
Abstract
Objective
To explore the prevalence of type I and type II Helicobacter pylori infection and investigate risk factors in a population from Hainan Province in China.
Methods
Data came from a large, cross-sectional study conducted from August 2022 to April 2023 involving five cities of Hainan. Subjects with confirmed 14C-urea breath test (UBT) and positive serological assay were included. All subjects had a gastroscopy. According to presence or absence of CagA/VacA proteins, subjects were classified as either type I (present) or type II strains (absent). Gastroscopic findings and several socio-demographic factors were examined for correlation with antibody serotyping.
Results
In total, 410 subjects were investigated for H. pylori strain types. The overall prevalence of the highly virulent, type I H. pylori strain was 79% (324/410) and type II strain was 21% (86/410). There was a strong association between type I strain and peptic ulcer disease. Of several sociodemographic factors investigated, only smoking and data over baseline (DOB) values showed significant differences between type 1 and type II strains. Logistic regression analysis showed a lower risk of type I H. pylori infection in smokers compared with non-smokers, and a higher risk of H. pylori type I infection in subjects with medium and high data over baseline (DOB) values compared with subjects who had low DOB values.
Conclusion
Highly virulent, type I H. pylori infections predominate in Hainan and the co-positivity of CagA and VacA antibodies are related to type I H. pylori infection. We found that Type I H. pylori was closely associated with peptic ulcer disease and the DOB values were generally high.
Keywords
Introduction
Helicobacter pylori (H. pylori) is a gram-negative bacterium that colonizes primarily in the stomach and duodenum and affects approximately half of the world’s population. 1 Interestingly, results from a meta-analysis indicated that the overall prevalence of H. pylori infection in China is about 44%. 2 Research has shown that H. pylori has developed complex multiple adaptive mechanisms to evade the immune system while promoting chronic inflammation in the stomach and duodenum, and, most infected people do not show any significant symptoms. 3 However, H. pylori has been shown to be a major risk factor for chronic gastritis and peptic ulcer disease, and, it is also the primary carcinogen for gastric cancer.4,5 The pathogenicity of H. pylori is mediated by an interplay of several virulence factors that include cytotoxin-associated gene A (CagA), and vacuolating cytotoxin A (VacA) which play a critical role in disease development. 4 Indeed, H. pylori infection has been subdivided into type I and type II strains based on the presence or absence of CagA/VacA proteins, respectively. 5 Importantly, studies have shown that type I H. pylori is closely associated with the development of upper gastrointestinal (GI) disease and gastric cancer. 5
It is generally accepted that the peak period of H. pylori infection is during childhood and that intrafamilial transmission is the main route of infection. 6 The number of siblings, mother’s infection, age, low socioeconomic status, residing in a rural environment, and family crowding have been considered as high-risk factors for H. pylori infection. 7 However, there is a paucity of data on potential risk factors affecting H. pylori strain types. Therefore, the aim of this study was to investigate the distribution of H. pylori types I and II among subjects in Hainan Province in China and investigate correlations between strain types and upper GI diseases.
Methods
Study population
This study was conducted from August 2022 to April 2023 using data from 21 health service stations and a tertiary hospital, and subjects were from five cities respectively in north, south, east, west, and central area in Hainan (i.e., Haikou, Sanya, Qionghai, Dongfang, and Wuzhishan). Suitable subjects had either, been involved in a previous study and were willing to undergo further examinations, 8 or were recruited from outpatient services. To be eligible for the study, subjects had to be permanent residents of Hainan Province, over 14 years of age, able to complete a 14C-urea breath test (UBT) and a questionnaire, and provide written informed consent. The following subjects were excluded: in the past two weeks had received proton pump inhibitors, bismuth and H2 receptor blockers or other drugs that could have affected a breath test result; in the past four weeks had received antibiotics; had severe heart, liver, and kidney dysfunction; had active upper GI bleeding; had undergone previous partial or total gastrectomy; were suffering with serious mental illness; were unable to complete the study questionnaire correctly. Subjects were interviewed face-to-face by trained personnel using a standardized epidemiological questionnaire and information related to various sociodemographic factors, lifestyle, environmental exposures, clinical manifestations, and personal medical history were collected. The study protocol was approved by the Ethics Committee of Second Affiliated Hospital of Hainan Medical University (2023-KCSN-17; November 29, 2023) and written informed consent was obtained from all participating subjects. The reporting of this study conforms to STROBE guidelines. 9
Assessment of H pylori infection strain type
The status of H. pylori infection strain type was confirmed by a 14C-urea breath test (UBT) and a serological H. pylori antibody test.
