
Abstract
Despite increasing participation of female athletes in strength-sports such as weightlifting and powerlifting, there is limited research investigating how the menstrual cycle (MC) and MC-related symptoms may influence the strategies and training practices elite athletes and coaches employ to optimise training, wellbeing and competition outcomes. The aim for this study was to investigate both athlete and coach perspectives and lived experiences, to provide real-world application pertaining to athlete health, training, and competition performance throughout the MC. Four semi-structured focus group interviews were conducted, including eight elite female weightlifters and powerlifters, and seven coaches (n = 4 M, 3F). Thematic analysis was conducted using an interpretive phenomenological approach to identify key themes. Athletes shared various experiences of MC-related symptoms including low-back pain, increased fatigue, and changes in technique. Athletes and coaches provided insight into how they adjusted training in response to MC-related symptoms including reducing intensity and swapping exercises or training days. Participants also acknowledged the importance of addressing other factors such as the prevailing stigma of the MC, communication barriers, and knowledge gaps, as these contribute to appropriately managing MC-symptoms around training and competition. This data contributes to our understanding of MC-symptomology, and management of training throughout the MC in strength-sport athletes. Importantly, this research highlights the need to normalise the MC further while advancing knowledge and awareness in the strength-sport environment. Future research integrating MC-symptom tracking and subjective measures alongside objective performance may further clarify the impacts of the MC on elite strength-sport athletes.
Introduction
Competitive strength-sports, such as powerlifting and weightlifting, are individual sports that use resistance exercise training as the primary modality for skill acquisition, conditioning, and performance. Athletes work collaboratively with their coach to develop characteristics of absolute strength and power, and accrue skeletal muscle mass, in order to improve their one-repetition-maximum (1RM) for competition lifts. Powerlifting and weightlifting represent distinct expressions of maximal strength. In powerlifting, success is determined by an athlete's ability to lift the greatest possible loads in three competition exercises (squat, bench press, and deadlift), which are typically performed at low movement velocities due to the high external loads. 1 In contrast, weightlifting places a substantially greater requirement on high movement velocities, as athletes must lift the heaviest possible loads while achieving rapid and precise barbell displacement during two competition lifts: the snatch and the clean and jerk. 2 The individualised nature of strength-sport competition and coach-athlete dynamic means coaches have a large impact on athletes’ performance and success, 3 by tailoring training programs, providing specific technical instruction, and physical, psychological and social development. 4 Such support provision requires an evidence-based approach; integrating coaching expertise, athlete values, and the best relevant research evidence to optimise the decision-making process surrounding performance. 5 However, currently, evidence around coaching practices for strength-sport coaches working exclusively with female athletes is limited, and female athletes are underrepresented in sport and exercise science research 6 across all sports, 7 including strength-sports. Research including and exclusively investigating female strength-sport athletes is particularly important as there has been a substantial increase in female participation rates in weightlifting and powerlifting competition (between 2009–2022).8,9 The applicability of findings from male-participant derived research may be limited in some areas which likely differ in female strength-sport athletes, such as lived experiences, 10 social identity in sport, 3 or the manipulation of/responses to training.11,12 Also, there are physiological differences between males and females related to muscle fibre type, size and distribution, and endogenous sex hormones.13,14 In particular, one key physiological factor that may influence female strength-sport athletes is the menstrual cycle (MC).
The MC is a cyclical pattern of fluctuating endogenous female sex hormones (estrogen and progesterone), which is highly individual and often associated with different symptoms that may affect training practices, athlete health and wellbeing, and performance-related parameters relevant to programming and coaching instruction. Inter- and intra-variability is seen in MC length, phase durations, bleeding patterns and symptoms, 15 choice to use hormonal contraceptives (HC; 48% of female powerlifters, 16 28–57% of the athletic population), 17 and perceived changes in subjective athletic performance. 17 Despite the widespread use of HCs, there is currently limited evidence-based rationale to support or discourage their use in females participating in resistance training aimed at increasing hypertrophy, power, and/or maximal strength. 18 The MC literature has largely focused on females participating in both resistance and cardiovascular exercise types (team-sport or mixed samples of athletes) or have pooled untrained, recreational, and elite athletes in their analysis,19–23 creating limitations in the applicability for elite strength-sport athletes, as training demands and competition performance significantly differ between groups. As there may be links between the presence of MC symptoms and changes in wellbeing and performance,24–26 coaches and athletes may benefit from MC research specific to the strength-sports to inform decisions around support provision and development of individualised plans to optimise health, training outcomes and competition performance.
Athletes from strength-sports commonly acknowledge the prevalence and severity of MC-related symptoms and their potential impacts on training and performance. Commonly reported MC-related symptoms include pain and cramping, reductions in motivation and perceived strength, increased fatigue, and changes in technical execution of lifts, most commonly in the premenstrual or menstrual phase.16,20,27 Despite this recognition, little is known about how training programming is modified throughout the MC. Recently, there has been increasing interest in adjusting training programs around the MC,28–30 and reports from team-sport coaches indicate both a willingness to adapt training sessions31,32 and strong desire to better understand how to optimise training prescription, monitoring practices, and the MC's influence on physical performance. 33 However, research also shows that coaching decisions and support provision in this area are shaped by numerous sociocultural factors including personal experience or lack thereof, coach gender, social stigmas, communication barriers, perceived secrecy, and limited knowledge or research availability.20,21,23,31,34,35 Notably, most of these insights come from studies focused on team sports, with limited data available regarding female strength-sports athletes. To date, only three research groups have specifically examined female strength-sport athletes perceptions of performance, using surveys16,27 or individual semi-structured interviews. 20 To our knowledge, no studies have investigated coaches’ perceptions regarding the MC of their strength-sport athletes or the decision-making processes they employ based on MC phases or associated symptoms. Therefore, this study aimed to investigate the perceptions and practices of both elite strength-sport (powerlifting and weightlifting) athletes and coaches using focus group interviews. Interview questions were designed to provide insight into the influence of the MC, identify practices for managing or adjusting training based on MC-related symptoms, and to explore the individual and sociocultural impacts of the MC on performance, health, and wellbeing of strength-sport athletes.
