
Abstract
Objective
We aimed to investigate the relationship between blood pressure and cognitive function among older adults in India.
Methods
In this study, we analyzed cross-sectional data of systolic and diastolic blood pressure (SBP and DBP, respectively) and cognitive testing from 3690 adults aged 60 years and older participating in the Longitudinal Aging Study in India—Diagnostic Assessment of Dementia from 14 states in India.
Results
After controlling for key sociodemographic, health, and geographic factors, higher SBP and lower DBP were each independently associated with worse cognitive function. Older age, female sex, lower education level, being widowed, residing in a rural area, being a member of a Scheduled Caste or Scheduled Tribe, having a low level of economic consumption, being underweight, and a history of stroke were all independently associated with worse cognitive function scores.
Conclusions
Both SBP and DBP were independently associated with cognitive function among older adults in India in diverging directions. Clinical interventions targeting high SBP and low DBP may benefit both cognitive health and cardiovascular health.
Introduction
Evidence for the relationship between cardiovascular health and cognitive function has increased in recent decades, and hypertension has emerged as a key potential modifiable risk factor for dementia prevention,1–3 Most research to date on hypertension and cognitive function has taken place in high-income, Western countries 4 ; few studies have examined this relationship among older adults outside of Europe or the United States. Subsequently, there is still much unknown about the relationship between hypertension and cognition in low- and middle-income countries where older adults may have different physical and social environments, health challenges, and health care systems than their counterparts in high-income countries.
A better understanding of the association between cardiovascular risk factors and cognitive function is especially important in India, which is undergoing substantial demographic changes owing to declining fertility rates and increasing life expectancy5,6 while experiencing an epidemiologic transition as the prevalence of noncommunicable diseases grows. 7 Both transitions result in an increasing population-level risk for dementia owing to an aging population 8 and increasing prevalence of cardiovascular diseases and risk factors. 9
Hypertension treatment and control is an area of particular interest as a potential modifiable risk factor for cognitive decline 1 in India and other low- and middle-income countries. 10 Nearly two-thirds of Indians over age 60 years have hypertension, and nearly 70% of those with hypertension are either undiagnosed or diagnosed but uncontrolled. 11 Given the large burden of hypertension and the growing population of older adults in India, as well as the emerging evidence that blood pressure control may reduce dementia risk, we sought to investigate the relationship of systolic and diastolic blood pressure (SBP and DBP, respectively) with cognitive function using new data from the Longitudinal Aging Study in India—Diagnostic Assessment of Dementia (LASI-DAD). This analysis builds on our prior study of LASI-DAD data examining the relationship between hypertension (defined as self-reported physician diagnosis or elevated SBP or DBP) and cognitive function. 11 By examining SBP and DBP separately and as continuous variables throughout their full distributions, this study can identify potential differences in how SBP and DBP may relate to cognitive function.
Methods
The Longitudinal Aging Study in India—Diagnostic Assessment of Dementia (LASI-DAD)
The LASI-DAD is a National Institute of Aging-funded study that collects data on demographics, health, economics, and cognitive function among a national sample of Indians aged 60 years or older (N = 4096).12,13 In the LASI-DAD, an informant is interviewed regarding the cognitive and daily function of the respondent, and additional information is collected via geriatric assessment, brain imaging, and genetic analyses. 13 Ethics approval for the LASI-DAD was obtained from the Indian Council of Medical Research and all collaborating institutions. 12 Literate respondents provided written consent for participation; illiterate respondents provided thumbprints instead of signatures.