Urea breath test
Full details of the test have been reported elsewhere. 8 In brief, eligible subjects were tested on an empty stomach or had fasted for at least 2 hours before taking the test. Subjects swallowed a 14C urea capsule with an appropriate amount of water and then waited for 15–20 min. Subsequently, they were asked to blow their breath on a card for about 3–5 min, and sampling was completed when the colour of the indicator tablet had changed from orange to yellow indicating the presence of H. pylori. Basal delta over baseline (DOB) values were categorised as low (≥4 DOB <16) or medium/high (DOB ≥16). 10
Serology
The immunoblotting method was used to detect IgG antibody in serum samples. H. pylori antibody typing test kit (manufacturer: Shenzhen Burroughs Bio-products Co., Ltd; medical device registration No.: National Instruments Note Approval 20153401438) was used according to manufacturer’s instructions for detection of the bacterium. For this test, 2–5 ml of fasting venous blood was collected from each subject. All samples were analysed within 2 h of blood collection. The H. pylori antigen was electrophoresed by SDS-polyacrylamide gel, separated according to different molecular weights, and then transferred to nitrocellulose membrane. If there was corresponding antibody in the examined serum, enzyme-linked immunosorbent assay (ELISA) was applied, and colour bands appeared in the corresponding position of the antigen, and the H. pylori type was judged according to the molecular weights of the positive bands.
H. pylori strain types were determined from blood samples as follows: (1) type I H. pylori antibody positive (i.e., presence of CagA and VacA bands either alone or together); (2) type II H. pylori antibody positive (i.e., only one of urease (Ure) A and UreB bands or both, but no CagA, VacA bands present); (3) H. pylori antibody negative (i.e., only control band appeared in colour-developing zone, and no positive zone is observed). Gastroscopy was performed on all subjects who had a positive UBT and serological H. pylori antibody test.
Statistical analysis
This study focused on the H. pylori serotyping as the main study index. In a previous study, the overall type I strain prevalence in Chinese subjects was estimated to be approximately 58%. 11 Therefore, using α = 0.05 (two-sided test), with an allowable error δ = ±1.7%, Z_(1-α/2) = 1.96, and P = 58%, the calculation yielded a requirement for 370 subjects. However, considering a shedding rate of 10%–20%, a total of 410 cases were needed in the study, which ensured both the accuracy and scientific validity of the study results.
Statistical analysis was performed using SPSS software (version 25.0 for Windows®; IBM Corp, Armonk, NY, USA). A P-value <0.5 was considered to indicate statistical significance. Continuous variables were presented as mean ± SD, and categorical variables were described as percentages or frequencies and χ2 tests were used to compare inter-group differences. Univariate and multifactorial logistic regression analyses were used to investigate significant predictor variables for type I infection and estimate odds ratios (ORs) with 95% confidence intervals (CIs).
Results
H pylori infection strain status
In total, 410 subjects were investigated for H. pylori strain types. Of these, 238 (58%) subjects were male and 172 (42%) were female with a mean age of 54 ± 17 years (range 18–93 years). The overall detection rates of H. pylori CagA, VacA, UreA and UreB antibodies were 77% (316/410), 58% (238/410), 58% (238/410) and 83% (342/410), respectively. Differences in the detection rates between the regions for each type of antibody were not statistically significant (Table 1).
