
Abstract
Introduction
The relationship between socioeconomic status and various components of health is well established. Research has also highlighted that social deprivation can affect patterns of injury and outcome after trauma. The interaction between outcomes following blunt chest trauma and socioeconomic status has received limited attention in trauma research. The aim of this study was to investigate the relationship between socioeconomic factors, mechanisms of injury and outcomes following blunt chest trauma using deprivation measures calculated on the basis of domicile postcodes.
Methods
A retrospective study design was used in order to examine the medical notes of all blunt chest wall trauma patients who presented to the ED of a large regional trauma centre in South West Wales in 2012 and 2013. Baseline characteristics were presented as median and interquartile range or numbers and percentages. Differences between the baseline characteristics were analysed using Mann–Whitney U test and Fisher’s exact test. Odds ratios and 95% confidence intervals were presented from the univariable analysis. Multivariable logistic regression analysis was used to identify significant predictors for the development of complications.
Results
Patients in the ‘more deprived’ group were more likely to be the victims of assault (p < 0.001) and were more likely to have an unplanned re-attendance at the Emergency Department than the patients in the ‘less deprived’ group (p < 0.001). On multivariable analysis, social deprivation was not a risk factor for the development of complications, but it was a significant risk factor for prolonged length of stay (p < 0.05).
Conclusions
This is the first study in which social deprivation has been investigated as a risk factor for complications following isolated blunt chest wall trauma. Residing in a ‘more deprived’ area in South West Wales is not associated with the development of complications following isolated blunt chest wall trauma.
Introduction
Social deprivation has been defined as the lack of access to opportunities and resources which we might expect in our society. 1 The relationship between socioeconomic status and various components of health is well established.2–4 Research has also highlighted that social deprivation can affect patterns of injury and outcome after trauma.5,6 There is a strong relationship between social deprivation and the incidence of injury, and evidence suggests that the disadvantaged are less likely to survive.2–6 Higher crime rates and alcoholism associated with deprived areas may result in increased incidence of trauma. Previous research has suggested that deprivation may be a risk factor for poorer outcomes due to the association with smoking, extremes of body mass index or diabetes, financial hardship and homelessness.2,3
The interaction between outcomes following blunt chest trauma and socioeconomic status has received limited attention in trauma research. Mortality rates in blunt chest wall trauma have been reported to range between 5.7% 7 and 18.7%. 8 It has been estimated that the annual lost economic output from deaths and serious injuries from major trauma in the UK is between £3.3 billion and £3.7 billion. 9 An understanding of the impact of socioeconomic factors on blunt chest trauma could potentially benefit health care providers and improve targeting of preventive strategies.
In a recent American study by Barrett-Connor et al. (2010), no significant differences were reported in traumatic rib fracture according to race/ethnicity, marital status, education, self-reported overall health, depressed mood, alcohol use, cigarette smoking and physical activity. 10 In a study investigating rib fractures in alcoholic men, however, a statistically significant association was reported between rib fractures and disruption of social and familial links, irregular feeding habits (in bars or pubs, not at home), ethanol consumption by close relatives and intensity of tobacco consumption. 11 Research has highlighted that rib fractures are common among heavy alcoholics.11,12 Their presence is related closely to nutritional status, lean mass and vitamin D levels. 12 As a result of the lack of agreement in the research, the aim of this study was to investigate the relationship between socioeconomic factors, mechanisms of injury and outcomes following blunt chest trauma using deprivation measures calculated on the basis of domicile postcodes.
Methods
Setting and sample
A retrospective study design was used in order to examine the medical notes of all blunt chest wall trauma patients who presented to the Emergency Department (ED) of a large regional trauma centre in South West Wales (Morriston Hospital) in 2012 and 2013. Morriston hospital has approximately 90,000 presentations to the ED per year and serves a population of 450,000 people. Those patients coded as ‘blunt chest trauma’ or ‘rib fractures’ were identified using the hospital database. Morriston Hospital does not currently use ICD codes in the ED so patients were retrieved from the database using general codes (injury, fracture, chest, thorax) and then patients who did not meet the inclusion criteria were excluded following examination of their medical notes. Patients with any significant concurrent injuries were excluded. Patients aged 16 or more were included in the study.