Methods
Ethics approval was granted by Victoria University Human Research Ethics Committee (HRE23–187). Study design and reporting was completed per the Consolidated criteria for Reporting Qualitative Research (COREQ). 36 The first author (BA) adopted the role of ‘facilitator’ of the group discussion and conducted four separate semi-structured focus group interviews. The focus group interviews were conducted either in-person at Victoria University (Footscray Park Campus, Melbourne), or online via Zoom (Zoom Video Communications Inc., San Jose, CA).
Participant recruitment
Recruitment for coach and athlete focus groups occurred over a five-month period from February to June 2024. Seventeen coaches and thirteen athletes were initially invited to participate. Of these, nine coaches and twelve athletes returned correspondence and were interested in participating. Two coaches were unavailable for focus groups due to overseas travel or coaching commitments, leaving a total of seven coaches who participated. Four athletes were unavailable for focus groups due to work commitments, leaving a total of eight who participated. The first two focus groups were conducted in-person (coaches 1–4; and athletes 1–4); the final two focus groups were conducted online via Zoom (coaches 5–7; and athletes 5–8), and each took between 57 and 71 min to complete.
Methodological orientation
This study was underpinned by a pragmatic research philosophy, and interpretive phenomenological analysis was chosen as the theoretical framework. 37 This framework acknowledges the facilitator plays an active role in the interpretation of data. 37
Interview guide
Prior to data gathering, a semi-structured interview guide (Supplementary File 1A) was developed and informed by relevant literature,31,38–40 agreed upon by the research team, and refined through pilot testing with five female weightlifting and powerlifting athletes. The interview guide included six questions aimed at exploring training practices throughout the MC, and perceptions related to wider sociocultural factors. The semi-structured nature of the guide allowed the facilitator flexibility for prompts and follow-up questions to encourage a flow in discussion and allow the interviewer the flexibility to ask participants to elaborate on specific aspects of their responses.
Reflexivity
The facilitator was a 28-year-old, practicing female strength and conditioning coach and athlete, with a Bachelor in Sport and Exercise Science, and Master in Strength and Conditioning. These qualities allowed for ‘insider status’ that aided recruitment and focus group discussions. Consistent with Braun and Clarke's reflexive thematic analysis, 41 the facilitator is acknowledged as the primary analytic instrument whose interpretative engagement shaped all stages of the research process. The facilitator identifies as a cis-gender woman strength athlete and strength and conditioning coach, is regularly menstruating and tracks her MC, with prior experience using hormonal contraceptives. She entered the study with embodied knowledge of MC–related physical and psychological fluctuations, as well as established coaching practices and beliefs within strength-sport environments. This positionality informed the formulation of research questions, the focus and direction of interview probing, and the analytic attention given to particular patterns of meaning. Shared experiential positioning with participants likely facilitated rapport and depth of disclosure but also risked assumptions of shared understanding. Reflexive practice was therefore embedded throughout analysis, with the facilitator exploring how her experiences influenced coding choices, theme boundaries, and interpretations, and actively working to privilege participants’ accounts over personal expectations. With respect to ethnicity, the facilitator identifies as white, Australian. This may have shaped the analytic lens through which data were interpreted, and therefore the themes and meanings should be understood within this cultural context. Reflexivity was further enacted through regular analytic dialogue with the co-authors, who challenged interpretations and contributed to refining themes. The final themes represent a reflexively co-constructed interpretation rather than an attempt at analytic neutrality.
Participant recruitment and inclusion criteria
Participants were recruited via recruitment flyers on social media and email through purposive, snowball sampling via the facilitator's professional network. To be eligible for the athlete focus group, participants needed to be female, ≥ 18 years old, and have competed at national or international level in their respective strength-sport. For the coach focus group, participants were eligible if they were ≥ 18 years old and had coached a female athlete at national or international level in their respective strength-sport. Prior to the focus group interviews, all participants were informed of the purpose of the project, risks and benefits, and requirements of participation, and consented to participate.
Sample size
We conducted four separate focus groups and aimed to recruit four people per group. This sample size was considered sufficient in relation to the study aim, recruitment specificity, quality of the dialogue, and analysis strategy. 42 Coaches and athletes were separated into different focus group interviews to ensure participant comfort and synergistic group dynamics. Homogeneous grouping reduces the influence of pre-existing power dynamics, 43 and facilitates more open discussion, particularly when exploring potentially sensitive topics such as the MC. This approach also allowed independent exploration of coaches’ and athletes’ perspectives, given expected differences in knowledge and experience. Focus groups were limited to four participants to encourage interaction, equal participation, and in-depth discussion of individual and shared experiences and perspectives.