The LASI-DAD is a sub-study of the larger, nationally representative Longitudinal Aging Study in India (LASI), which collects a broader set of data in a larger sample of over 70,000 Indians aged 45 years or older. 14 The LASI-DAD is one of 10 national studies in countries around the world who belong to the Health and Retirement Study international network that is administering the Harmonized Cognitive Assessment Protocol to generate comparable cognitive function data in low-, middle-, and high-income countries so as to enable international comparisons of dementia risk factors, prevalence, and outcomes. 15
The LASI-DAD uses two-stage stratified random sampling and oversampled participants who had a high-risk of cognitive impairment. In the first stage of sampling for the data used in the present study, the full LASI sample was stratified by participants’ state of residence and cognitive impairment risk. Cognitive impairment risk was determined using respondents’ performance in baseline LASI data collection. For the second stage, participants were randomly selected in approximately equal numbers from the high-risk and non-high-risk cognitive impairment strata. State sample sizes in the LASI-DAD were proportional to samples sizes used in the main LASI; additional details on LASI-DAD sampling have been previously published. 12
LASI-DAD interviews took place an average of 7 months after the main LASI interview, from April 2017 through April 2019. There were no significant differences in response rates between respondents at high risk of cognitive impairment (82.8%) and those without this risk (82.9%), according to their cognitive function in the main LASI. The LASI-DAD has partnered with geriatric health centers in 14 states/Union Territories across India to facilitate interviews. Some interviews are conducted in participants’ homes owing to the respondent’s preference and distance to a health center. 12 Our included LASI-DAD participants were from both rural and urban areas in Jammu and Kashmir, Haryana, Delhi, Rajasthan, Uttar Pradesh, Madhya Pradesh, West Bengal, Odisha, Assam, Karnataka, Kerala, Tamil Nadu, Telangana, and Maharashtra. The interviews were conducted in 13 local languages.
Measures
Cognitive function
Cognitive function was measured using a summary cognition score consisting of 18 cognitive tests administered during the LASI-DAD interview (range from 0 to 360, with higher scores indicating better cognitive function). Additional details on the individual cognitive tests can be found in the LASI-DAD protocol. 12
Blood pressure
For each LASI-DAD participant, blood pressure was measured three times while seated. We used the average SBP and DBP for the second and third measurement as the values for measured SBP and DBP.
Covariates
We assessed several sociodemographic characteristics that are relevant to the risk of hypertension, cognitive function, and health care utilization including age, urban/rural residence, caste, educational attainment (less than lower secondary, upper secondary and vocational training, tertiary education), relationship status (married, widowed, separated/divorced, never married), and per capita household consumption (in Indian rupees).
Caste was self-reported by LASI-DAD participants and grouped into the following categories: Scheduled Caste, Scheduled Tribe, Other Backward Class, or “no caste or other caste.” These categories are all official designations used by the Indian government to recognize socioeconomically disadvantaged groups, and they have been used in previous population-based studies in India 16 including the LASI 17 and LASI-DAD. 11 Whereas caste designation can be associated with socioeconomic status, these categories are broad, heterogeneous, and the association with socioeconomic status varies throughout India. 16
Participants’ economic status was measured using annual per capita household consumption; prior studies have indicated that this is a better measure of economic standing in low-income and rural settings than measures of income or wealth.17,18 Household consumption included self-reported expenses over the previous year for food, household utilities, fees, durable goods, education, health care, discretionary spending, transit, and remittances. Total household consumption was converted to per capita consumption after dividing by the total number of household members.
Health characteristics included body mass index (BMI) calculated using measured height and weight, and self-reported physician-diagnosed stroke, diabetes, and heart disorders.
Six geographic regions were defined: Center (Madhya Pradesh), North (Jammu and Kashmir, Haryana, Delhi, Rajasthan, Uttar Pradesh), South (Karnataka, Kerala, Tamil Nadu, Telangana), East (West Bengal, Odisha), West (Maharashtra), and Northeast (Assam).