Distribution of H. pylori antibodies through the districts of Hainan.

Data are expressed as, n (%).
Cag A, cytotoxin-associated gene A; VacA, vacuolating cytotoxin A; UreA, urease A; UreB, urease B; ns, not statistically significant.
Overall prevalence of the highly virulent, type I H. pylori strain was 79% (324/410) and type II was 21% (86/410). Although the detection rate of type I H. pylori strain was higher than that of type II H. pylori in all regions of the province, the difference was not statistically significant (Table 2).
Distribution of H. pylori antibody typing in Hainan.

Infections that could not be determined by antibodies were categorized as type II strains.
Data are expressed as, n (%).
Cag A, cytotoxin-associated gene A; VacA, vacuolating cytotoxin A; UreA, urease A; UreB, urease B; ns, not statistically significant.
Correlation between H. pylori strain type and upper gastrointestinal diseases
Based on gastroscopic results and histopathologic types, subjects were categorized into four groups: peptic ulcer disease; non-atrophic gastritis; chronic atrophic gastritis/ intestinal metaplasia; gastric cancer. Compared with type II strain, type I strain was more strongly associated with peptic ulcer disease (P < 0.001). However, incidences of non-atrophic gastritis, chronic atrophic gastritis/intestinal metaplasia, and gastric cancer did not correlate with H. pylori antibody typing (Table 3).
Correlation between H. Pylori strain type and upper gastrointestinal disease.

Data are expressed as, n (%)
CAG, chronic atrophic gastritis; IM, intestinal metaplasia; ns, not statistically significant.
Analysis of influencing factors associated with H. pylori serotyping
