
Abstract
There has been an increased interest in the effects the menstrual cycle (MC) may have on sports performance. As a part of the MC, many females experience a wide range of symptoms related to hormonal fluctuations and menstrual bleeding, including physical pain and mood disturbances. Currently, there is a lack of data on the MCs of females who participate in resistance training. The dearth of information on the regular MC in female athletes may lead to poorly informed training recommendations which may be detrimental for female athletic advancement. The purpose of this survey was to determine the average MC characteristics, hormonal contraceptive (HC) use and perceived effects of the MC on training in resistance-trained athletes, and to determine if there are differences in these variables when comparing recreationally trained women to competitive-level athletes. A survey addressing questions about the MC, HC use and perceived effects of the MC was accessed by 906 participants who self-identified as resistance-trained athletes. Resistance-trained athletes, competitive or not, experience MCs similar to data on other exercising females and the general population. MC symptoms are widespread and, for some, can be quite severe and limiting. Competitive athletes were not more likely to experience MC irregularities than non-competitive females. Nearly half of the participants reported using HCs. Most participants perceived that their MC had a negative effect on their performance and that their MC caused reductions in training load or workout program adherence, although most competitive-level athletes did not withdraw from competitions due to MC symptoms.
Introduction
The hormonal fluctuations of the menstrual cycle (MC) cause a myriad of processes in the body linked to reproduction. In recent years, there has been an increased interest in the effects the MC may have on sports performance.1–4 A “normal” MC is approximately 22–35 days duration between menstrual periods in reproductive-age women. 5 A regular MC leads to a recurrent and cyclical process of rises and falls in estrogen and progesterone, and it is estimated that an individual will experience 451 MCs in their lifetime, starting from approximately age 12 to age 50 on average. 6 The MC can be considered a vital sign 7 and should be considered a crucial indicator of metabolic and physical health.7,8 As a part of their regular MC, many females experience a wide range of symptoms related to hormonal fluctuations and menstrual bleeding, including physical pain and mood disturbances. Over 90% of young women, girls and those who menstruate in Australia, 9 and almost three-quarters of young women worldwide 10 experience period pain (dysmenorrhea). Very little evidence suggests that MC symptoms reduce significantly with age, 11 hence most women will likely experience regular period pain at some stage in their life. In addition, it is perhaps unsurprising that menstrual symptoms such as period pain, and others such as heavy menstrual bleeding, reduced participation in sport10,12 in both the general population and athletes alike.
Previous research has found that 83–93% of female athletes experienced MC-related symptoms such as pain or heavy bleeding that may reduce training adherence or performance.13–15 There is evidence that exercising females may experience different length cycles or cycle irregularities and amenorrhea at higher rates than their sedentary counterparts. 16 The prevalence of irregularities in different populations of exercising females is important for establishing MC characteristics and for establishing MC effects on performance but at this point is not well documented in the literature. The dearth of information on regular MCs in female athletes may lead to poorly informed training recommendations which may be detrimental for female athletic advancement. Previous research has found that 50% of athletes perceived their MC had a negative impact on performance. 13 Therefore, further understanding all components of the MC, including the perception of its effects on exercise, is an essential component to account for MC effects as a whole.
Hormonal contraceptive (HC) use is another important topic that impacts the MC and potentially sports performance. 17 HCs create a unique hormonal environment that differs from the natural MC by using exogenous hormones to modulate the hormonal rises and falls normally seen in a natural MC. 18 Previous studies report that approximately 29.0–49.5% of exercising females worldwide use some form of HC for various reasons,13,14,19,20 but it is unclear if there are any sports discipline or specific factors that influence HC usage. As part of developing a complete understanding of the MC, it is imperative to establish the prevalence and role of HC use in different sports populations to understand the effects they may have on training and performance.
Previous surveys focused on MC-related symptoms and characteristics of team sport or endurance athletes, women performing mixed exercise types (resistance and cardiovascular) or a mixture of female athletes and exercisers.13–15,19 While previous information on MCs in athletes has been beneficial, there is a lack of differentiation of exercise and activity types in previous work. Resistance training is an important aspect of general exercise and is the primary training mode for strength sports. Strength-based sports include Olympic weightlifting, powerlifting, CrossFit, physique-based sports, throwing sports and other related strength-oriented competitions. Since resistance training and strength-based sports are based upon different training styles than endurance training the impact of any MC changes may be different in these sport types, as different areas of the body and training styles are used. For example, a reduction in explosive power due to MC changes may be more detrimental in throwing sports than in marathon running.