Data analysis
We calculated descriptive statistics for sociodemographic and health characteristics, stratified by hypertension status. We estimated four linear regression models with different sets of covariates to examine the relationship between blood pressure (SBP and DBP, 10 mmHg change) and summary cognition. Model 1 was the unadjusted relationship between blood pressure and summary cognition score. In Model 2, the following sociodemographic characteristics were added: age group, sex, education, relationship status, residence, caste, and per capita consumption (quartiles in Indian rupees: ≤24,100, 24,101–36,920, 36,921–58,580, 58,581+). In Model 3, we added the following health conditions and risk factors: BMI, stroke, diabetes, and heart disorders. In Model 4, region of residence was added.
We excluded 406 (9.9%) LASI-DAD participants from the analysis owing to missing data for one or more covariates (85 participants were missing BP data and 294 were missing BMI data), which resulted in the final sample for analysis. We used an adjusted Wald test to assess the overall effect of covariates and a residual plot to assess model fit. All analyses were performed using Stata software, release 15.1 (StataCorp LLC, College Station, TX, USA). We used the LASI-DAD post-stratification sampling weight to adjust for non-responses and the complex sampling design. 19 The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 20
Results
Among our LASI-DAD sample of 3690 participants, the mean SBP was 135.9 mmHg (standard deviation [SD] 22.9) mmHg and the mean DBP was 82.0 (SD 12.2) mmHg (Table 1). The results in Table 1 are stratified by hypertension status, with hypertension defined as SBP ≥140 mmHg or DBP ≥90 mmHg. The mean summary cognition score was 125.0 (SD 43.4) out of a maximum score of 360.0. On average, respondents with and without hypertension performed similarly on cognitive testing. Most LASI-DAD participants (59.6%) were between the ages of 60 and 69 years; 29.9% were between 70 and 79 years old and 10.5% were age 80 years or older. Hypertension was more common among those with urban residence (p < 0.05), no caste or other caste (p < 0.05), obesity (p < 0.001), diabetes (p < 0.05), and a history of stroke (p < 0.05).
Characteristics of the LASI-DAD sample, weighted.
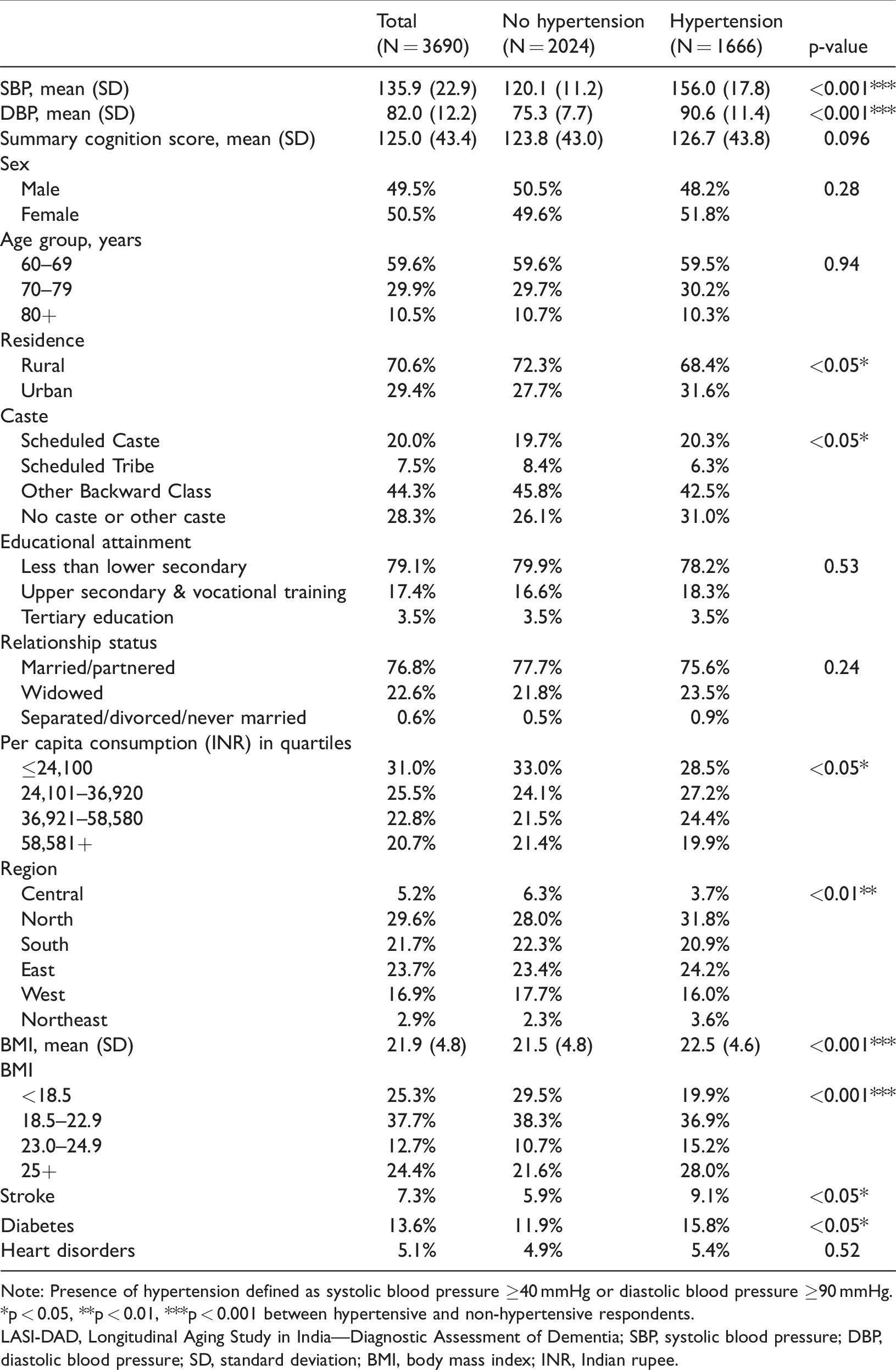
Note: Presence of hypertension defined as systolic blood pressure ≥40 mmHg or diastolic blood pressure ≥90 mmHg.
*p < 0.05, **p < 0.01, ***p < 0.001 between hypertensive and non-hypertensive respondents.
