
Abstract
Rugby union exhibits large variations in the idealised player physical profiles across positions. The pursuit of physique ideals with limited professional support can influence eating disorder symptomology, exercise compulsion, and low sexual drive. The primary aims were to (1) explore the prevalence of elite male rugby union players who are at risk for eating disorders, low sex drive, and exercise compulsion, and (2) explore the relationship between risk and players’ professional status, weight, age, and playing position. A secondary aim was to explore the nutritional service support and dietary monitoring practices experienced by the players. Participants were recruited from four elite professional rugby union squads in Ireland. Players (≥tier3) over 18 years of age and training ≥ three times per week were eligible. Participants completed the eating disorder examination questionnaire, exercise addiction inventory, and sex drive section of the low energy availability in males questionnaire. Ninety-seven players participated in the study. The mean age of participants was 22 ± 4 years. Eating disorder risk (9.3%), reported low sex drive (20.6%), and exercise compulsion (16.5%) was indicated. Players in the forwards position, regardless of professional status, reported higher eating concerns (p = 0.03). No significant difference was identified between professional status or position when determining sex drive. Access to a nutritionist (99%) and dietary monitoring practices (68%) was reported by players. Awareness of low sex drive and disordered eating in elite rugby should be encouraged, alongside access to professional nutritional support. Further research is needed to understand the contextual risk factors in male players.
Introduction
Athletes often shift their eating behaviours knowingly or unknowingly throughout periods of their career e.g., the pathway development stage, pre-season or injury. Dietary change may lead to disordered eating behaviours that include short-term restrictive diets, compulsive eating, or irregular eating patterns, with or without excessive exercise beyond assigned training. 1 While these behaviours may not meet clinical thresholds, they can evolve into diagnosable eating disorders that are mental illnesses with defined criteria characterized by abnormal eating behaviours such as self-induced restriction of food intake, preoccupation with body shape or weight, and bingeing and purging. 1 Eating disorders and excessive exercise are associated with serious mental health consequences, including depression and anxiety, and can lead to long-term health risks that persist beyond an athlete's career. 2 While appropriate athlete dietary patterns guided by professional nutritionists or athlete dietary self-monitoring practices may facilitate athletic development and optimise health, there is also a risk of inappropriate dietary change, compulsive exercise, disordered eating behaviour, or eating disorders, which may contribute to potential disruption to energy availability (EA), a key determinant of nutritional status. 2
Prolonged EA disruption may result in low energy availability (LEA) and a mismatch between dietary energy intake and the energy expended in exercise that leaves the body's total energy needs unmet.3,4 The degree of disruption crosses a continuum from adaptable LEA (benign and readily reversible) to problematic LEA, presenting greater and potentially persistent disruption to various physiological and psychological body systems. Symptoms include fatigue, anxiety, low motivation, low sex drive, stress fractures, and disrupted sleep.3,5 These interconnected concepts of LEA, disordered eating, eating disorders, and the related physiological and psychological symptoms of low sex drive and compulsive exercise may co-occur or exist in isolation. 6 To limit risk, sporting organisations may gain the support of nutritionists to influence athletes’ nutritional knowledge, evoking appropriate dietary behaviours.7,8 However, the degree of prevalence and etiology of risk may often emerge from a myriad of factors such as psychological and socio-cultural (peer pressure, weight stigma, physique ideals), professional status or attempts in attainment, sport-specific pressures, and the frequency and level of access to psychological and nutritional support.5,9
Male team sport athletes, particularly rugby union players, may be a high-risk group in the development of disordered eating behaviour and eating disorders, 10 because of the strong association with masculinity and physique norms. 11 Players exhibiting a variation in “idealised” anthropometric and physique profiles across two positional groups. Forwards (front row, second row, back row) are typically taller, heavier, and possess more muscle and fat mass, whereas backs (half backs, centres, wings/fullbacks) are lighter, faster, and cover higher speed. 12 Notably, players’ body mass may range from 70 to 140 kg, with the average body mass of professional forwards increasing from 103 kg in 1991 to 113 kg in 2019 13 which may risk weight stigmatisation in the sport and drive body size concerns for players. The ceiling for a player's physique is often related to coaching intent in sports. The ‘physique culture’ of attaining these typical profiles at an early age (usually commenced at a vulnerable adolescent age for influence within an elite development pathway) has been associated with players’ progression from amateur to elite professional level. 14 There has been a paucity of research indicating physique concern differences between forwards and backs in attaining these profiles, although higher eating concerns have been reported among professional forwards. 15 In addition, the maintenance of a required positional physique at the professional level considering the games’ high energetic needs16,17 and physique cultural “norms” may influence risk behaviours such as disordered eating practices, excessive exercise, overtraining, and mask-associated symptoms of suboptimal EA, including low sex drive. These risks may be exacerbated without professional nutritional support. 8 To monitor associated risk and symptomology, the International Olympic Committee's (IOC) relative energy deficiency in sport (REDs) clinical assessment tool version 2 (CAT-2) outlines a step-wise approach, with the initial use of self-reported screening tools, with a more expansive investigation recommended if prevalence is indicated. 18
To date, no research has investigated the risk prevalence rates and relationships between eating disorders, low sex drive, and compulsive exercise, as well as contextual factors such as nutrition support and energy monitoring practices in an elite sports population that exhibit markedly diverse anthropometric profiles. Considering the ‘physique culture’ within elite rugby union, the primary aims of the present study were to 1) explore the prevalence of elite male rugby union players scoring at risk for eating disorders, low sex drive status and exercise compulsion, and 2) explore the relationship between risks and a players’ professional status, weight, age and playing position. A secondary aim was to explore the nutrition service support and energy monitoring practices experienced by players to contextualize the results.