Currently, there is a lack of data on the MCs of resistance-trained athletes. Normative data on MC characteristics, including the prevalence of irregularities and HC use, in the resistance-trained population will better inform the effects of the MC on strength performance. Understanding athlete perceptions about MC effects is a substantial component in establishing any actual MC performance effects, but there is a lack of data in this area, specifically in the resistance-trained population. There has been an increase in popularity on the topic of adjusting resistance training programming around the MC, 21 but further normative data on the MC in the target population is necessary to better inform these theories and practices. Therefore, the purpose of this survey was to determine the average MC characteristics, HC use and perceived effects of the MC on training in resistance-trained athletes, and to determine if there are differences in these variables when comparing recreationally trained athletes to competitive-level athletes.
Methods
A survey was employed to explore MC characteristics and perception of the MC's effect on performance for resistance-trained athletes. Pilot testing undertaken with 10 athletes prior to survey launch included the understandability and appropriateness of the questions. Changes were made to the survey after this feedback and prior to the official launch of the survey. The final version of the survey was hosted on the Qualtrics Platform (Qualtrics Ltd, Provo, Utah, USA, March 2021). The cross-sectional online survey was anonymous, and participants were recruited via a social media recruitment poster distributed via the authors’ Instagram pages @helms3dmj and @kimsantabarbara which combined had approximately 135,500 followers. The original post had a reach of 35,866 accounts according to the Instagram-provided post analytics and was then re-shared over 195 times across multiple powerlifting and strength athlete-based accounts. After participants viewed the recruitment poster on social media they could choose to follow a link to the survey, which began with an information page with the purpose and objectives of the survey as well as an explanation of any potential risks and benefits from participation. Participants were informed that they were giving their consent to participate by moving forward with the online questions. Interested participants could then click a “continue” button which demonstrated their consent to participate in the anonymous survey if they chose to do so. The survey took most participants between 10 and 20 min to complete and was made available from April 2021 until June 2021. This research was approved by the Auckland University of Technology Ethics Committee on 5 March 2021 (AUTEC reference number 21/22).
Procedures
Participants completed the anonymous survey comprised of 79 questions. The survey had five sections: participant demographic/background information, MC characteristics, HC use and characteristics and perceptions of MC effects. Demographic and background information included questions on age, experience with resistance training, including competitive level (if applicable), other types of training they participated in and their geographic location. The MC characteristics section included questions about period regularity and MC symptoms, timing and severity. The HC section included questions on the type of HC used, the main purpose for their use, duration of use and any experienced side effects. The perception of MC effects section included questions about perceived positive or negative effects on performance, their timing and severity. In the section on MC effects, participants were specifically asked if they felt their workouts were affected by their MC, giving the participant the choice to identify any part of their MC, such as the menstrual period or pre-menstrual time frame.
Subjects
Participant inclusion criteria were females aged 18–53 who self-identified as not having experienced menopause. Participants self-identified as currently participating in a high level of resistance training and primarily participating in resistance-training exercises over any other exercise types. They participated in full-body resistance training and trained at least two times per week, and had at least a two-year training history. A current and regular MC was not an inclusion criterion as it was considered important to establish an accurate depiction of the frequency of amenorrhea in the target population. Participants who considered themselves to be competitive-level athletes were asked to self-identify as such, the criteria being that they actively competed in a strength-based sport, including Olympic weightlifting, powerlifting, CrossFit or a physique-based sport regardless of their level or experience. These participants were considered “competitive-level athletes” to differentiate them from recreational-level athletes for analysis. Based on the criteria outlined by McKay and colleagues on defining training caliber, 22 the competitive-level athletes in this survey would be classified as Tier 3 and above and the recreational-level athletes would be classified as Tier 2.