Data collection and analysis
The focus group interviews were audio-recorded and transcribed verbatim by an independent transcription service (Otter.ai, version 3.70.0; Otter.ai, Inc., Mountain View, CA), imported into Microsoft Word, and then reviewed by the facilitator. Transcripts were de-identified prior to sharing with co-authors (DMH and AN). Data were analysed using a deductive approach, utilising the six phases of thematic analysis. 41 Similar to previous research,38,44,45 to help reduce potential bias and improve study rigour two of the researchers (BA and DMH) independently completed familiarisation, coding, and theme development. Findings were then discussed among three members of the research team (BA, DMH and AN), who reached consensus on key themes and sub-themes. Examples of quotations used to construct codes, sub-themes, and key themes are available in Supplementary File 1B. Participants were provided with the opportunity to withdraw specific statements during or up to 14 days after the focus group discussion, before data analysis and write-up. All participants were given the opportunity to review via email the transcribed data, and in accordance with the COREQ framework (participant checking) a summary of the key results, thematic coding with de-identified quotes, and final themes, to ensure that the information accurately reflected their experiences, views, and opinions and to mitigate any uncertainties. Throughout the discussions, the facilitator ensured relatively equal contribution from all participants. Relative participation was subsequently verified with a retrospective assessment via ChatGPT5 (OpenAI, 2025) (e.g., total word volume and theme attribution frequencies), conducted on aggregated, de-identified metrics only. No identifiable participant data were provided to or processed by any AI large language model. Detailed contribution metrics are provided in Supplementary File 2.
Results
Participant characteristics
Table 1 and Table 2 summarises participant characteristics. The athletes were powerlifters (n = 4) and weightlifters (n = 4), with mean ± SD age of 30.1 ± 4.9 years, and 5.4 ± 2.6 years of training experience within their respective sport. Coaches were from weightlifting (n = 4) and powerlifting (n = 3) backgrounds, with age of 33.8 ± 9.2 years, and 7.8 ± 4.8 years of coaching experience, including 3.6 ± 2.3 years of coaching at a national or international / world level in their respective sport.
Athlete characteristics.
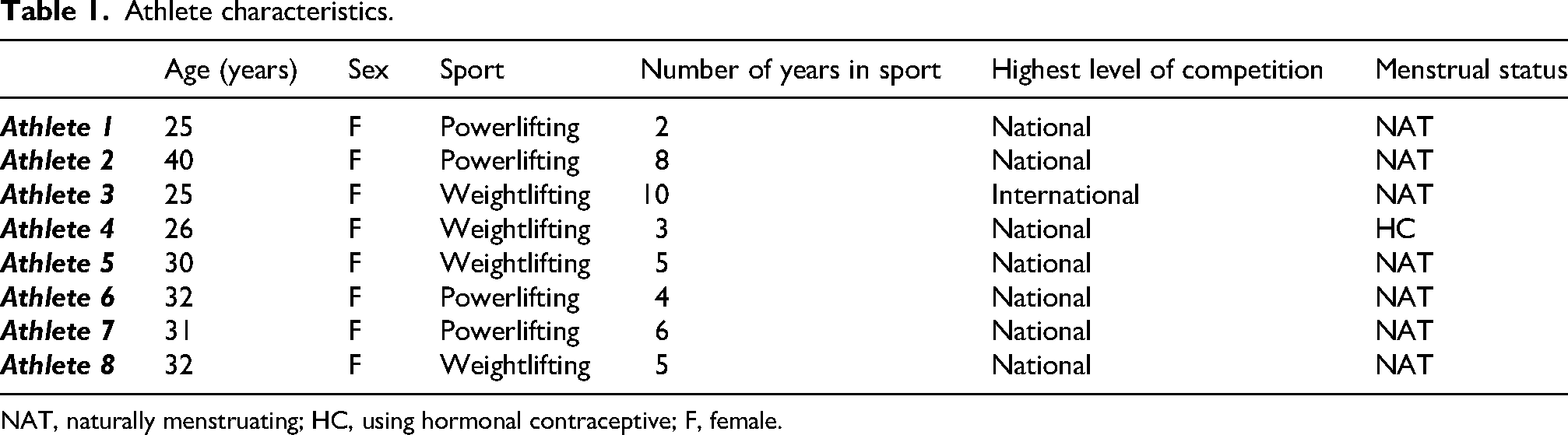
NAT, naturally menstruating; HC, using hormonal contraceptive; F, female.
Coach characteristics.
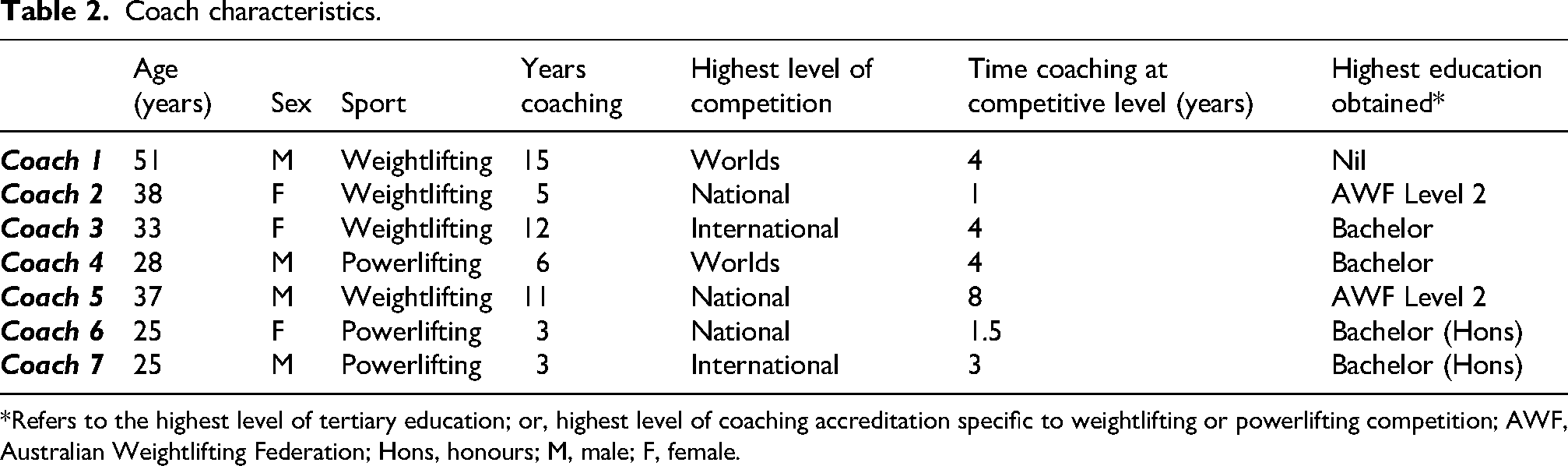
*Refers to the highest level of tertiary education; or, highest level of coaching accreditation specific to weightlifting or powerlifting competition; AWF, Australian Weightlifting Federation; Hons, honours; M, male; F, female.