LASI-DAD, Longitudinal Aging Study in India—Diagnostic Assessment of Dementia; SBP, systolic blood pressure; DBP, diastolic blood pressure; SD, standard deviation; BMI, body mass index; INR, Indian rupee.
Table 2 shows results from the linear regression models of summary cognition score for blood pressure and the other covariates. Without adjustment (Model 1), a higher SBP was associated with worse cognition (p < 0.01) whereas a higher DBP was associated with better cognition (p < 0.001). When adding sociodemographic variables (Model 2), older age, female sex, lower education level, being widowed, residing in a rural area, being a member of a Scheduled Caste or Scheduled Tribe, and having a low level of economic consumption were all independently associated with worse cognitive function. The independent relationship of SBP and DBP to summary cognition was attenuated with the addition of these sociodemographic variables. The addition of BMI and self-reported health conditions (Model 3) showed that being underweight (p < 0.001) and a history of stroke (p < 0.01) were associated with worse cognitive function. After additional adjustment for geographic region (Model 4), higher SBP (p < 0.01) and lower DBP (p < 0.001) continued to be independently associated with worse cognition. Figure 1 shows the predicted summary cognition score with SBP and DBP derived from Model 4, holding all covariates constant at their mean values. Several covariates remained independently related to cognition in the final model with older age (p < 0.001), female sex (p < 0.001), lower education level (p < 0.001), being widowed (p < 0.05), rural residence (p < 0.001), being a member of a Scheduled Caste (p < 0.01), being a member of a Scheduled Tribe (p < 0.01), lower economic consumption (p < 0.01 compared with second and third quartiles, p < 0.001 compared with fourth quartile), being underweight (p < 0.001), and a history of stroke (p < 0.01) having a negative association with cognitive test performance. Region of residence was also independently associated with cognitive function, with lower cognitive performance among those in the Central and North regions and higher performance among those in the South region. When dividing the SBP and DBP continuous distributions into quartiles and entering a categorical variable for each quartile into our regression models, we found a monotonic relationship from lowest to highest quartile for both SBP and DBP, with the highest SBP and lowest DBP quartiles each associated with the lowest cognitive function (data not shown).