Of several sociodemographic factors investigated by univariate analyses, only smoking (P < 0.05) and data over baseline (DOB) values (P = 0.001) showed significant differences between type 1 and type II strains (Table 4). A multifactorial logistic regression analysis was conducted using the significant findings from the univariate analysis to determine if the factors were correlated with type I H. pylori infection. Subjects with medium and high DOB values were shown to have a significantly higher risk of type I H. pylori infection (OR = 2.67;95% CI = 1.525–4.765) than subjects with low values. By contrast, smokers had a reduced risk of type I H. pylori infection compared with non-smokers (OR = 0.57; 95% CI; 0.35, 0.94) (Table 5).
Univariate analysis of various factors that may be associated with H. pylori typing.
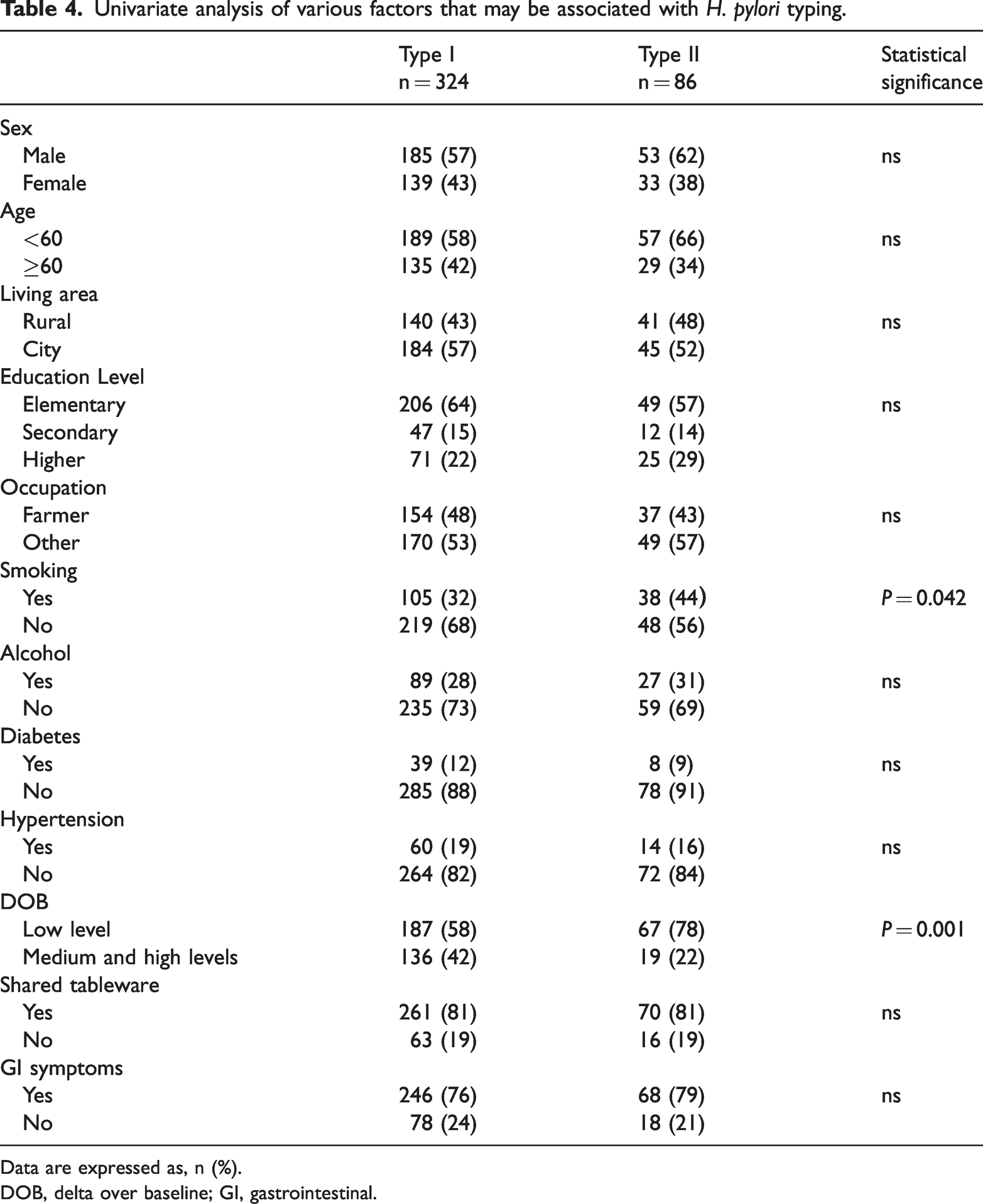
Data are expressed as, n (%).
DOB, delta over baseline; GI, gastrointestinal.
Risk factors for type I H. pylori infection as confirmed by logistic regression analysis.

DOB, delta over baseline.
Distribution of H. pylori antibodies by sex and age group
In male subjects, detection rates of H. pylori CagA, VacA, UreA, and UreB antibodies were 58%, 56%, 58%, and 56%, respectively. Although these values were slightly higher than for females (i.e., 42%, 45%, 42%, and 44%, respectively) differences between sexes in antibody detection rates were not statistically significant (data reported in text and not in a table).
For the ≥60 age group detection rates of H. pylori CagA, VacA, UreA, and UreB antibodies were 42%, 42%, 39%, and 40%, respectively. Although these values were higher compared with the ≤39 years and 40–59 age groups, differences between age groups in antibody detection rates were not statistically significant (data reported in text and not in a table).
Among the type I H. pylori infected group, CagA and VacA were predominantly co-expressed in all three different age groups and there was no statistically significant difference among groups. However, UreB was predominantly expressed alone in different age groups among subjects with type II strain. Again, detection rates of the distinct subtypes in the different age groups were not statistically significant (data reported in text and not in a table).