Statistical analysis
Descriptive data, including means, frequencies, standard deviations (SD), modes, percentages and ranges were reported for each section to establish normative data in this population. Chi-square tests were used for group comparisons, specifically for analyzing differences in competitive-level athletes compared to recreational-level athletes for MC characteristics, HC use and MC perceptions for categorical data as well as for group comparisons between HC users and nonusers. Strength athletes were defined as any participant who indicated they were competitive in a strength sport, regardless of competitive level. Effect sizes were calculated with Cramer's V. Effect sizes were reported with degree of freedom of 1 ≥ 0.1 represents a small effect, ≥0.3 represents a medium effect and ≥0.5 represents a large effect, degree of freedom of 2 ≥ 0.07 represents a small effect, ≥0.21 represents a medium effect and ≥0.35 represents a large effect, degree of freedom of 3 ≥ 0.06 represents a small effect, ≥0.17 represents a medium effect and ≥0.29 represents a large effect. 23 Incomplete or missing data (unless the missing data was in the optional nutrition section) were excluded from final analyses. Significance was determined at the p ≤ 0.05 level. All statistical analysis for this research was performed using JASP Team (Amsterdam, The Netherlands, 2023). JASP (Version 0.17) (https://jasp-stats.org/) computer software for Mac.
Results
Demographic and background characteristics:
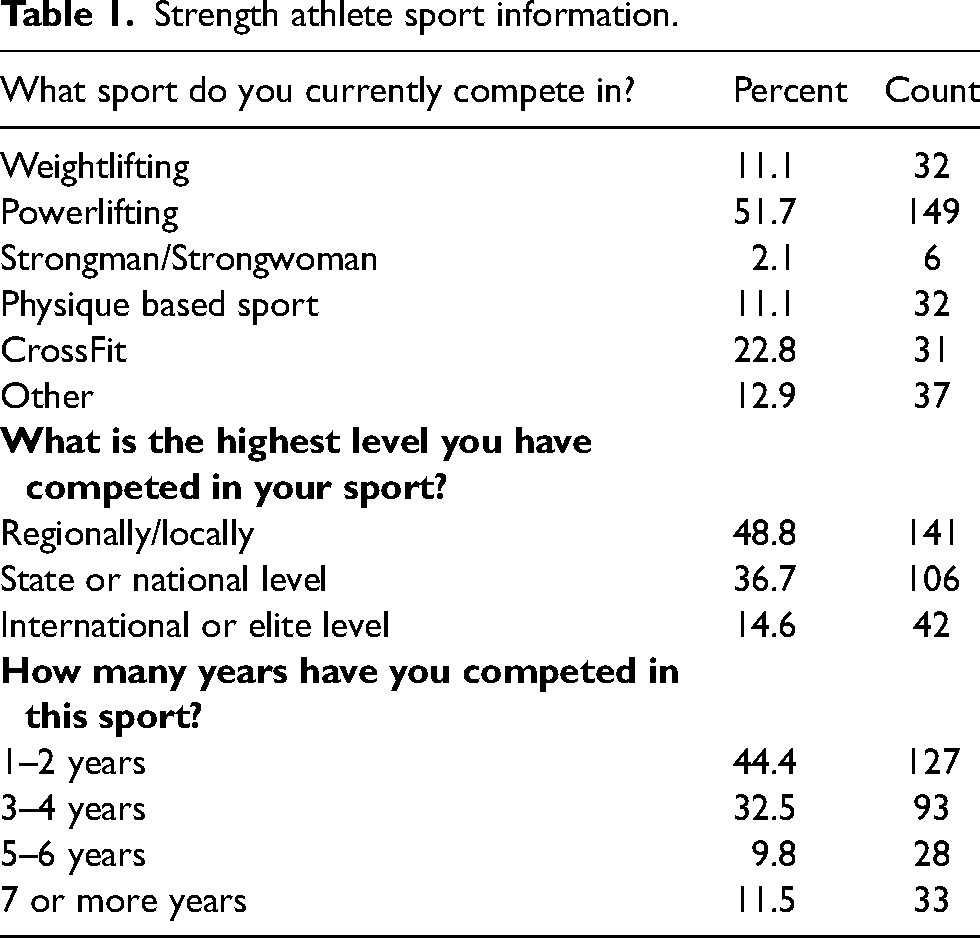
Nine hundred and six participants accessed the survey online. Participants who did not meet the survey criteria were removed, leaving 809 responses that were analyzed. Participants ranged in age from 18 to 48 years, with a mean age of 27 ± 5.95 years and most commonly had been doing resistance training for 6–10 years (30.5%). Hours of weekly participation in resistance training ranged from 1–2 h per week (2.7%) to 7 or more hours per week (31.1%), with most participants training 5–6 h weekly (44.5%). A total of 267 participants (33%) self-identified as competitive-level athletes with most of these athletes competing at the regional or national level (88.3%). Further information on competitive athletes is shown in Table 1. Participants from 53 countries completed the survey with the following breakdown: a majority (57.5%) from the USA, followed by New Zealand (7.7%), the UK (7.1%), Canada (7.0%), Australia (5.4%), Europe (7.0%) Asia (2%), the Middle East (2.0%), Latin America (1.0%) and Africa (0.5%).