Final themes
Data analysis revealed five main themes (Figure 1) including (1) MC Symptomology, (2) Training Strategies, (3) Holistic Athlete Health, (4) Culture and Communication, and (5) Knowledge Gaps. The process of coding, sub-theme and theme development, and direct quoting from the focus groups can be found in Supplementary File 1B.
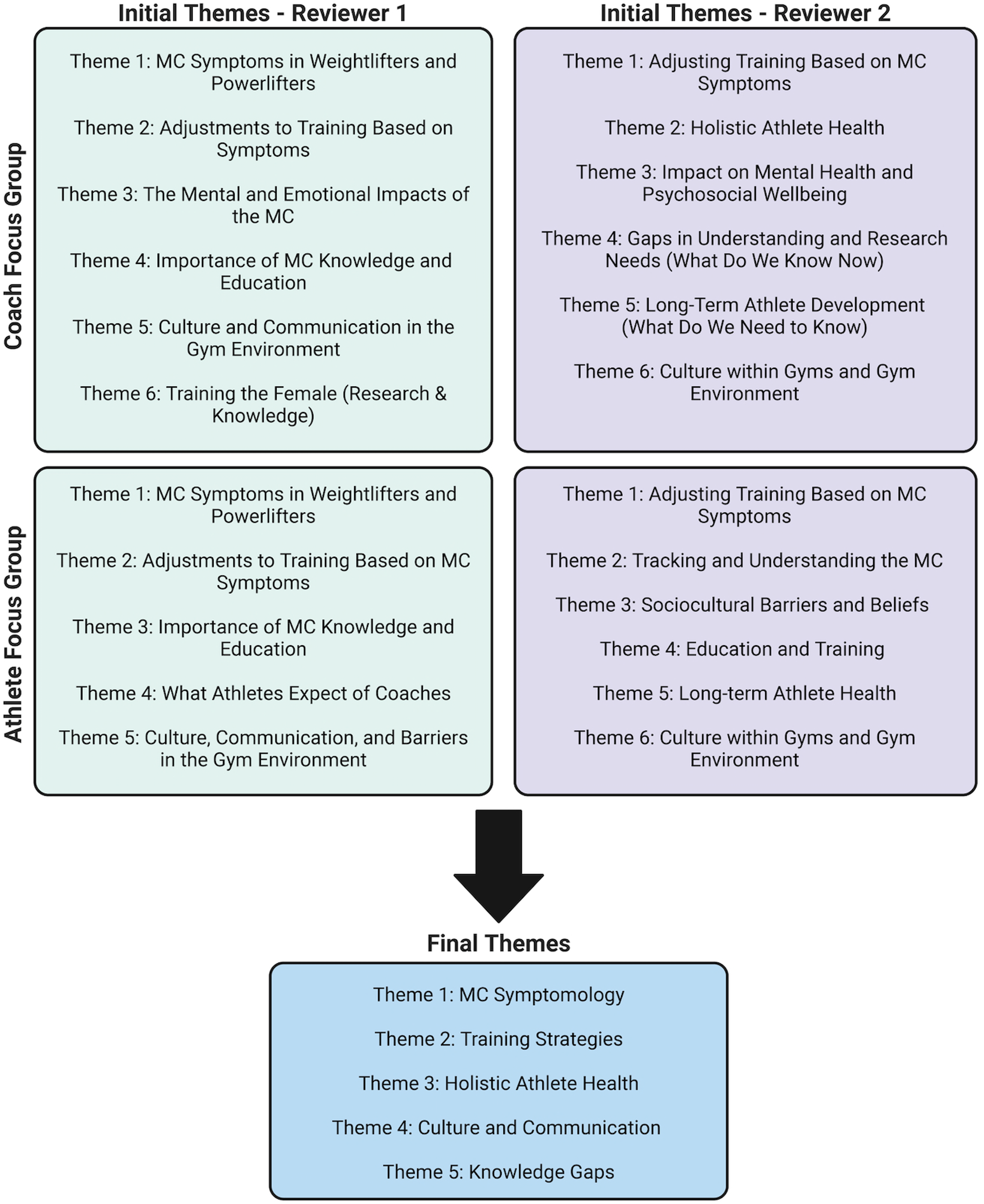
Process of theme development.