Discussion
The diverse clinical presentation of H. pylori infection is related to the interaction among bacterial virulence, host genetics, and environmental factors.12,13 Of these, the virulence factors secreted by H. pylori primarily form the molecular basis of disease pathogenesis and determine the pathogenicity of H. pylori. 14 These virulence factors can be categorized according to four major pathogenic processes: colonization; damage to the gastric mucosal epithelium; inflammatory and immune responses; disease induction.15,16 CagA and VacA are considered the main virulence factors of H. pylori. 4 The protein CagA has been shown to induce substantial cellular alterations through the injection of filamentous structures into the gastric epithelial cells as part of a type IV secretion system (T4SS). This process impairs cell motility, proliferation and apoptosis, which can ultimately modulate the arrangement of the entire cytoskeleton. 16 VacA is a multifunctional toxin which can damage the gastric mucosa and delay the repair of gastric epithelial cells through vacuolation, induction of apoptosis and promotion of autophagic pathways.4,16 An additional virulence factor used by H. pylori is urease. In the stomach, urease hydrolyses urea to produce ammonia and carbonic acid. These two substances provide the necessary environment for the settlement and survival of H. pylori by neutralizing gastric acid. 4
Previously, H. pylori bacteria were classified into high virulence type I strains (i.e., expressing CagA/VacA proteins) and low virulence type II strains (i.e., did not express CagA/VacA proteins).5,17,18 Several differences in pathogenicity between H. pylori strains have been reported, with regional differences being an important factor. Studies indicate that several regions worldwide are predominantly infected with the high virulence type I strain.5,19,20 Indeed, our present study also showed that the highly virulent, type I H. pylori strain was predominant in Hainan, with an incidence rate of up to 79%. Our detection rates for CagA, VacA, UreA, and UreB antibodies were consistent with findings from a previous study. 5
It is well established that highly virulent, H. pylori strains are more pathogenic and can potentially cause severe upper GI disease.4,5 Although we found a strong association between the type I strain and peptic ulcer disease, in contrast to previous studies, we did not observe significant differences in the prevalence of chronic non-atrophic gastritis, atrophic gastritis/intestinal metaplasia or gastric cancer among those infected with different H. pylori strains. 21 We suggest that this finding could have arisen because, in addition to the two main virulence factors (i.e., CagA and VacA), other H. pylori pathogenic factors such as, outer inflammatory protein A (OipA), blood group antigen-binding adhesin (BabA) and outer membrane protein (OMP), may also be involved in the development of upper GI disease. 16 Furthermore, H. pylori infection is not the only factor which contributes to the development of upper GI tract disease; several other factors such as smoking, alcohol consumption, sleep deprivation and non-steroidal anti-inflammatory drugs have also been associated with damage to the gastric mucosa.22,23 Moreover, while previous studies in western populations have shown that infection with highly virulent, H. pylori strain (CagA positive) can significantly increase the risk of atrophic gastritis and gastric cancer, studies in Asian populations have not confirmed this relationship.24–26 In addition to serotyping, H. pylori genotypes appear to be also associated with GI disorders. For example, a study from Germany found that the vacA s1 allele was a significant risk factor for duodenal ulcer, vacA s2 for chronic gastritis, and vacA s1 and vacA s2 for gastric ulcer. 27 Similarly, Iranian researchers have suggested that cagA-EPIYA-ABCCC motif has a strong positive relationship with gastric cancer. 28 These findings may also explain our results. Due to sample limitations, we did not investigate cagA and vacA genotypes.
Currently, there is no consensus on potential risk factors associated with H. pylori serotyping. While a Spanish study reported that sex, age, education and body mass index (BMI) were correlated with H. pylori serum antibodies, we did not find any significant correlation between H. pylori serotyping and sex, age, area of residence, education, occupation, alcohol consumption, diabetes, hypertension, sharing of utensils, or GI symptoms. 19 However, univariate analysis showed that there were significant differences between type I and type II strains in terms of DOB values and smoking status. Further investigations using multifactorial logistic regression analysis showed a higher risk of H. pylori type I infection in subjects with medium and high DOB values compared with subjects who had low DOB values. As mentioned previously, CagA and VacA can effectively adapt to the complex gastric environment through multiple mechanisms that facilitate them escaping from host immune clearance and allow them to persist in the stomach. This will ultimately lead to an increased density of H. pylori in the stomach, which may explain the generally high DOB values of type I H. pylori strain in this study. Interestingly, the multifactorial logistic regression analysis also showed a lower risk of type I H. pylori infection in smokers compared with non-smokers.