Strength athlete sport information.
MC characteristics:
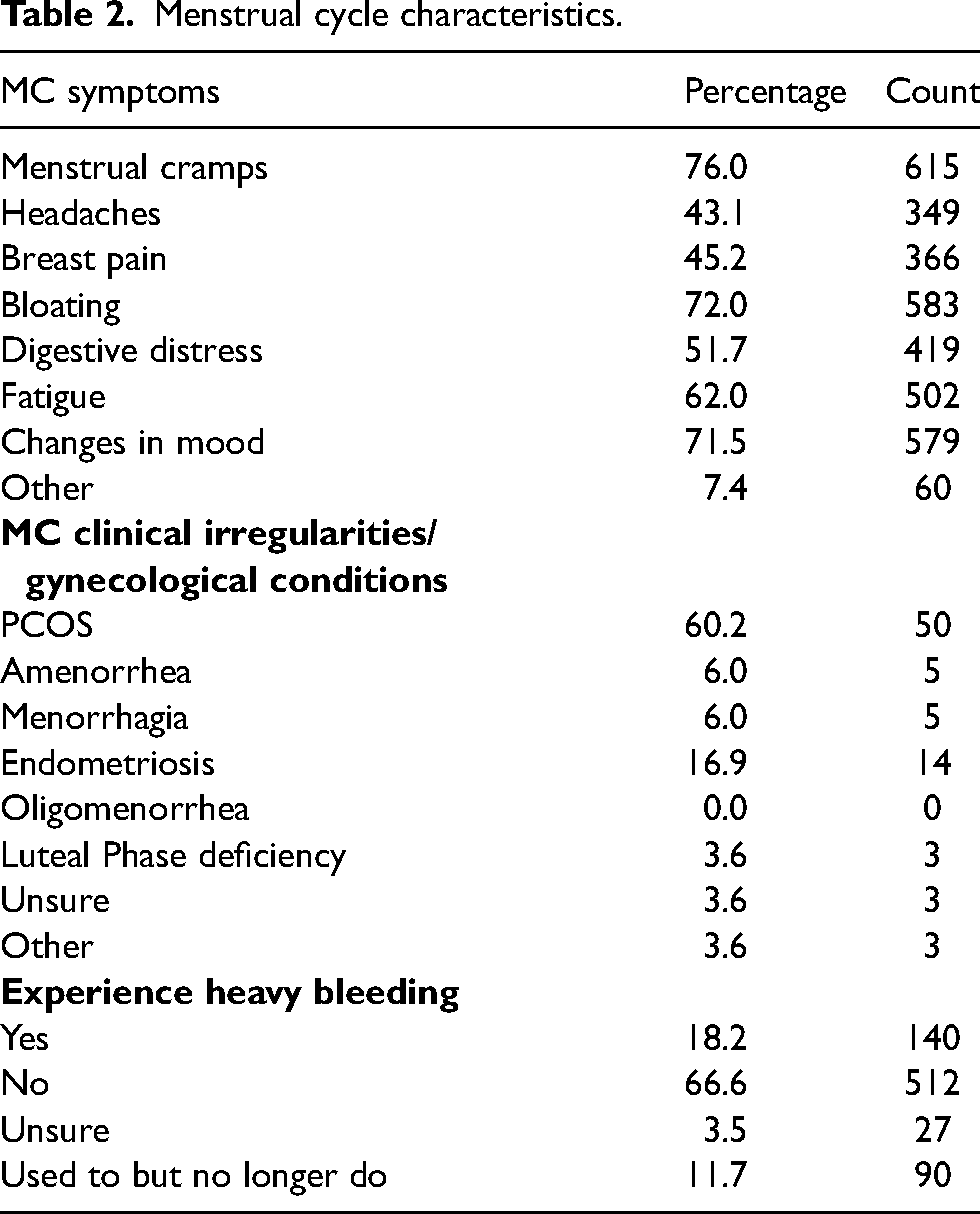
The mean age of menarche reported in this population was 13 ± 1.7 years; the mode of reported menarche age was 12. Most participants (68.3%) answered that their periods came regularly, with (72.7%) reporting that their MC lasted 25–31 days. Strength athletes were comparable, with 68.1% indicating that their periods came regularly and 75.7% reporting that their MC lasted 25–31 days. There was no significant association between number of hours of training per week and MC regularity (p = 0.69). More detailed information on MC characteristics and irregularities is in Table 2. 11% of participants reported experiencing amenorrhea in the last two years due to factors connected to low energy availability (such as physique contest preparation, dieting, excessive training, etc.). There was no significant association between hours of training per week and experiencing amenorrhea (p = 0.661). 5.6% reported they were diagnosed by a healthcare provider with amenorrhea, and 9.3% of participants with a MC irregularity, with polycystic ovary syndrome (PCOS) being the most common irregularity diagnosis. Competitive-level athletes had a similar frequency of MC irregularities (8.8%). There was no significant association among competitive-level athletes and MC irregularity diagnosis (p = 0.664). 75.3% of participants tracked their MC using an app or calendar counting. 92% of participants stated they experience MC-based symptoms, with uterine cramps the most cited symptom (76%). HC use was associated with a lower likelihood of MC symptoms overall (p < .001) with a small effect (effect size = 0.167) and specifically a lower likelihood of cramps (p < .001) with a small effect (effect size = 0.147). Participants indicated their worst symptom severity was 5.47 ± 1.9, on a pain scale from 1 to 10. Most (76%) of participants indicated they did not experience iron anemia. A complete breakdown of symptoms and related details is found in Table 2.