Data collection
The patient’s postcode, age, sex, injury mechanism, number of rib fractures and history of chronic lung disease were all identified from the medical notes. The number of rib fractures was determined by the clinical notes however in the cases where the number of rib fractures could not be determined using the clinical records, then the X-ray report was reviewed by the investigators. The development of complications during the recovery phase following blunt chest wall trauma was the composite outcome measure investigated in this study. Data collection for this outcome was completed from the time the patient presented to the ED through to discharge from hospital. Patients were reported to have developed complications if one or more of the following were documented in their medical records; in-hospital mortality, morbidity including all pulmonary complications (chest infection, pneumonia, haemothorax, pneumothorax, pleural effusion, or empyema), ICU admission, an unplanned representation to the ED or a prolonged length of stay as defined as a total hospital stay of seven or more days.
The medical notes were reviewed following guidelines suggested in a study by Gilbert et al (1996). 13 The ED medical notes of all patients presenting to the ED of Morriston Hospital in 2012 and 2013 were examined and data recorded on a pre-designed database. A validation check was completed in which an additional researcher checked the accuracy of data input for 10% of all patients, in order to reduce information bias. If a patient’s notes had missing or incomplete data for the variables under investigation, they were still included in the database. The dataset was also stored on a hospital encrypted computer to ensure data security (Safe-end protector encryption).
Deprivation scores
Domicile postcodes were recorded from the medical notes. On the basis of this postcode, the patients were assigned a deprivation code using the Welsh Index of Multiple Deprivation, 2011 (WIMD). 1 The WIMD is the official measure of relative deprivation for small areas in Wales produced by the Welsh government and was developed as a tool to identify and understand deprivation in Wales. Eight domains of deprivation are included: employment, income, education, health, community safety, geographical access to services, housing and physical environment. Each domain is made up of a number of indicators and there are 35 indicators in total that compromise the WIMD 2011.
The income domain indicator has the highest weighting (23%) for the overall WIMD score and was used as a marker of deprivation in this study for a number of reasons. In contrast to the WIMD code (which is a relative score), the income domain indicator is an absolute score which provides the percentage of those living in the area receiving income related benefits. It has an extremely high correlation with the overall deprivation index. 1 Using the WIMD code, each patient was assigned the corresponding income domain indicator score and this was used as an absolute measure of deprivation in the analysis. In order to analyse whether there were any differences in patient demographics, injury mechanisms and outcomes, patients were classified as ‘more deprived’ if their income domain indicator score was 22% or more and ‘less deprived’ if their score was 21% or less. This cut-off value corresponds to the top 30% of the most deprived areas in Wales. 14
Data analysis
Baseline characteristics were presented as median and 25th and 75th interquartile range (due to non-normal distributions) for the continuous variables, and numbers and percentages for categorical variables. Differences between the baseline characteristics were analysed using Mann–Whitney U test (continuous variables) and Fisher’s exact test (categorical variables). Odds ratios and 95% confidence intervals were presented from the univariable analysis. All prognostic variables were included in the final analysis. Multivariable logistic regression analysis (with fractional polynomials used to model the continuous variables) was used to identify significant predictors using the Likelihood test statistic. There was less than 1% missing data and therefore we used a simple imputation of the mean method to avoid exclusion of patients from the final analysis. 15
Ethical approval
The South West Wales Research and Ethics Committee confirmed that ethical approval was not required for this study and also waived the need to obtain written informed consent from the patients. All patient information was anonymised and de-identified prior to analysis.
Results
Patients’ demographics, injury mechanisms and complication rates.