Material and methods
Design and data collection
A cross-sectional study design was adopted and an online questionnaire was used to collect self-reported data in English using Microsoft Forms (Microsoft 365, Redmond, WA, USA). The online questionnaire was available in English and was open for responses between November 2023 and March 2024. Methodological procedures followed the Checklist for Reporting Results of Internet E-Surveys, 19 as outlined in Supplementary Material 1. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and approved by the Technological University Dublin Research Ethics Committee (REC 22-62).
Study settings and participants
The participants were elite male rugby union players recruited from four professional clubs in Ireland representing senior, academy, or pre-academy squads. Professional players were defined as those under an academy or senior contract and paid to play, while non-professional players were defined as those not under contract and unpaid and training in the clubs’ pre-academy squad with the aim of obtaining professional status. The eligibility criteria for inclusion were: (1) elite male rugby union athletes (15-a-side) classified as ≥tier 3 according to McKay et al.; 20 (2) aged 18 years or older; and (3) engaging in training at least three times per week. To maximise representation, all eligible players across the four clubs were invited to participate. An initial invitation email was sent to key stakeholders (e.g., performance managers) acting as gatekeepers. This email outlines the study's purpose and inclusion criteria. Gatekeepers, following signposting of the study to all players within their respective club therefore ensuring maximum reach, then distributed the participant information sheet and the URL link to the online questionnaire to interested players with a password to access the survey. Before beginning the survey, the participants were presented with an information sheet and a screening question to confirm eligibility. If the participants did not meet the eligibility criteria, the survey was ended. Informed consent was obtained through the voluntary and anonymous completion of the questionnaire.
Online questionnaire design
The online questionnaire (see Supplementary Material 2) comprises 71 items, incorporating both validated instruments outlined in the IOC REDs CAT2 used as proxy LEA indicators, and self-constructed questions. The validated instruments included were the Eating Disorder Examination Questionnaire (EDE-Q) version 6.0 (28 items), 21 Exercise Addiction Inventory (EAI) (6 items), 22 and sex drive section from the low energy availability in males questionnaire (LEAM-Q) (4 items). 23 An additional thirty-three self-constructed questions captured information on participant nutrition service support, dietary monitoring practices (8 items) and participant background characteristics (25 items). The questionnaire incorporated a completeness check. Participants could review and modify their responses using a back button prior to submission. Only fully completed questionnaire were included for analysis. The questionnaire was piloted with three male rugby players to assess the completion time and confirm the clarity and comprehension of all items.
Eating disorder risk
Eating disorder risk was assessed using the EDE-Q, 21 which evaluates symptoms across four subscales: restraint, eating concerns, shape concerns, and weight concerns. The EDE-Q is a validated tool for use within adolescent male athletes. 24 A global score was calculated by averaging the four subscales, with a cut-off of ≥1.68 used to indicate elevated eating pathology in males, in line with the recommendations of Schaefer et al. 25 The EDE-Q score demonstrates disordered eating pathology. Players demonstrating higher EDE-Q scores may lead them to develop clinical eating disorders, rather than being interpreted as a risk stratification tool for eating disorders. It must be noted, a higher EDE-Q score does not directly put the player at an higher risk of an eating disorder in the future, but rather is reflective of their current eating behaviours.