Multivariable linear regression analysis of blood pressure and covariates on summary cognition score (N = 3,690).
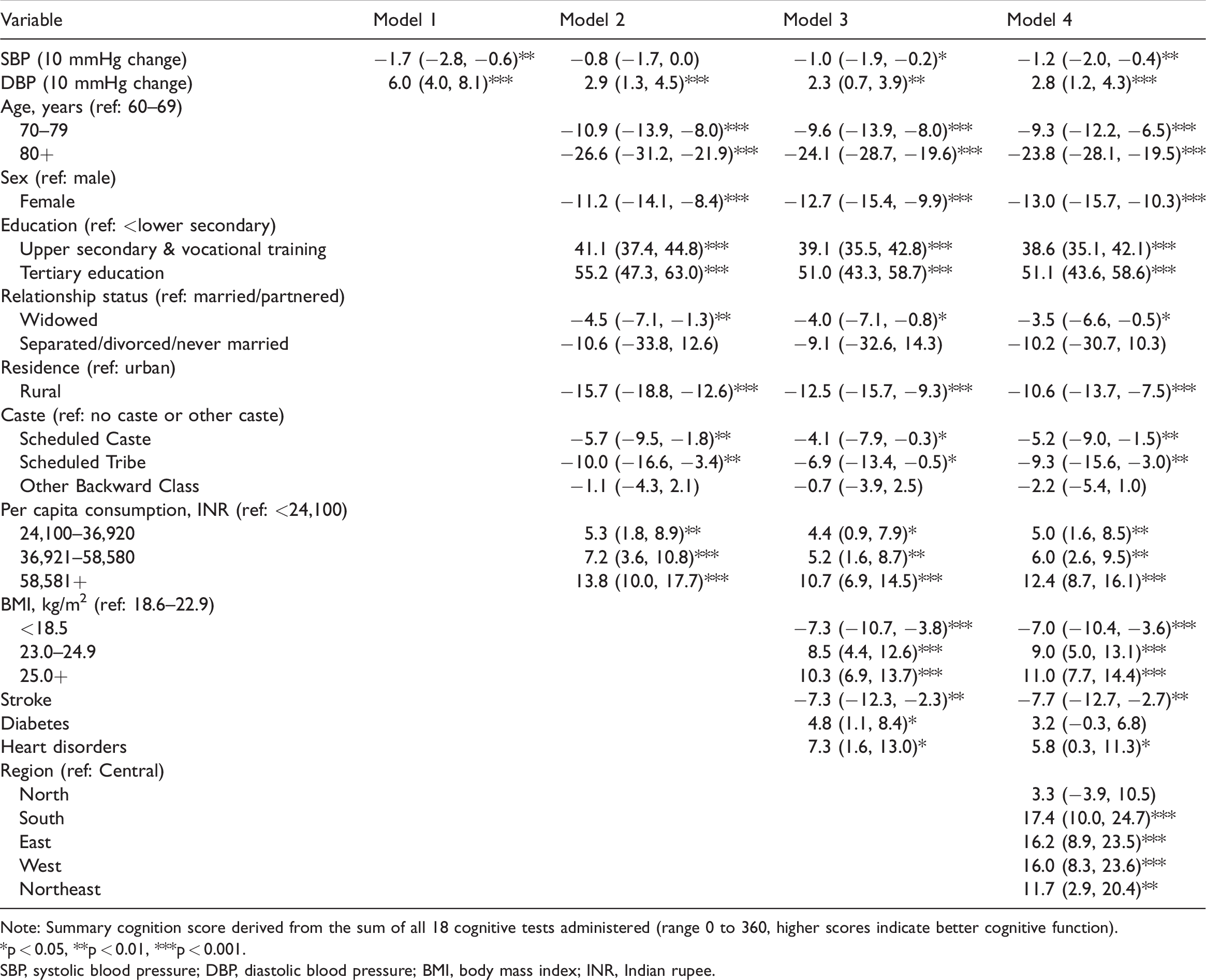
Note: Summary cognition score derived from the sum of all 18 cognitive tests administered (range 0 to 360, higher scores indicate better cognitive function).