Menstrual cycle characteristics.
HC characteristics
40.2% of participants indicated they use HCs. The combined oral contraceptive pill was the most common (43.8%). A majority (67%) indicated they had used this HC method for over two years. Fewer competitive-level athletes used HC (38.4%). The most common reason for HC use was for contraceptive purposes (72.8%), and the second most common reason was for MC symptom relief (13.7%). 45.4% of participants believed their HC caused unwanted side effects. Figure 1 displays further HC information.
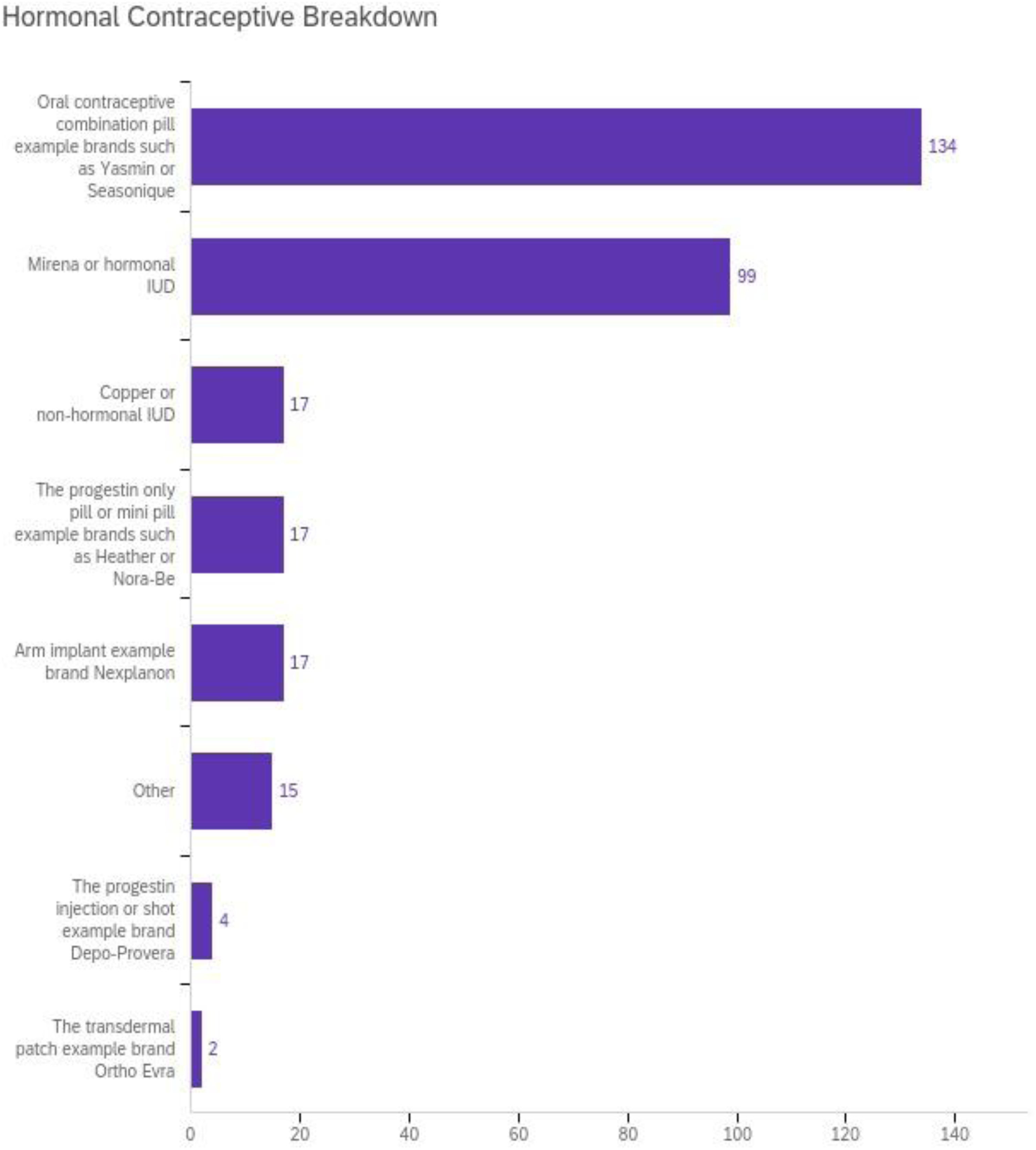
HC type.
Perception of MC effects:
59.4% of participants perceived their MC had a negative impact on training or performance, but 46% perceived their MC had a positive impact on performance. Most participants cited the negative impacts on performance occurring in the days leading up to menstruation or during menstruation (89.5%), and 38.0% perceived the positive effects to occur in the week after mensuration. The most reported negative effect was fatigue (43.4%), and the most reported positive effect was feeling stronger (34.8%).
Competitive-level athletes were comparable, as 64.9% perceived their MC had a negative impact on performance, and 38.0% perceived their MC had a positive impact on performance; there were no significant associations between competitive-level athletes versus recreational-level athletes and the perception of negative MC impacts on performance (p = 0.080) or positive impacts on performance (p = 0.954).
69.5% of participants altered their program due to MC symptoms, with decreasing load or volume as the most cited alteration (83.3%). Competitive-level athletes were significantly less likely to alter their training due to their MC (p = 0.008) with a small effect (effect size = 0.145) compared to recreational-level athletes. Only 1% of competitive athletes had ever dropped out of a competition due to MC-related concerns.
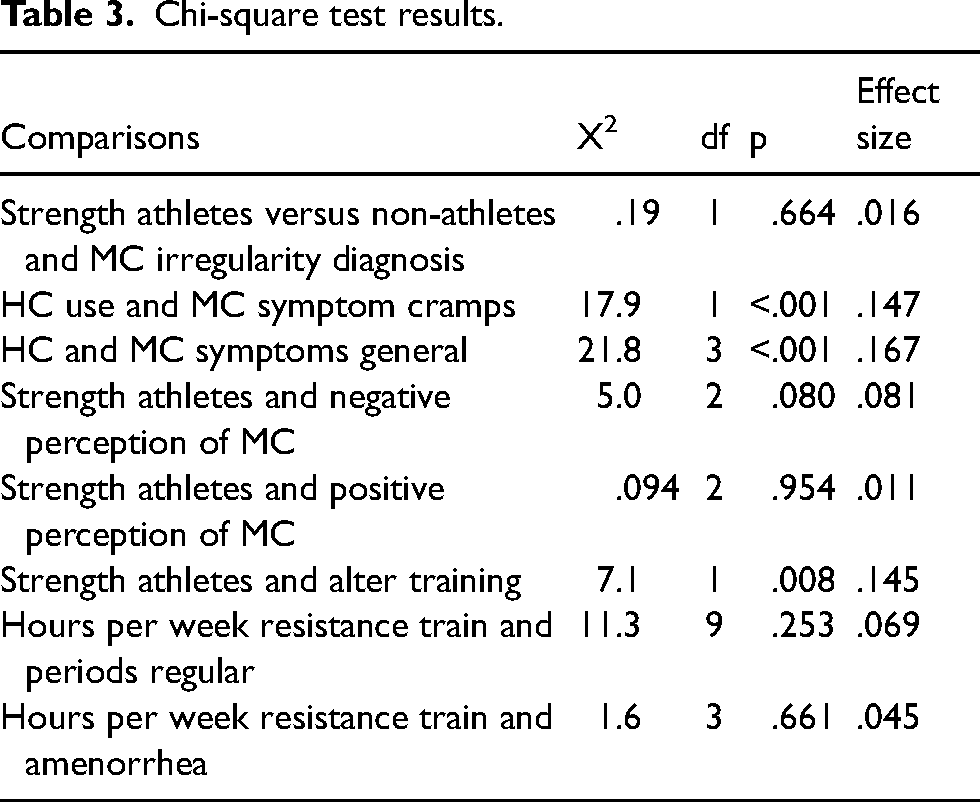