Theme 1: MC symptomology
Athletes and coaches briefly discussed common physical and psychological/cognitive symptoms impacting training and performance. All participants recognised that the impacts of MC symptoms were athlete dependant: “We've got a bandwidth of the degrees of which their cycle will affect their training, some barely noticeable, others before anything's on the bar.” Coach 1
Physical symptoms
All athletes in our focus groups experienced physical symptoms, including low-back and joint pain, cramping, heavy bleeding, low energy, increased fatigue, and perceived strength loss and coordination changes in certain exercises. The coaches raised concerns over symptoms, and how they might impact performance through altered technique, changes in timing, bar speed, coordination, and pelvic floor dysfunction. These changes were relatively similar across powerlifting and weightlifting athletes, with slight differences in how they experienced or perceived these MC-related symptoms. For example, weightlifting athletes and coaches mentioned coordination, pelvic stability, and timing changes: “I do get sore boobs or back pain and just noodly, like, just unco (-ordinated)…” Athlete 8 “I'm going to observe that, you know, coordination is down, stability around the pelvis, trunk area is down, they are having symptoms of back pain or maybe like stress urinary incontinence…” Coach 3 “…dips in strength, particularly bench, will get impacted by it (the MC)…” Athlete 6 “If it affected them a lot more and they came in with a lot more bloating or cramping or something like that, and back pain that was really limiting how well they could get into deadlift positions and brace, or use their belt, we would change things.” Coach 7
Psychological/cognitive symptoms
Both athletes and coaches described psychological and cognitive impacts across the MC including changes in behaviour, motivation, emotional state/mood, and increased anxiety and stress. The coaches and athletes acknowledged the influences of external stressors (i.e., outside of training or competition) as important factors influencing MC symptoms and wellbeing: “But what I've noticed with certain stages of the cycle is there can be like, disruption in terms of like mental health things, like anxiety and things of that nature that come along, and then that can end up causing something else and it's a bit of a domino effect.” Coach 2 “…but I have found that stress management has been the best way to manage (PMS symptoms). And depending on how stressed I am, will determine how painful my day one and day two is.” Athlete 3 “But now that I'm on the IUD, it's just very rarely that I would have to pull back because, like I would still get the normal PMS cramps and all that kind of stuff, but it's not as exaggerated… But now, with the contraception, it's around the energy and mood, which in weightlifting, really affects you.” Athlete 4
Theme 2: Training strategies
Both coaches and athletes adjusted training strategies on an individualised basis to overcome performance limitations due to MC-related symptoms, based on conversations and previous trends in symptoms or performance. We identified two sub-themes that reflected the discussion that emerged from our interviews around training strategies: athlete autoregulation and coach-led adjustments.
Athlete autoregulation
The athletes generally expressed that it was important to be intuitive, to listen to their bodies, warming up as normal and adjusting training where needed based on MC symptoms: “But I usually won't know how I'm feeling until I start warming up. So, it's almost something that you, that I have to address on the day.” Athlete 1
Coach-led adjustments
All coaches had clear strategies to alter training, if necessary. Generally, they would first observe the athlete's lifting and training (behaviour), and agreed that if movement quality was altered from normal, a reduction in intensity (load) would be the first adjustment: “Yeah, I drop intensity, first. If quality was dropped, I would match quality with intensity.” Coach 3 “I’m not a huge advocate of avoiding the session entirely, unless that individual is noticeably debilitated in their ability to do anything. I usually find that coming in and actually just moving through the session has more of a positive effect on their actual experience and perception of pain.” Coach 6 “I could alter the training block to three weeks, which might be of benefit to them and just stagger it so that they're working in unison with their cycle… I would, ideally, I would, but it's really dependent upon how much that that athlete knows about themselves.” Coach 1 “It was good having my coaches to help sort of set up my programming and not give me excuses, but give me like, justification of why things might not be going well that particular week.” Athlete 8