*p < 0.05, **p < 0.01, ***p < 0.001.
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; INR, Indian rupee.
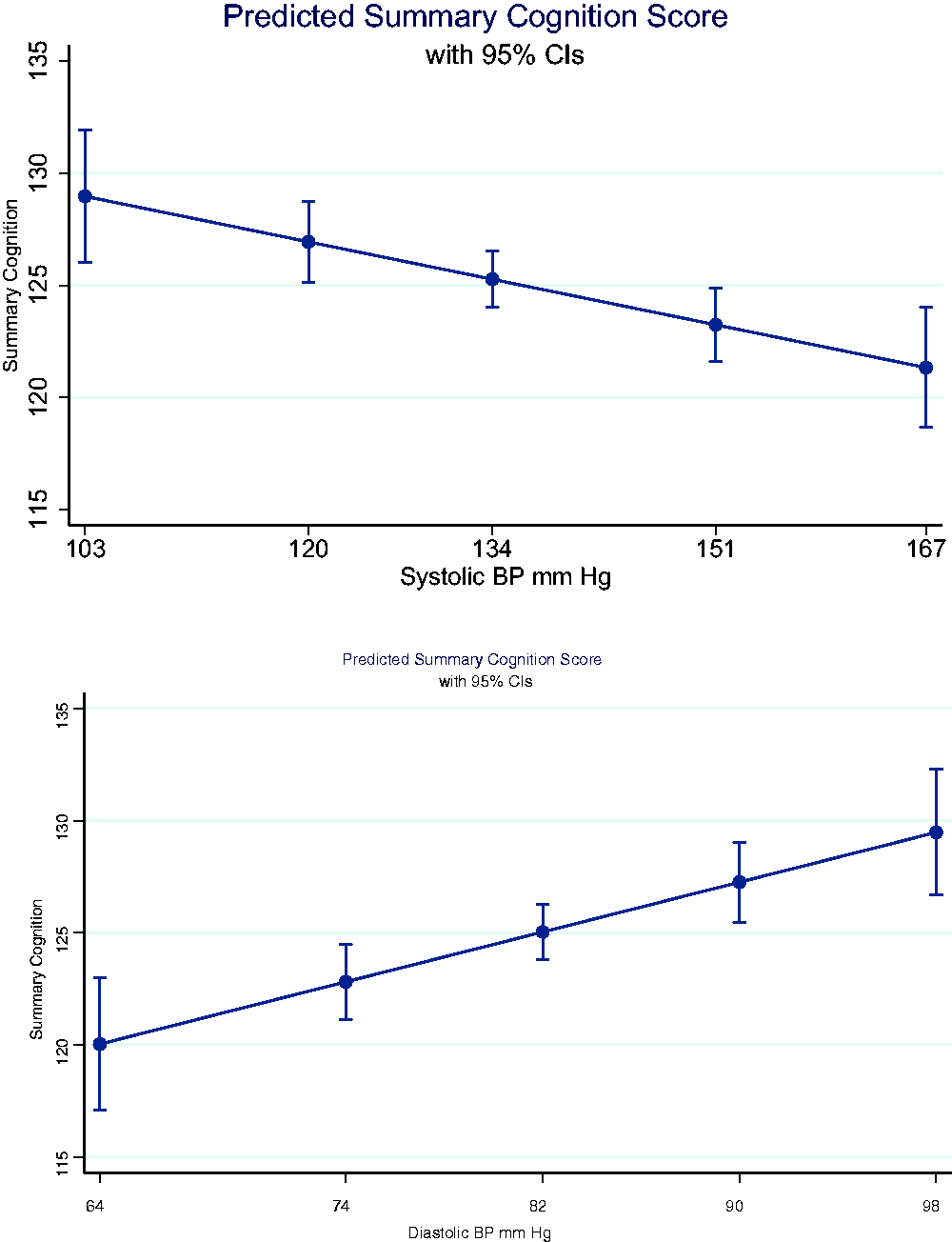
Summary cognition score versus systolic blood pressure (SBP, upper panel) and summary cognition score versus diastolic blood pressure (DBP, lower panel).