Our study had several limitations. For example, the small number of subjects and risk factors included in the study may have impacted the analysis of H. pylori serotyping and related influencing factors. In addition, it was a cross sectional study and so did not reflect temporal changes. Furthermore, it was restricted to subjects over 14 years of age and so did not cover all age groups. This is particularly pertinent since the peak period of H. pylori infection is during childhood. 6 Therefore, more prospective large-scale studies across different age groups are required to investigate H. pylori serotyping and related risk factors further.
In summary, highly virulent, type I H. pylori infections predominate in Hainan and the co-positivity of CagA and VacA antibodies are related to type I H. pylori infection. We found that Type I H. pylori was closely associated with peptic ulcer disease and the DOB values were generally high.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241253454 - Supplemental material for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China
Supplemental material, sj-pdf-1-imr-10.1177_03000605241253454 for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China by Runxiang Chen, Daya Zhang, Yanting Lv, Shimei Huang, Da Li, Fan Zeng, Chen Chen, Xiaodong Zhang, Shiju Chen, Jun Wang and Feihu Bai in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241253454 - Supplemental material for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China
Supplemental material, sj-pdf-2-imr-10.1177_03000605241253454 for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China by Runxiang Chen, Daya Zhang, Yanting Lv, Shimei Huang, Da Li, Fan Zeng, Chen Chen, Xiaodong Zhang, Shiju Chen, Jun Wang and Feihu Bai in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605241253454 - Supplemental material for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China
Supplemental material, sj-pdf-3-imr-10.1177_03000605241253454 for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China by Runxiang Chen, Daya Zhang, Yanting Lv, Shimei Huang, Da Li, Fan Zeng, Chen Chen, Xiaodong Zhang, Shiju Chen, Jun Wang and Feihu Bai in Journal of International Medical Research
Supplemental Material
sj-pdf-4-imr-10.1177_03000605241253454 - Supplemental material for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China
Supplemental material, sj-pdf-4-imr-10.1177_03000605241253454 for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China by Runxiang Chen, Daya Zhang, Yanting Lv, Shimei Huang, Da Li, Fan Zeng, Chen Chen, Xiaodong Zhang, Shiju Chen, Jun Wang and Feihu Bai in Journal of International Medical Research
Supplemental Material
sj-pdf-5-imr-10.1177_03000605241253454 - Supplemental material for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China
Supplemental material, sj-pdf-5-imr-10.1177_03000605241253454 for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China by Runxiang Chen, Daya Zhang, Yanting Lv, Shimei Huang, Da Li, Fan Zeng, Chen Chen, Xiaodong Zhang, Shiju Chen, Jun Wang and Feihu Bai in Journal of International Medical Research
Supplemental Material
sj-pdf-6-imr-10.1177_03000605241253454 - Supplemental material for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China
Supplemental material, sj-pdf-6-imr-10.1177_03000605241253454 for Detection of Helicobacter pylori strain types and analysis of risk factors among subjects from Hainan Province, China by Runxiang Chen, Daya Zhang, Yanting Lv, Shimei Huang, Da Li, Fan Zeng, Chen Chen, Xiaodong Zhang, Shiju Chen, Jun Wang and Feihu Bai in Journal of International Medical Research
Footnotes
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This work was supported by Hainan Province Clinical Medical Center (No. 2021818), The specific research fund of The Innovation Platform for Academicians of Hainan Province (YSPTZX202313), Hainan Provincial Health Industry Research Project (22A200078), National Clinical Key Speciality Capacity Building Project (No. 202330) and Hainan Provincial Postgraduate Innovation Research Project (Qhyb2022-133).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.