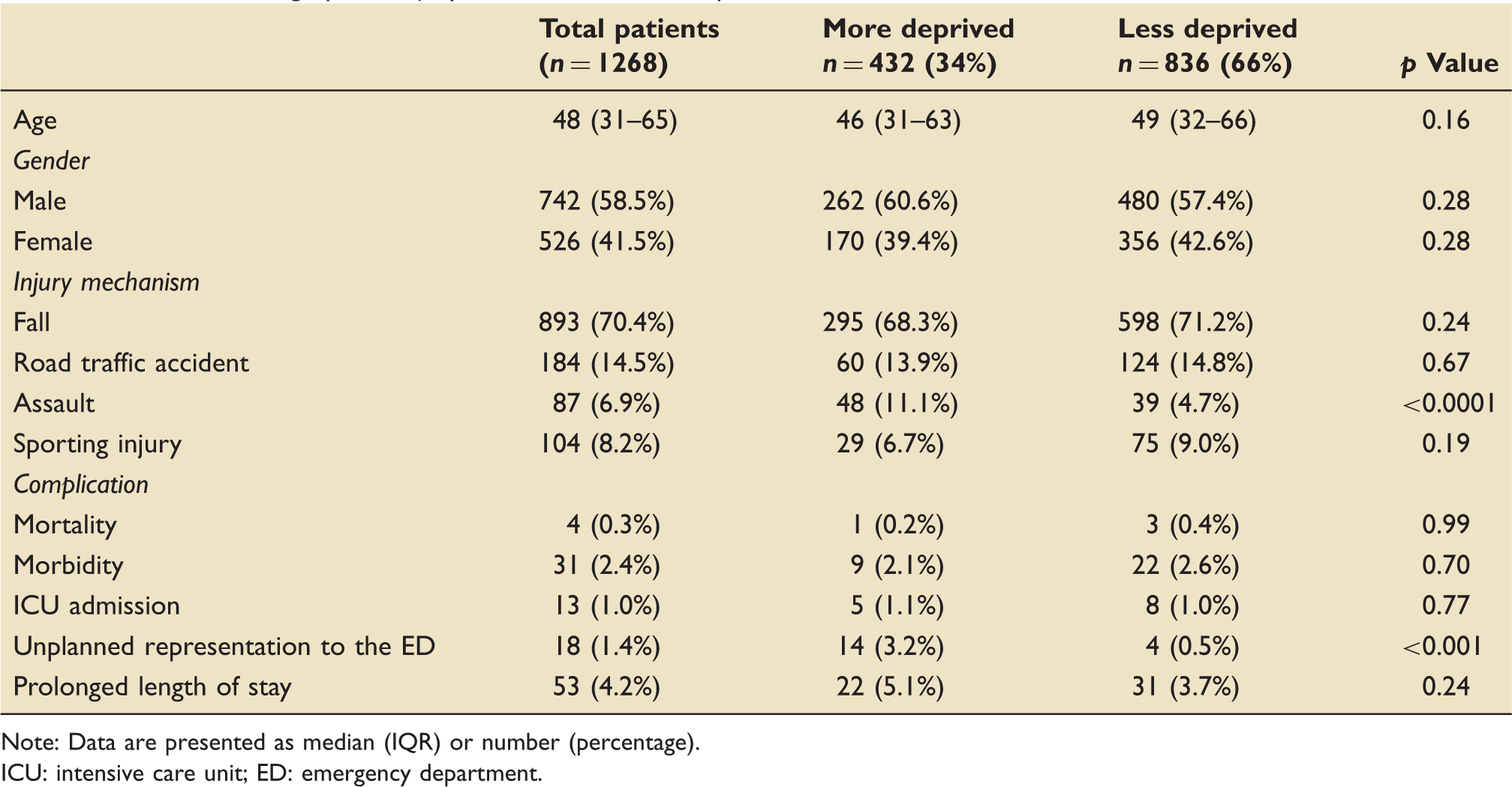
Note: Data are presented as median (IQR) or number (percentage).
ICU: intensive care unit; ED: emergency department.
Results of univariable analysis.