85.7% of participants felt comfortable discussing their MC with their coach. The most cited reason for not discussing their MC with their coach was that their coach was male (72.7%). Competitive-level athletes were slightly more likely (90.5%) to feel comfortable discussing their MC with their coach. See Table 3 for all Chi-square test results associated with this data set.
Chi-square test results.
Discussion
This survey focused on MC characteristics, HC use and perception of MC effects on training and performance among females who participate in resistance training both competitively and non-competitively. Like the broader population, participants reported high rates of MC-related symptoms, and slightly less than half used a form of HC. However, contrary to existing research on other exercising women, most participants reported regular MCs. Further, most participants perceived that their MC had a negative effect on their performance. However, in those who were competitive-level athletes, a vast majority indicated that they had never dropped out of a competition due to MC symptoms. Besides this difference, competitive and recreational-level lifters in the present sample reported similar MC characteristics, symptoms, and symptom severity levels.
The findings from this study on MC regularity align with previous related research on MCs among the general female population 24 and contrast research on females performing general exercise. 16 De Souza et al. 16 used active hormonal monitoring to categorize MC regularity rather than memory recall (the method used in the present survey) which may explain the contrasting findings. Therefore, further investigation is warranted regarding the prevalence of MC irregularities and their effects on performance among resistance-trained women, specifically using hormonal monitoring techniques.