Exercise compulsion
Exercise compulsion was measured using the EAI, 22 where scores ≥24 indicate a risk of compulsive exercise, scores of 13–23 suggest the presence of some symptoms, and scores of 6–12 indicate no symptoms. The EAI has demonstrated good internal reliability among elite-level athletes. 26
Low sex drive
Low sex drive was evaluated using four items from the LEAM-Q. 23 Criteria for low sex drive included reporting any of the following: morning erections ≤2×/week in the past month; decrease in the number of morning erections in the past month compared with baseline; low sex drive or lack of interest in sex; sex drive reduction in the past month or decrease in sex drive when training volume increases. The scoring was performed as described by Lundy et al. 23
Statistical analysis
All statistical analyses were conducted using the statistical software SPSS V.29.0 (IBM, Armonk, New York, USA). Data are presented as means, standard deviations, or percentages. Both sub-scales and global scores are presented where possible. Participants were categorised by professional status (professional/non-professional) and further stratified by playing position, weight, and age. Prevalence, the primary outcome of the study, was determined using descriptive statistics based on the percentage of participants at risk of eating disorders, low sex drive, and exercise compulsion. Associations between categorical variables were evaluated using the chi-square test to determine whether the risk of low sex drive, exercise compulsion, and eating disorders differed according to professional status, body mass, age, and playing position (back or forward). Group comparisons for non-normally distributed data were conducted using the Mann-Whitney U test to determine whether the EDE-Q subscale scores differed based on position category or professional status. Internal consistency among the applied measures was assessed using Cronbach's α, with values >0.70 considered acceptable. 27 To reduce the probability of any type 1 error, the alpha level for statistical significance was set at 0.05. Spearman's rank correlation was used to assess the relationship between EDE-Q and EAI scores. Because the target group in the current study was the entire elite male rugby union player population available in Ireland, no power calculations were performed. The results of the statistical analysis were interpreted in the context of the exploratory nature of the study.
Results
Participants
Of the 285 elite male rugby union players eligible, 34% (n = 97) completed the questionnaire fully, of which 54.6% (n = 53) were professional and 45.4% (n = 44) were non-professional (Fig. 1). The mean age of the participants was 22 ± 4 years, with a mean body mass of 99.6 ± 12.9 kg. The highest competitive playing levels reported included category tier 4: international senior 15 s (n = 10), international senior 7's (n = 4), international age grade (n = 55), and category tier 3: senior professional club (n = 36), senior club (n = 1), and university (n = 1), based on the classification by McKay et al. 20 The demographic characteristics of the participants are summarized in Table 1. Table 2 presents the prevalence data for participants who scored above the threshold cut-offs for the EDE-Q, EAI, and sex drive section of the LEAM-Q. The internal consistency for the EDE-Q and EAI is reported in Table 3. Additional descriptive data of scores for the EAI and EDE-Q are presented in Supplementary Material 3.
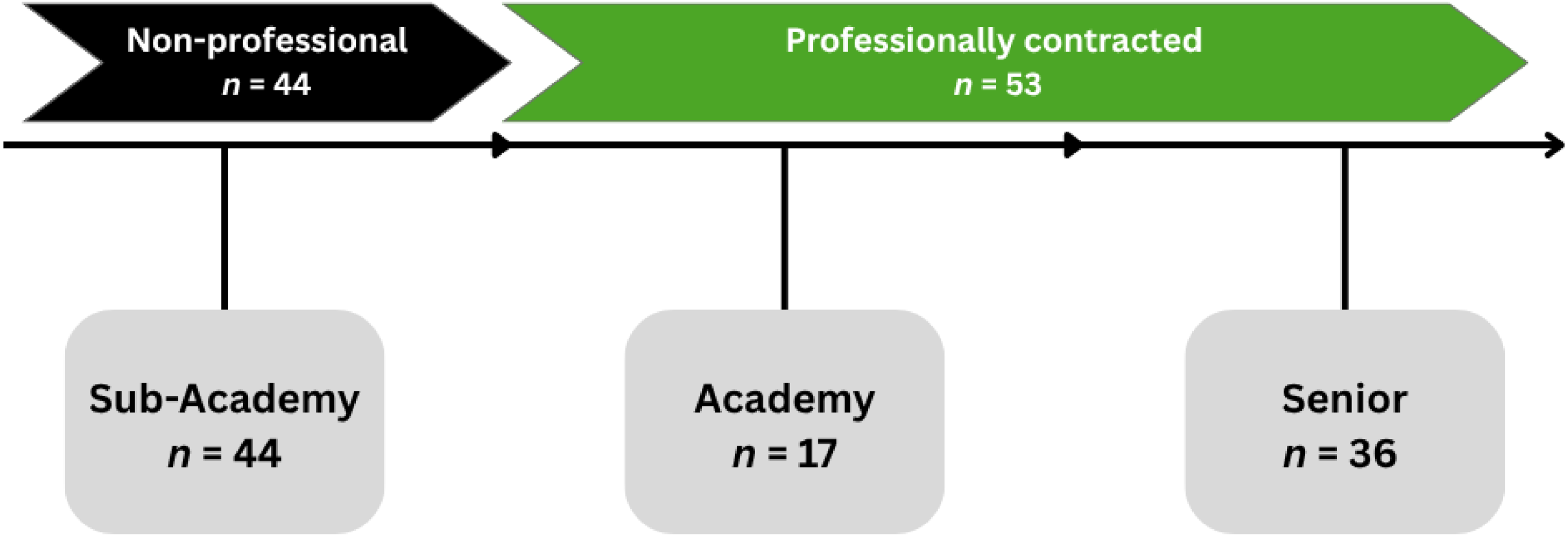
Participant professional status visualised along the trajectory of the elite male rugby union player pathway stage in Ireland. Note: n, number of participants denoted from each stage.