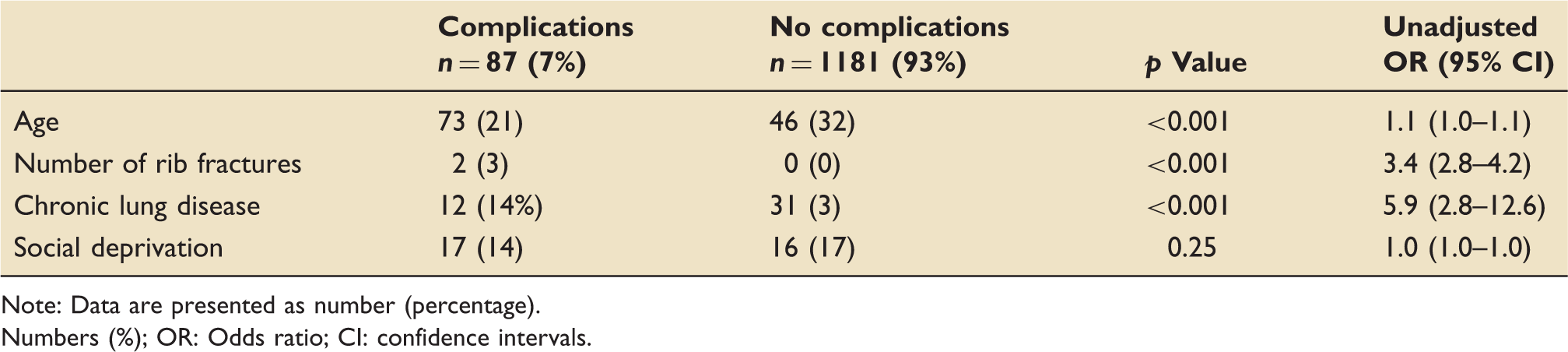
Note: Data are presented as number (percentage).
Numbers (%); OR: Odds ratio; CI: confidence intervals.
Risk factors and their adjusted odds ratios for the development of complications following blunt chest wall trauma.
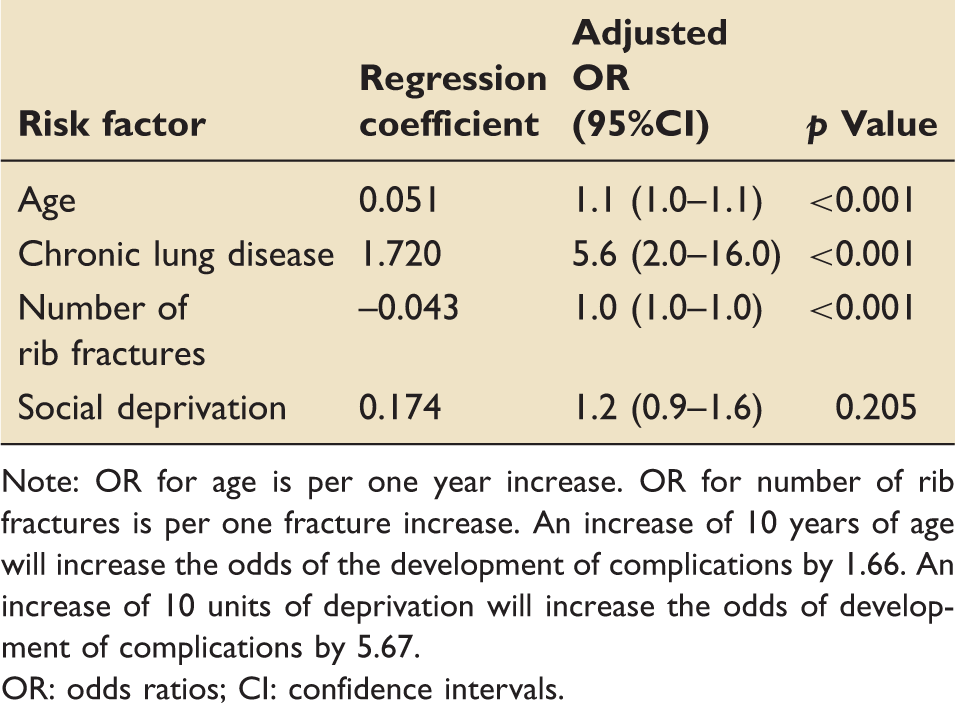
Note: OR for age is per one year increase. OR for number of rib fractures is per one fracture increase. An increase of 10 years of age will increase the odds of the development of complications by 1.66. An increase of 10 units of deprivation will increase the odds of development of complications by 5.67.
OR: odds ratios; CI: confidence intervals.
Risk factors and their adjusted odds ratios for prolonged length of stay following blunt chest wall trauma.