In line with previous surveys showing that a vast majority of exercising females experience MC symptoms13,14 92.0% of our respondents reported experiencing MC symptoms as well. Cramps were the most listed symptom (76.0%), and most reported symptoms occurred at the end of the luteal phase and/or the beginning of the menstrual period (91.6%). These findings align with research on other types of athletes as well, as the timing and type of observed MC symptoms were similar in studies on runners and swimmers.12,25 The pain severity of symptoms in this current study was also notable, with most participants listing their worst symptoms as a mean of 5.5 on a scale of 10, or “moderate” on the pain scale. Previous research has shown that this pain severity level may impact one's physical capability for multiple days every month, causing them to miss important activities of daily living, including training. 9 Indeed, competitive-level athletes or their coaches may benefit from considering MC pain severity when programming training. Understanding the breadth and intensity of MC symptoms can improve the effectiveness of coaching for female athletes and the individual experiences of athletes by providing context and validation for real-life experiences.
The high prevalence of HC use found in this study aligns with some previous findings, with close to half of the participants utilizing some form of HC and a majority using combined oral contraceptive pills.13,20 However, the present findings differ from a recent survey which found relatively low HC use (approximately 10%) in a women's football group surveyed in South Africa. 26 The authors attributed this lower level of HC use to cultural and socioeconomic differences in the region. 26 Other previous research has shown that HC use varies widely across countries and regions worldwide. 27 Notably, the present survey was primarily composed of participants from similar culturally Westernized countries (84.7% of respondents were from the US, UK, New Zealand and Australia, combined). Therefore, when there is a difference in HC use prevalence between regions as possibly indicated by some data, researchers should be aware of these contextual differences when generalizing HC use among athletic populations globally.