The coaches also discussed that training alterations should be carefully made based around performance requirements and/or goals, which are largely dependent on the phase of the year. For example, if near competition time, the coaches expressed views that athletes must learn to negotiate, and train through any MC symptoms to be prepared to perform on competition day. Despite this, the coaches also highlighted that this was only the approach for short periods of time, and that athlete health and wellbeing should be prioritised. Additional to competition phases, coaches expressed that training strategies and alterations based on the MC are athlete dependant, and will vary based on an athlete's own MC trends, temperament, and awareness or knowledge of their MC: “I think it's reactive in the initial phases, and then, depending on where the relationship is at, yeah…Things just appear over time. Patterns tend to appear. For some girls. We just listen to their body.” Coach 5 “So, it's kind of a very conscious awareness of like pulling and pushing depending on the temperament of the athlete and the evidence that you've gathered…” Coach 3
Theme 3: Holistic athlete health
Holistic athlete health was discussed by coaches, which represents viewing the MC as an important factor alongside other variables that contribute to overall wellbeing, such as, sleep, psychology, nutrition, training load, and recovery. The coaches expressed a desire to improve their knowledge around the MC, and in particular its impacts on their athletes. This included being able to monitor any irregularities, address recurring symptoms, or furthering their understanding of bleeding patterns within their athletes. Importantly, the coaches appeared to interpret health similarly to the World Health Organisation definition (“a state of complete physical, mental, and social wellbeing, and not merely the absence of disease or infirmity”
46
; and viewed the MC as being an indicator of health and a pre-requisite for optimal performance: “I think part of being a woman is having a healthy cycle. And if the training that they're doing is impacting their health, because their cycle is impacted, then that's really important information for me to know… if we're looking at having high performing athletes, we also need healthy athletes.” Coach 3 “I've been tracking my cycle for years. I am fascinated by the data, but more so just to make sense of how things feel… not to influence exactly what I do.” Athlete 6 “No, he has no clue what's going on.” Athlete 1 “And then tell that to my coach, and there is a massive difference between me making that decision (to adjust training) and also someone else being like, yeah, you're right, go for it.” Athlete 4
Theme 4: Culture and communication
The presence of MC stigma in society, and within their training and performance environment, was a discussion point for both athlete and coach groups. For athletes, MC stigma was associated with dismissing of symptoms, discomfort in conversations, and was expressed as a major variable in the lack of understanding and dissemination of knowledge of the MC and its potential to impact training and performance: “So, there's never really been a very healthy discourse, at least in the circles that I've been in, around training and periods and where you are in your cycle, that sort of stuff.” Athlete 7 “The coach-athlete relationship is the basis of everything…So that's probably where I go to, is just having an actual relationship with a person. And if you have that relationship, you’re bound to find things about what's affecting their training. Things affect their training. It could be the menstrual cycle…” Coach 5
Theme 5: Knowledge gaps
Coach and athlete participants also mentioned the lack of accessibility of applied and practical information regarding specific elite female strength-sport athlete training: “I don’t think I know and like a lot about the literature out there, I have read a couple of studies. But they have been really impractical studies in my opinion.” Coach 4 “You know in powerlifting, we all squat, bench and deadlift and in weightlifting, you all perform the same movements, regardless of what gender… But the one thing that's very different is our hormones, and the way in which that can be managed, regulated, or not addressed at all. And when we choose to ignore that, we're missing this huge portion of potential performance that might even be going to waste.” Athlete 1 “I think also a coach who actually wants to have knowledge and interest in it, and also is interested in you, as the athlete. Because they also want the trends, for me, that's a coach that actually wants the best for me, and the best performance.” Athlete 4 “I'm not sure exactly his depth of understanding (in reference to her coach). He has enough to know where to stop someone, where to talk to someone, sit with someone…I guess that's a big part of the expectation that I have. Is that they're willing and open, though, to being like, either learning or just listening.” Athlete 5 “More what I would want for them [athletes] is, for them to at least observe how they feel at different points… or at least know roughly when it might be starting… like just kind of baseline stuff like that.” Coach 7 “…our generation and younger generations are sourcing more information, that at least in the fitness industry, there might be a greater tendency to lean towards implementing strategies to address menstrual cycle, performance, dips, etc. At least at a faster rate.” Athlete 2
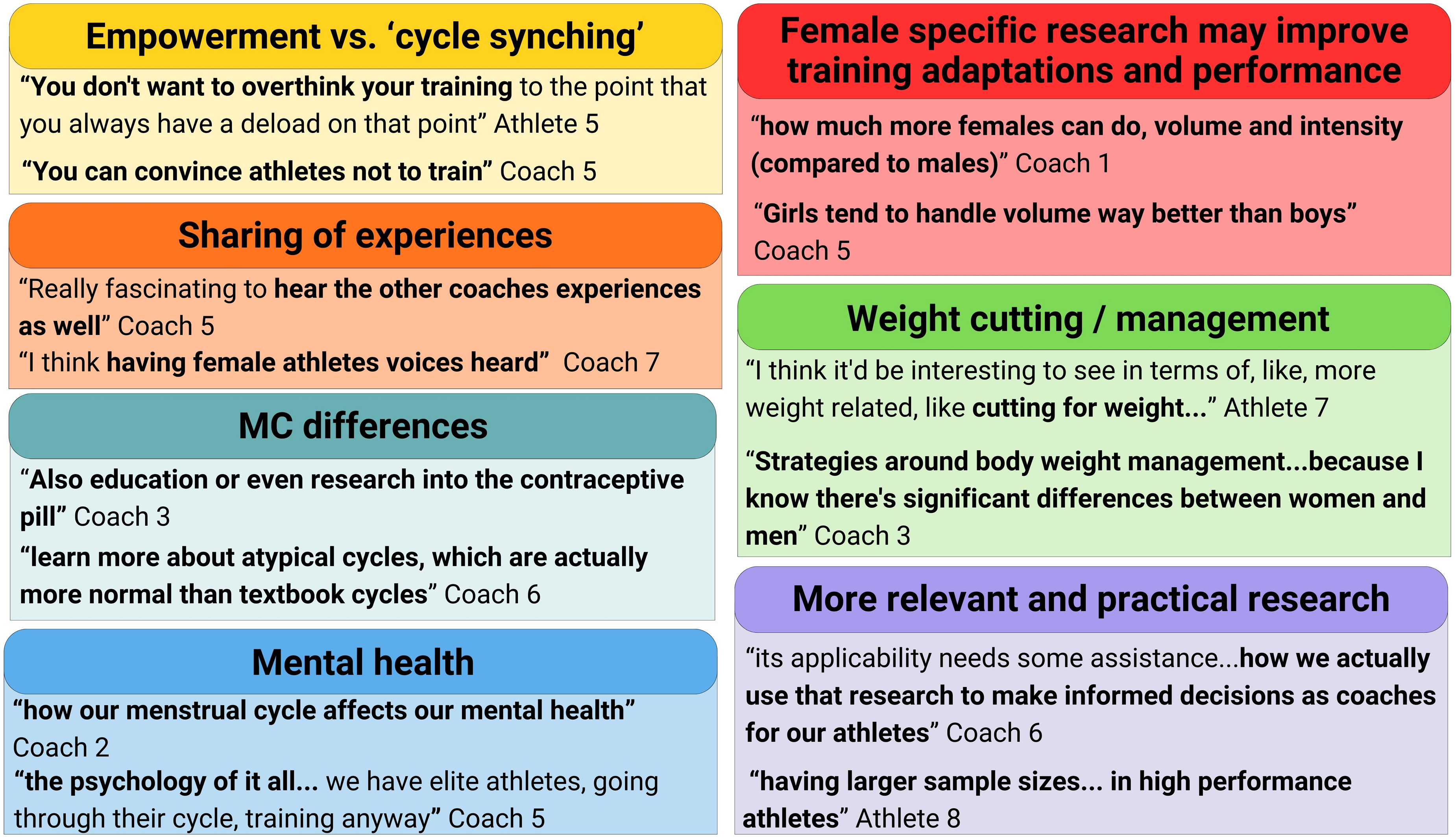
Reflections around future research and education from strength-sport athletes and coaches.