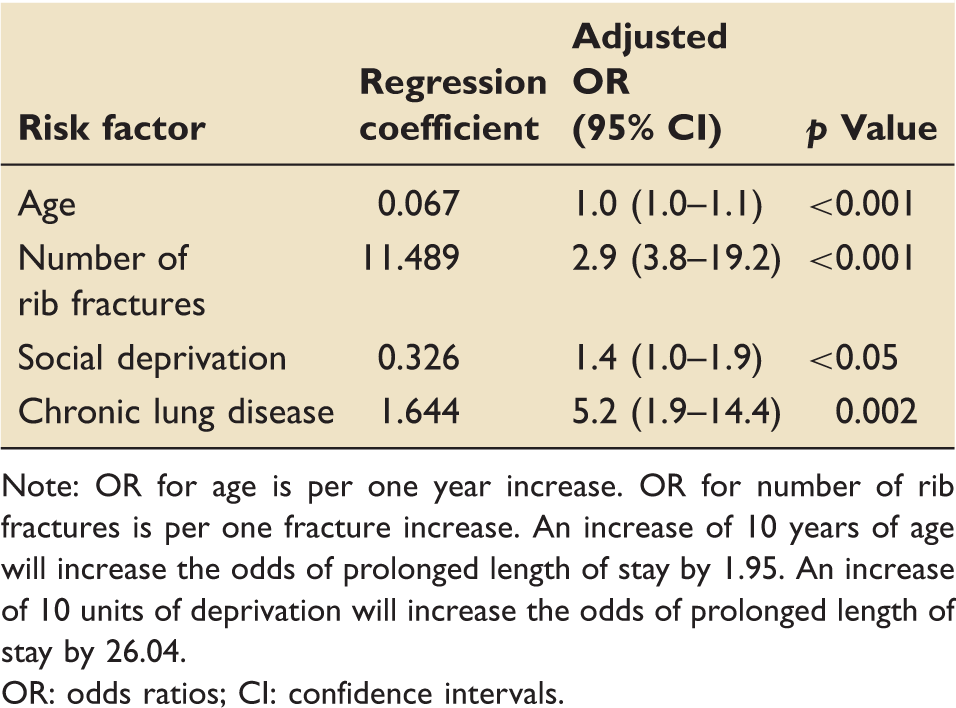
Note: OR for age is per one year increase. OR for number of rib fractures is per one fracture increase. An increase of 10 years of age will increase the odds of prolonged length of stay by 1.95. An increase of 10 units of deprivation will increase the odds of prolonged length of stay by 26.04.
OR: odds ratios; CI: confidence intervals.
Discussion
The aim of this study was to investigate the relationship between social deprivation and isolated blunt chest trauma in South West Wales. After adjusting for other recognised predictors, we have not found any evidence to suggest that social deprivation is an independent predictor of the development of complications following isolated blunt chest trauma. Age, chronic lung disease and number of rib fractures were all reported to be predictors of the development of complications and this supports the findings of previous research. 16 It was also found that isolated blunt chest trauma patients from a more deprived area did not sustain more severe injuries than those from a less-deprived area. These results support the findings of Barrett-Connor et al. who also reported that no significant differences existed in traumatic rib fracture according to race/ethnicity, marital status, education, self-reported overall health, depressed mood, alcohol use, cigarette smoking and physical activity. 10
This study highlighted that patients in the ‘more deprived’ group were significantly more likely to be the victim of assault resulting in isolated blunt chest trauma, than patients in the ‘less deprived’ group. This finding supports Dunn et al. who reported that head injured patients in the ‘more deprived’ group were more likely to sustain their injury as a result of assault. 6 They also reported that the patients in the less-deprived group were more likely to be in a road traffic accident or to have fallen from a height; however, the results of this study found no significant difference in any other injury mechanism. This may be due to the different injured body part under investigation. It could be suggested that the increased risk of assault in the more deprived group is due to increased rates of unemployment and alcoholism; however, further research would be needed to investigate the causes for the differences in injury mechanism.