Demographic information of participants.
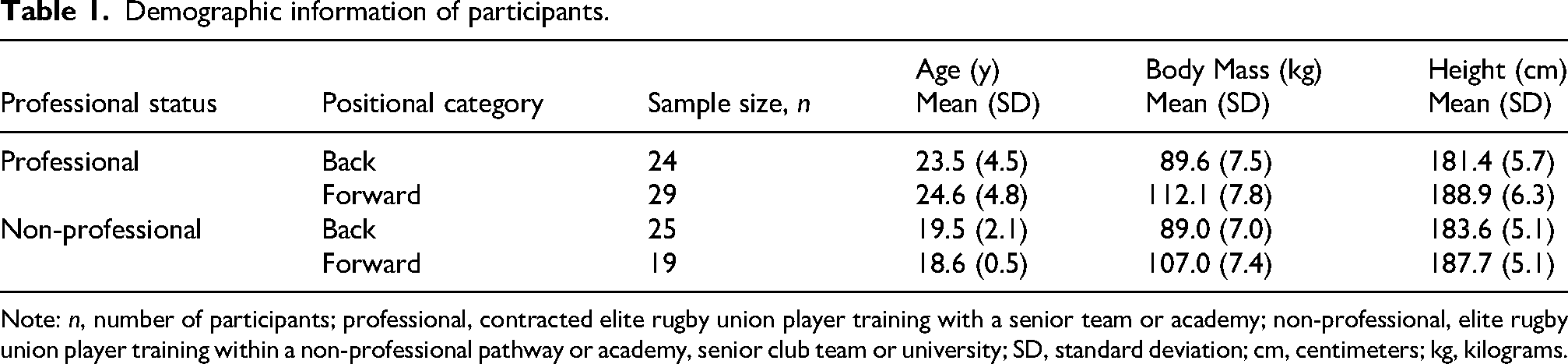
Note: n, number of participants; professional, contracted elite rugby union player training with a senior team or academy; non-professional, elite rugby union player training within a non-professional pathway or academy, senior club team or university; SD, standard deviation; cm, centimeters; kg, kilograms.
Participants presenting with scores above the threshold cut-off for low sex drive, eating disorder risk and exercise compulsion.