In supplemental analyses, we tested whether taking medication for hypertension (as self-reported by LASI-DAD respondents) was independently associated with cognition by adding this variable to Model 4; however, the relationship was not statistically significant (data not shown). Additionally, we tested for interactions among the covariates included in Model 4 and found some evidence that low DBP was more strongly associated with worse cognition in the oldest age group (age 80+ years) than in younger age groups (p = 0.002; data not shown). The interaction between SBP and age was not statistically significant.
Discussion
Using new data from a large, nationally representative survey in India, we found that both SBP and DBP were independently associated with cognitive function among older Indian adults, with higher SBP and lower DBP associated with worse cognition. These findings are consistent with prior cross-sectional 21 and longitudinal studies 22 among older adults in the United States. A 2003 study of adults from a single district in the state of Haryana in northern India found a relationship similar to our findings for DBP and cognition, but an opposite relationship for SBP (higher SBP was associated with better cognitive function in the prior study). 23 In a 2013 study of older adults in Latin America, India, and China, lower SBP was associated with an increased risk of dementia and lower DBP was associated with a higher score on the Clinical Dementia Rating scale in rural India. 24
There are a number of mechanisms that may explain the relationships found in our study between blood pressure and cognitive function. Hypertension may worsen neurodegeneration and cognitive decline owing to increased levels of inflammation, cerebrovascular dysfunction, and both clinical (e.g., stroke) and subclinical (e.g. diminished whiter matter integrity) brain injury.22,25–27 Cerebral hypoperfusion owing to low blood pressure may also adversely affect cognitive function.22,28 Our findings underscore that clinical interventions targeting high SBP and low DBP may benefit cognitive health in addition to cardiovascular health,1–3 particularly in India where the burden of cardiovascular disease and dementia are expected to grow as a result of ongoing epidemiologic and demographic transitions.7,8,10 The SPRINT Memory and Cognition In Decreased Hypertension (SPRINT MIND) trial found that intensive SBP control in older adults (50 years and older, mean age = 68 years) was associated with a lower likelihood of incident mild cognitive impairment or dementia. 1 SBP may be a particularly promising area of focus for hypertension control interventions that could benefit older adults in India. However, as noted in a recent study 28 that included both SPRINT and Action to Control Cardiovascular Risk in Diabetes–Blood Pressure (ACCORD-BP) trial data, aggressive treatment of hypertension that results in low levels of DBP (<60 mmHg) may increase the risk for adverse cardiovascular outcomes; similarly, our findings raise the question of whether treatments that result in low DBP may also increase the risk for worse cognitive outcomes.
Interestingly, our previous findings exploring the relationship between hypertension, defined as a clinical diagnosis or hypertensive blood pressure measurement (≥140/90 mmHg), did not show an independent relationship between hypertension and cognitive test performance; however, we found significant relationships between various sociodemographic factors and cognitive performance. 11 When examining the relationships with SBP and DBP as continuous variables, we found significant relationships with cognitive function. These differences in findings highlight the importance of how blood pressure measurement and hypertension variables are operationalized and analyzed in population-based studies. Moreover, our previous analyses found that most participants with hypertension in the LASI-DAD sample were undiagnosed or uncontrolled. Health care access may vary according to sociodemographic factors in India, and sociodemographic factors were independently associated with cognitive performance in this analysis and in our prior study. 11 Future longitudinal studies that use the full range of SBP and DBP measurements as well as information regarding hypertension treatment and control will be useful in determining the level of blood pressure control that is most beneficial to brain health.