Another important finding of this study is the high prevalence of side effects from HC use. 45.0% of participants in this survey indicated they experience some sort of HC side effect. Despite this large percentage of reported side effects from HC use, HC use was associated with a lower likelihood of experiencing MC symptoms overall, including cramps specifically. Similarly, in prior research, 40% of elite female athletes who used HCs also perceived that HCs caused adverse side effects. 20 Of note, many females are prescribed HCs to alleviate their MC symptoms.18,19 While the present survey supports the notion that HCs may alleviate MC symptoms for some individuals HC use alone may not be a sufficient remedy for all who experience MC symptoms since a large number may still experience some level of unwanted side effects specifically from HC use. Ultimately, whether the trade-off of MC symptoms for HC-related side effects is worth it, resulting in a net improvement, warrants further investigation. Further research is also needed to discover new antidotes for MC symptoms that produce a lower rate of unwanted side effects.
Most participants perceived that their MC negatively impacted performance (59.4%), specifically during the late luteal phase or the onset of the menstrual period. This is slightly higher than previous related research on marathon runners, where 41.7% perceived that their performance was negatively impacted by their MC. 12 However, the present rates are similar to those reported (65.6%) in previous research on a mixed group of elite athletes. 28
In the present study, fatigue was the most commonly cited negative side effect (62%) that impacted training. This finding aligns with research on other athletic populations of females that found that fatigue was a common MC symptom impacting performance.12,19 In the present study, a considerable number of participants indicated that they made alterations to their training due to their MC (69.5%), with reducing load or volume being the most common alteration. The prevalence of MC-based fatigue is important for the athlete and coach to be aware of. Like pain, fatigue may also need to be considered prospectively for workout programming, as fatigue may prompt training load and volume reductions.
Although more than half of competitive athletes perceived that their MC affected performance during competition, only 1% reported dropping out of a competition due to their MC. This is mirrored in a survey of competitive athletes, where most high-level athletes reported negative side effects related to their MC, but only 4.2% reported refraining from exercise during specific times of their MC. 20 This finding may demonstrate that although competitive athletes often experience the same level and intensity of symptoms as the general exercising population, their competitive drive may override the desire to refrain from exertion, especially for a one-time event like a competition. This finding aligns with previous research on athletes, which found many athletes are willing to push through pain due to passion for the sport, athletic identity, normalization of pain in sports and external expectations to perform under all circumstances.29,30 This interesting difference between exercising women and female athletes in the present survey warrants further research to explore the connection between perceived MC impacts on performance, and the actual measured performance effects of the MC itself.
Most participants felt comfortable discussing their MC with their coach, but 14.0% did not, primarily due to their coach being male. This finding is echoed by Martin et al. 31 and Findlay et al., 15 as both reported that most female athletes were comfortable speaking about their MC with their coach, but not all felt this way. Since MC symptoms are common, it is crucial that all athletes with MCs are comfortable enough to speak to their coach about their symptoms, regardless of their coach's gender or sex. To facilitate such critical communication, male coaches can take the initiative to educate themselves on the topic of the MC in sport to encourage an open dialogue and give the athlete space to express concerns they may have surrounding their MC and performance.
Limitations of this research:
Since this was a cross-sectional survey based on memory recall of events, answers are subject to recall bias. Another limitation of this research is that participants self-identified their level of participation in resistance training, including their experience, competitive level and history. Therefore, the findings may not be an accurate representation of differences between (and characteristics of) recreational and competitive-level athletes. Many participants also reported participating in other types of physical activity, including cardiovascular training and team sports, making these findings potentially more varied than might be reported by a group of exclusively resistance-trained athletes.
Conclusion
Females who participate in resistance training, competitive or not, experience MCs similar to data on other exercising females, and the general population. MC symptoms are widespread and, for some, can be quite severe and limiting. In this study, MC irregularities were not more common in females who participated in resistance training compared to data on other exercising females, and PCOS was the most cited irregularity. Competitive-level athletes were not more likely to experience MC irregularities than recreational-level athletes. Nearly half of the participants reported using HCs, with the combined oral contraceptive pill the most used form. Most participants perceived that their MC had a negative effect on their performance and that their MC can cause reductions in training load or workout program adherence, although most competitive-level athletes did not withdraw from competitions due to MC symptoms. As research continues to uncover more details about the mechanisms behind these MC experiences, future investigations should focus on solutions. In the meantime, an understanding and individualized response to the fatigue, pain and other difficult MC symptoms is likely the best approach.
Footnotes
Data availability statement
The full data set from this survey can be made available by request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.