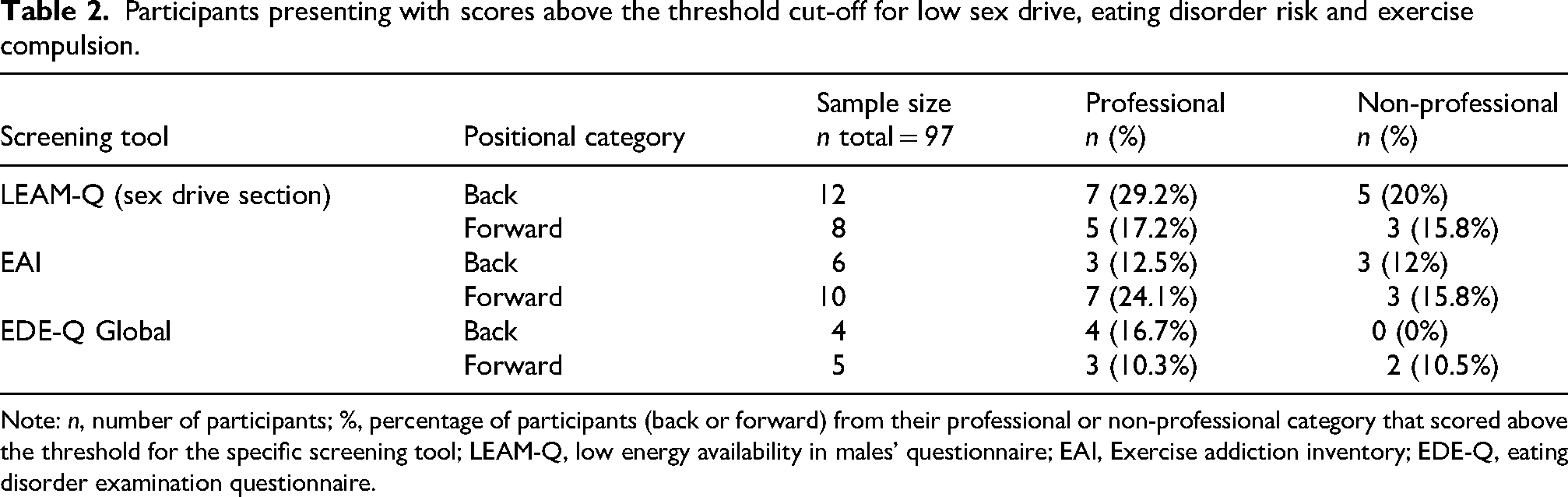
Note: n, number of participants; %, percentage of participants (back or forward) from their professional or non-professional category that scored above the threshold for the specific screening tool; LEAM-Q, low energy availability in males’ questionnaire; EAI, Exercise addiction inventory; EDE-Q, eating disorder examination questionnaire.
Internal consistency (Cronbach's α) and mean scores given players’ playing position for the global scores of the exercise addiction inventory and the eating disorder examination questionnaire and subscales.
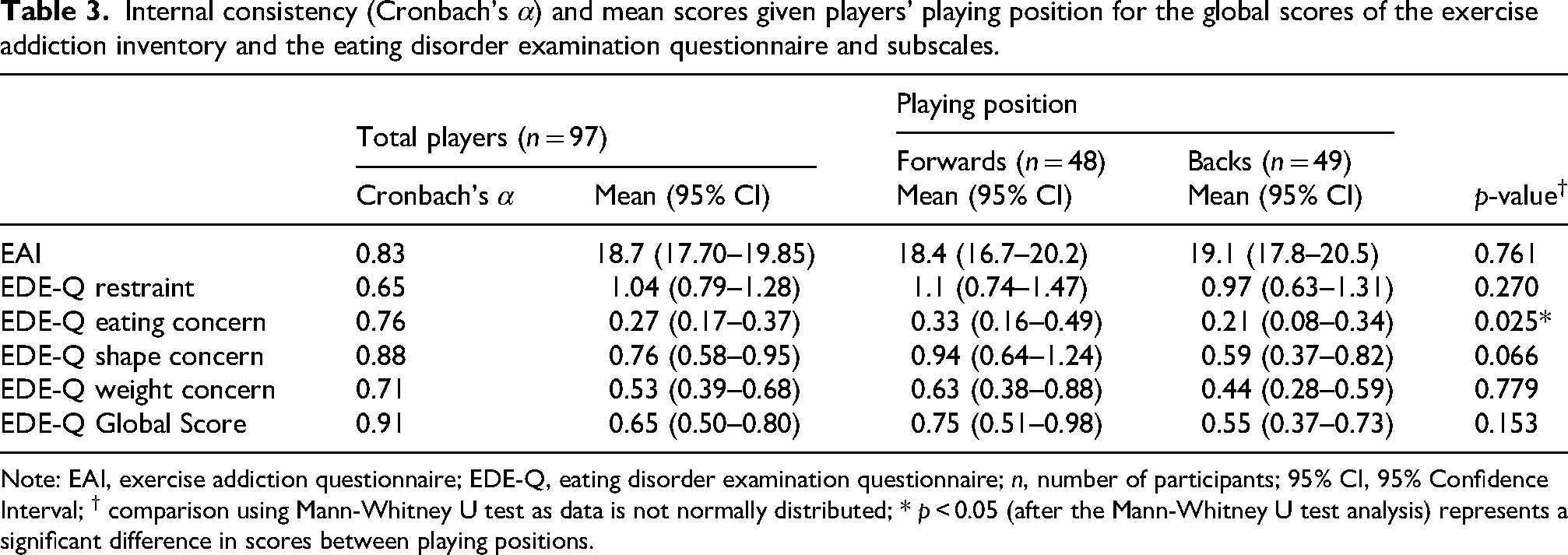
Note: EAI, exercise addiction questionnaire; EDE-Q, eating disorder examination questionnaire; n, number of participants; 95% CI, 95% Confidence Interval; † comparison using Mann-Whitney U test as data is not normally distributed; * p < 0.05 (after the Mann-Whitney U test analysis) represents a significant difference in scores between playing positions.