Several sociodemographic and health covariates showed a significant cross-sectional relationship with cognitive test performance in our final model. Other studies in high and low- and middle-income countries have also found that older age,29,30 female sex, 30 lower educational attainment,10,29,30 lower socioeconomic status,29,30 being underweight, 29 and a history of stroke 29 are associated with worse cognitive function. Additional factors associated with worse cognitive test performance in the LASI-DAD were being widowed, being a member of a Scheduled Caste or Scheduled Tribe, and residing in a rural area. These findings highlight the importance of social and economic factors as contributors to the cognitive health of older Indian adults. Additionally, we found significant regional differences in cognitive test scores, with individuals residing in Central and North regions performing worse than those in the South, East, West, and Northeast regions. Prior studies have documented large health differences among geographic regions of India.7,31 Further research is needed to better understand the mechanisms by which these geographic differences arise. Addressing potential geographic differences in access to hypertension care and treatments may be one strategy to reduce undiagnosed and inadequately treated hypertension in India, especially as demands on the health care system are expected to grow as older adults make up a greater share of the population. 32
There are several potential limitations to our study. Because there is currently only one wave of LASI-DAD data available, our analyses were cross-sectional; therefore, we are unable to establish the direction of causality for the relationships investigated. We were also unable to ascertain blood pressure variability or the timing of onset and duration of elevated or low blood pressure. Finally, our cognitive outcome measure was an overall summary score, so potential relationships for individual cognitive domains could not be assessed.
There are also several strengths in our study including the use of recently collected, high-quality data from the LASI-DAD, a national study with comprehensive social, economic, and health survey data, biomarker data, and cognitive testing. The study design allows for future analyses using LASI-DAD data that can be augmented with additional variables from the main LASI study because all LASI-DAD participants are also in the LASI sample. We were able to analyze a variety of social, economic, and health factors alongside direct blood pressure measurement data and robust cognitive testing data.
In conclusion, we found evidence of an independent cross-sectional association between high SBP and low DBP with worse cognitive function. Several sociodemographic characteristics and health characteristics also had significant associations with cognitive function. Future waves of the LASI and LASI-DAD will provide valuable opportunities to use nationally representative longitudinal data to provide additional insights into the relationship among hypertension, hypertension treatment, and cognitive aging in the growing population of older adults in India.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211068720 - Supplemental material for Blood pressure and cognitive function among older adults in India
Supplemental material, sj-pdf-1-imr-10.1177_03000605211068720 for Blood pressure and cognitive function among older adults in India by Madeline R. Farron, Mohammed U. Kabeto, Deborah A. Levine, Caroline R. Wixom and Kenneth M. Langa in Journal of International Medical Research
Footnotes
Authors’ contributions
Study concept and design: MRF, MUK, DAL, KML
Analysis and interpretation of the data: MRF, MUK, DAL, KML
Drafting of the manuscript: MRF, KML
Critical revision of the manuscript: All authors
Statistical analysis: MRF, MUK, KML
Obtained funding: KML
Administrative, technical, or material support: CRW
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by grants from the National Institute on Aging, National Institutes of Health (nos. R01 AG051125 and RF1 AG055273). Dr. Levine was supported by NIH grants (nos. R01 NS102715 and RF1 AG068410). Representatives of the National Institute on Aging were not directly involved in the collection, management, analysis, or interpretation of the data or the decision to submit the manuscript for publication. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Aging or the Department of Veteran Affairs.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.