Isolated blunt chest trauma patients residing in a more deprived area in this study were significantly more likely to have an unplanned representation to the ED than patients from a less deprived area. Unplanned representation at an ED has recently been added as a clinical quality indicator in English hospitals by the Department of Health and the rate should range between 1% and 5%. 17 The causes of unplanned representation have been investigated previously in trauma research and include persistent pain following an injury, 18 older age 19 and not being married. 20 Social circumstances have been previously identified as a predictor of repeated re-attendance at EDs.21,22 In the study by Lynch et al., 85% of re-attenders were single and 7.5% of no fixed abode. 21 We are unable to compare our results as we did not collect data on marital status. Further research is needed to identify the causes of ‘more deprived’ patients having a significantly higher recorded incidence of unplanned representations to the ED, as this improve clinicians’ understanding of how to reduce these representations.
Social deprivation was found to be a significant predictor for a prolonged length of stay following isolated blunt chest wall trauma. This result does not support the results of Dunn et al. who reported that head-injured trauma patients from a more deprived area had shorter median length of stay than the head-injured patients from a less-deprived area; however, this may again reflect the difference in body part injured. 6 It could be suggested that the increased incidence of prolonged length in the ‘more deprived’ group of patients is due to a number of factors including higher rates of alcoholism and smoking, but further research in this area would be needed to draw firm conclusions. As a result of the risk of prolonged length of stay in the more deprived isolated blunt chest wall trauma patient, the clinician managing the patient should consider the patient’s social status when planning for hospital discharge.
This study has a number of limitations. One potential limitation of the study is that polytrauma patients were excluded, so the results are only generalisable to isolated blunt chest wall trauma patients. As a result of the study design and the inherent nature of patients, a number of the independent variables investigated were potentially interdependent and an increase in one variable inadvertently leads to an increase in another. Multivariable logistic regression was used in an attempt to address this issue of collinearity. It is also possible that a confounding variable that influences the results was not considered in the data collection or analysis. It could therefore be suggested that the discovered association between social deprivation and prolonged length of stay is the result of both risk factor and outcome being related to common underlying unmeasured pathologies of some kind such as alcoholism. In prognostic clinical research, however, this is difficult to overcome due to the nature of the study population and therefore the results of the study should be interpreted with this in mind.
The use of the database to identify the patients for inclusion in this study may have resulted in a degree of selection bias. Errors may have occurred in the collation of the list of patients from the hospital database and similarly by the doctors completing the coding form in the ED. Similarly, as the data were being collected for each of the patients from their ED medical notes, reliance was placed on the information being both accurately and legibly documented. This may have led to some error in data collection and should be considered when interpreting the study results. The most appropriate method of overcoming a number of the study limitations is to complete a prospective study.
Another study limitation involves the use of the WIMD 2011 codes and the income domain indicator as the measure of social deprivation. This is a measure of area rather than individual deprivation and it is important to consider therefore that not everyone living in a deprived area is deprived, and that not all deprived people live in deprived areas. It should also be highlighted subsequent analysis of components of a composite outcome measure could lead to erroneous conclusions due to multiple testing. This should be taken into account when considering the results of this study.
Conclusions
This study has highlighted a number of well-recognised risk factors for the development of complications following blunt chest wall trauma. These included patient age, number of rib fractures and chronic lung disease. This is the first study in which social deprivation has been investigated as a risk factor for complications following isolated blunt chest wall trauma. The results of the study indicated that social deprivation was not a risk factor for the development of complications following isolated blunt chest wall trauma. Social deprivation was found to be a risk factor for prolonged length of stay. Patients from a more deprived area are more likely to be the victim of assault resulting in isolated blunt chest wall trauma and are also more likely to have an unplanned representation to the ED. Further research is needed to investigate the potential underlying causes for the results found in this study, such as increased alcohol intake, homelessness or unemployment. A prospective multi-centre study is planned to further investigate the impact of social deprivation on outcomes in blunt chest wall trauma patients.
Footnotes
Acknowledgements
This work was completed at the Emergency Department, Morriston Hospital, ABMU Health Board, Swansea, UK. Dr Ceri Battle has access to all the original data and takes responsibility for the integrity of the data. There are no conflicts of interest or financial support to declare.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.