Eating disorder risk
Overall, 9.3% of participants were classified as at risk of developing an eating disorder based on a global EDE-Q score ≥1.68. No significant association was found between eating disorder risk and a players’ professional status (p = 0.143), positional category (p = 0.702), body mass (p = 0.228) or age (p = 0.559). However, forwards, regardless of professional status, demonstrated significantly higher scores on the eating concern subscale than the back subscale (p = 0.03; Table 3).
Exercise compulsion
Exercise compulsion behaviour was reported by 16.5% of participants. No significant associations were found between exercise compulsion (EAI score ≥24) and positional category (p = 0.761), professional status (p = 0.456), body mass (p = 0.543), or age (p = 0.889).
Sex drive
Low sex drive was reported by 20.6% of participants, with no significant associations found with professional status (p = 0.589), positional category (p = 0.341), body mass (p = 0.340), or age (p = 0.763). Only 5% of participants demonstrated concurrent risk across domains, whereby 4% (professional) and 1% (non-professional) met thresholds for both low sex drive and either eating disorder risk (3% professional, 1% non-professional) or exercise compulsion (2% professional, 1% non-professional) (Fig. 2).
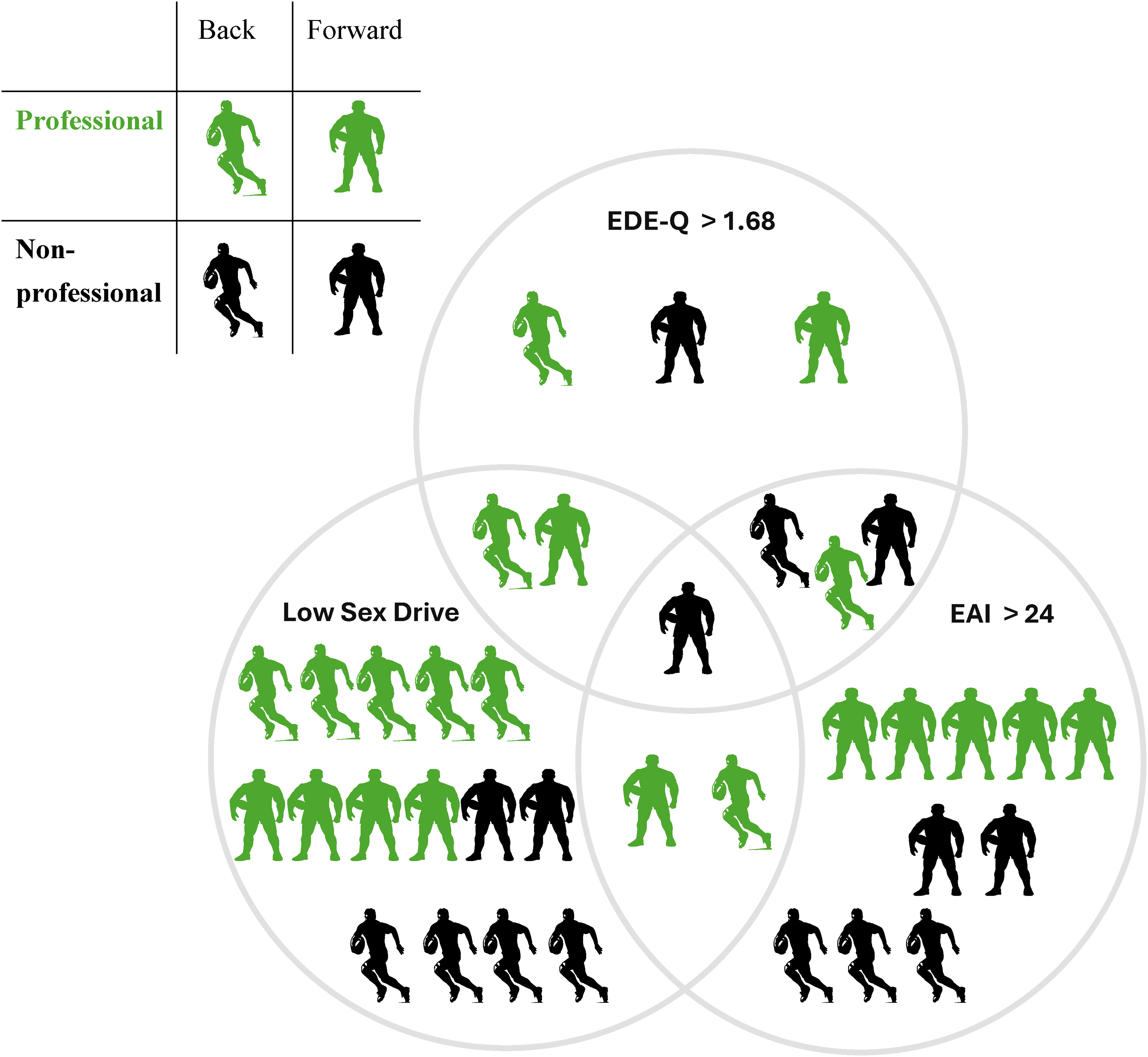
Prevalence and coexistence of eating disorder risk, low sex drive, and compulsive exercise in professional (green) and non-professional (black) elite male rugby union players. Note: Icons indicate players’ back and forward rugby positions. Of all participants (n = 97), nine scored ≥1.68 on the eating disorder examination questionnaire (EDE-Q 6.0), 20 reported low sex drive by scoring 2 or more on the sex drive section of the low energy availability in males’ questionnaire (LEAM-Q), and 16 scored ≥24 on the Exercise Addiction Inventory (EAI), indicating the risk of exercise compulsion.
Nutrition support
All participants reported attending at least one nutrition education session during their careers, and 99% indicated having access to a sports nutritionist within their training environment. Despite this high level of access, 9% (2% professional; 7% non-professional) stated they had never engaged with their sports nutritionists. A total of 60% (45% professional; 15% non-professional) reported having more than three one-to-one consultations, whereas 30% (5% professional; 25% non-professional) had between one and three consultations.