Discussion
The key intention of this study was to engage with elite strength-sport athletes and coaches and provide novel insights into their lived experiences and training practices in relation to the MC. Five key themes emerged from the interviews: (1) MC symptomology, (2) training strategies, (3) holistic athlete health, (4) culture and communication, and (5) knowledge gaps. Both athletes and coaches acknowledged a wide spectrum of physical and psychological symptoms affecting training and performance, with individual variability highlighted as a central consideration when determining appropriate training modifications and managing holistic athlete health. Underpinning these athlete training- and health-related decisions were numerous sociocultural impacts, such as, knowledge gaps, ongoing stigma, and the need for open communication and normalisation of conversations around the MC within training environments. Critically, athletes and coaches identified a lack of pragmatic MC knowledge specific to elite female strength-sport athletes, underscoring the demand for further research and education to inform evidence-based coaching practices and optimise athlete health and performance.
All participants in our research described physical and psychological MC-related symptoms and perceived these to impact training and sport-related performance. Previous reports indicate a high prevalence of MC-related symptoms in strength-sport athletes (83–92% of naturally menstruating, 40–45% hormonal contraceptive users)16,27 and mixed-athlete or team-sport samples (24–100%). 17 Numerous physical (i.e., low-back pain, bloating, cramps, fatigue, decreased coordination, pelvic instability, urinary incontinence) and psychological (i.e., perceived strength loss, altered mood and behaviour, cognitive changes) symptoms were described by participants in our study. These symptoms were perceived to potentially impact performance through altered coordination, as well as changes in timing and bar speed. Akin to this, in previous research, weightlifters (n = 6, 18–28 yr) have described experiencing reduced coordination and not being able to use core (trunk muscle) tension to move or hold/sustain a movement properly. 20 Athletes and coaches described these symptoms as occurring before the onset of, or in the first few days of their period, which matches previously reported timing of negative symptoms during the late luteal and early follicular phases.19–21,35,47 Strength-sport athletes and coaches may benefit from further research investigating how the prevalence and experiences of MC-related symptoms and perceived changes in performance may acutely impact training decisions and management, and consequentially athlete physical adaptations and competition performance.
All athletes and coaches described adjusting training reactively to MC-related symptoms, with athletes describing adjusting load, exercise, or the days of training, based on autoregulation (i.e., RPE) once they started a training session. Previous research in strength-sport athletes has documented similar use of training manipulation in response to MC-symptoms to those discussed in our focus groups, indicating up to 70% of athletes adjusted their program, and of this proportion more than 80% typically altered load or volume. 27 Weightlifting athletes also mentioned lowering intensity, and preferring lower complexity exercises or swapping to accessory movements if MC symptoms were causing discomfort during training. 20 Research exploring other team-sport athletes’ tendency to make MC-related training adjustments suggests that up to 52% altered, and between 0–76% missed training or competition. 17 A higher propensity to modify or refrain from training seems to be associated with the late luteal or early follicular phases,19,47 higher prevalence or severity of symptoms,48,49 and lower level of athletic competition.21,27,50 Additionally, some research suggests that MC-phase or symptoms may have more of a perceived effect or reduced performance in high-intensity, higher absolute load or more technically challenging training.20,21,51,52
Coaches in our focus groups described MC-related changes to movement quality and athlete behaviour, and responded by making adjustments including reducing load, reducing movement complexity, or swapping exercises or sessions. It is worth noting that, although the specific adjustments to training in response to MC symptoms (e.g., modifications to load, timing, or volume) are relatively straightforward, the decision-making process is complex and shaped by non-MC factors, such as, coach preferences, competition phase, and the inherently individualised nature of exercise programming. Similarly, other research has reported that coaches adjust training plans or implement MC-related symptom coping strategies with athletes reactively, on an individual basis. 32 There are a number of ways to adjust training which considers both objective and subjective (perceived) performance. There has been increased attention given to a MC-phase-based training approach from coaches and athletes through social media, in response to anecdotal reporting, popular opinion, physiological theory, and some scientific data. 30 This phase-based training approach adjusts training variables based on theorised acute and chronic adaptations to resistance training, versus a symptom-based training approach, which requires athlete experience and education around the MC. 29 It is reasonable to suggest that the individual training and competition environment and coach-athlete dynamic in powerlifting and weightlifting would allow for easier MC-phase based manipulation of training, when compared to team-based sports. Interestingly, our data suggests that even when the context allows for proactive programming, or syncing training to MC-phase, elite level strength-sport athletes and coaches are not choosing to do this. This may be due to several factors, such as, its practicality, time-cost, or necessity due to the current debate around its evidence-base. There is not enough scientific evidence yet to support whether females require MC-phase specific training28,53 to optimise the development of muscle hypertrophy, strength, or power, and ultimately competition performance. Practices may be further complicated by the fact that research investigating the magnitude and the direction of MC effects on objective strength performance is mixed54–57 and thus often non-congruent with the perception of athletes, and dependant on sport, context, or prevailing conceptions. Collectively, our data suggests that better-practice management and planning of training likely involves a combination of both athlete autoregulation and coach-led adjustments, and considers the MC and related symptoms as a standard element of athlete monitoring alongside other common factors, such as, nutrition, fatigue, sleep, stress, and motivation.28,53
The coaches and athletes in our study highlighted the importance of acknowledging the MC, and monitoring MC-related symptoms, characteristics and wellbeing in conjunction with other physiological measures. All athletes in our study reported MC tracking, and both athletes and coaches deemed tracking to be important. Interestingly, there appears to be a wide range (22–75%) in the proportion of athletes who report tracking the MC across different sports.22,27 This variance in MC tracking may be due to the differences in perception around its utility or usefulness. One perspective, similar to the views of our participants, is that the MC can be an important vital sign, 58 with tracking providing a tool for a level of insight into an individual's MC. Simple tracking, through available apps or journalling, of period start date, bleeding length and flow, and symptoms (both positive and negative) can help females become aware of timing of onset of menstruation, impacts of symptoms and potential identification of menstrual irregularities or need for further investigation of dysfunctions when tracked longitudinally. 59 Additionally, tracking has been reported to increase awareness, initiate ongoing conversation, and offer insight into individual experiences, 60 and impacts on training and performance, allowing effective management strategies to be identified to adapt training and benefit performance.20,34 However, it is important to note that there are athletes who identify a lack of usefulness of tracking, or perceive a lack of use of the tracked information,34,35,39 as well as those who prefer an acceptance of symptoms, avoidance of data, and may even perceive ignorance as beneficial.20,21 Therefore, despite the potential benefits of the tracking and use of MC data to empower athletes, individual preferences to track or manage MC symptoms should also be considered, as well as an individual's autonomy, privacy and safety. 61
There appears to be a close link between education and communication about the MC, with athletes and coaches who had previously attended education sessions being more likely to have spoken about the MC or hormonal contraceptive use (92%) 38 when compared to others who had not (12%). 22 Participants in our focus groups shared similar opinions seen in previous research of a culture of not talking about the MC and it being considered a taboo topic,20,35,39 and limitations in knowledge and education,31,34,38,39 but had high interest in learning about the MC, as well as creating safe spaces to increase MC-related conversations and share experiences and knowledge. A general understanding of the complexities of biology, hormones, cultural, and environmental aspects of health and sport experiences, and how these interplay with other factors (e.g., stress, lifestyle, injury, illness, recovery, nutrition), 13 may help with opening up communication around, and normalisation of, the MC.
