context of the high heterogeneity of the studies combined with the as yet unquantified effects of ICU therapies on tissue Doppler imaging. Future research should focus on the definition of normal values for diastolic function in critically ill patients, the effects of ICU therapies and consensus criteria for its assessment in this patient population. The results could inform interventional studies looking at preventative measures and potential treatments.
Footnotes
Acknowledgements
We would like to thank Dr Payashi Garry for reviewing the manuscript and Dr Stuart McKechnie for statistical advice.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.