Energy monitoring practices
A total of 68% of participants (36% professional; 32% non-professional) reported having measured their dietary energy intake at least once. The most commonly used method was a mobile phone application (60%), followed by working directly with a nutritionist (6%) and using food labels (3%). The reasons provided by the participants for measuring their dietary intake are shown in Figure 3.
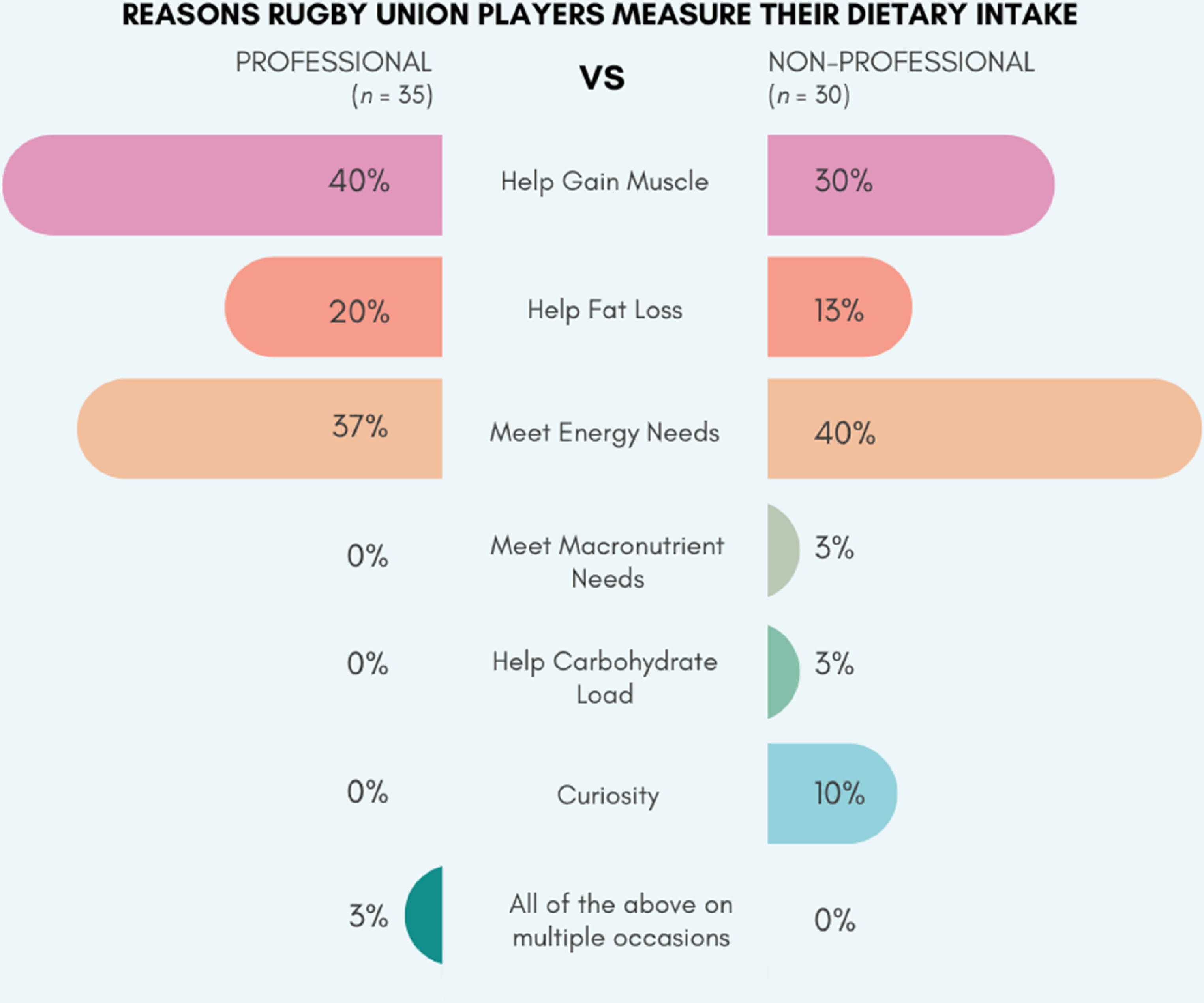
Reported reasons why elite male rugby union players in Ireland have measured their dietary intake.
Discussion
The primary aims of this study were to 1) explore the prevalence of elite male rugby union players who are at risk for eating disorders, low sex drive status, and exercise compulsion, and 2) explore the relationship between risk and players’ professional status, weight, or playing position. Risk prevalence was reported among players with eating disorders (9.3%), low sex drive (20.6%), and exercise compulsion (16.5%). Notably, forwards, irrespective of professional status, reported significantly higher eating concern scores on the EDE-Q subscale than the backs. However, no significant difference between professional status or position was identified when determining sex drive status or exercise compulsion.
A secondary aim was to explore the nutritional service support and dietary monitoring practices experienced by the players. Access to a nutritionist was reported by 99% of players, of whom 60% received more than three 1-1 consultations. Only 9% reported never engaging with a nutritionist. Dietary monitoring practices were reported by 68% of players, with the use of mobile phone applications most commonly used to support energy intake estimations.
To our knowledge, this is the first study to examine the co-occurrence and prevalence of eating disorder risk, low sex drive status, and exercise compulsion while simultaneously exploring contextual considerations of the nutrition service support available and dietary monitoring practices of a cohort of elite male rugby union players.