Research strengths and limitations
There are inherent strengths and limitations of focus group research and data interpretation which should be considered. Firstly, there are often power imbalances within groups, where one participant wishes to be heard above others, which may limit the ability of some participants to influence a discussion. 62 To overcome this, the facilitator started each focus group by laying ground rules, which included acknowledging the importance of everyone having an equal opportunity to engage within the discussion. Four participants (two athletes and two coaches) had prior substantive personal or professional relationships with the facilitator, which allowed for the recruitment of elite-level coaches and athletes. While pre-existing relationships may affect disclosure, potentially leading participants to present themselves in alignment with what they perceived to be the researcher's expectations, they can also enhance engagement and comfort. No information or bias regarding MC beliefs or strength training practices was shared before the focus groups. Additionally, although participation was voluntary, the purposive snowball sampling approach may have introduced bias, as participants might have been more open and interested in the MC than non-participants. Lastly, this study was based on a small, relatively homogeneous sample, and did not examine diversity within female athletes, such as choices around hormonal contraceptive use, perimenopausal or menopausal status, menstrual-cycle disorders (e.g., PCOS, endometriosis), or the influence of sociocultural factors (e.g., ethnicity, culture, religion, or age).
Summary and conclusion
This research provides considerable insight into the perceptions and training practices of elite strength-sport athletes and coaches throughout the MC. Elite strength-sport athletes’ experiences varied between individuals, however, all reported physical and psychological MC-related symptoms that were perceived to impact training. In response, athletes and coaches in this study discussed adjusting their training approaches, including reducing training intensity, by dropping load to meet prescribed RPE, changing movement patterns or complexity, or swapping training days. These decisions were based on athlete autoregulation, or made by coaches on a reactive, individualised basis, after assessing movement quality of their athletes throughout the session. Tracking MC-characteristics and symptoms through available apps was also discussed as a valuable tool in evaluating trends and making informed decisions around training. This included tracking period start date, bleeding length and flow, and symptoms. None of the athletes in the present study reported using calendar-based methods or hormone-testing kits. Although direct comparisons of MC tracking approaches were beyond the scope of this study, future research should more closely examine MC-tracking methods among female strength-sport athletes. The sporting environment allows a unique opportunity to disseminate knowledge and empower female athletes to become aware of MC impacts, and athletes and coaches discussed the importance of open and ongoing communication, knowledge sharing, and normalising discussions around the impact of the MC. This work may provide a framework to inform training strategies and practices throughout the MC to support health, wellbeing, and performance for female strength-sport athletes.
Supplemental Material
sj-docx-1-spo-10.1177_17479541261439786 - Supplemental material for Strength-sport athlete and coach perspectives and training practices throughout the menstrual cycle
Supplemental material, sj-docx-1-spo-10.1177_17479541261439786 for Strength-sport athlete and coach perspectives and training practices throughout the menstrual cycle by Brooke E Alvar, Dale M Harris, Steven J O’Bryan and André R Nelson in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-2-spo-10.1177_17479541261439786 - Supplemental material for Strength-sport athlete and coach perspectives and training practices throughout the menstrual cycle
Supplemental material, sj-docx-2-spo-10.1177_17479541261439786 for Strength-sport athlete and coach perspectives and training practices throughout the menstrual cycle by Brooke E Alvar, Dale M Harris, Steven J O’Bryan and André R Nelson in International Journal of Sports Science & Coaching
Footnotes
Acknowledgments
The authors would like to thank all coaches and athletes who generously gave their time, experiences and valuable knowledge to this study. Your contributions allowed this research to be possible and will enrich the understanding of this topic for the wider sporting community.
Ethical considerations
Ethics approval was granted by Victoria University Human Research Ethics Committee (HRE23-187).
Consent to participate
All participants provided written informed consent to participate, as well as verbal consent prior to the focus group interviews.
Consent for publication
Informed consent for publication was provided by all participants involved in the focus groups.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Victoria University (VU) Australian Government Research Training Program (RTP) Scholarship [DOI:![]() ].
].
Victoria University (VU) Australian Government Research Training Program (RTP) Scholarship,
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
De-identified data may be made available by request to the lead author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.