Eating disorder risk
The 9.3% prevalence rate of eating disorder symptoms reported in this study is lower than previously documented for elite (30%) 28 and professional (23%) 29 male rugby union players. Importantly, those studies utilised different screening tools, including the Eating Disorder Inventory (EDI) and the Eating Disorder Screen for Primary Care, rather than the EDE-Q. Similar, the Brief Eating Disorder in Athletes Questionnaire (BEDA-Q) also has reported a similar higher figure of 36% for symptoms of disordered eating among elite rugby players. 30 Comparing to studies that have utilising the EDE-Q, our findings were similar to elite collegiate rugby players (8.9%), 16 young academy rugby players (14%) 31 and to elite male student athletes (9.3%). 32 Our findings of higher levels of eating concerns in forwards versus backs is also consistent with Compte et al., 16 who reported a significant association between playing position and elevated eating concern pathology. However, caution is warranted when comparing prevalence rates across studies due to the differences in contextual factors, including the professionalism of the training environment, the level of nutrition service support, and the thresholds used to define clinical risk (e.g., the EDE-Q global score cut-offs of 2.3 in previous research versus the 1.68 used in the current study). It is well established that eating disorder risk is generally higher in weight category sports (22% in males, 42% in females) than in team ball sports (5% in males, 22% in females) 33 with elite athletes reported to have an elevated risk for disordered eating behaviours compared to non-athlete controls. 34 The variation in rates is frequently attributed to established sport-specific physique ideals and expectations, most often seen in weight-sensitive sports.2,6,35,36 While rugby union is not a weight-classified sport, the physique ideals of the sporting positions can still influence athlete behaviours, particularly among forwards, who often face pressure to attain and maintain specific body compositions. The current study contrasts with findings of broader sporting samples, where a greater risk prevalence (up to 32%) of disordered eating behaviour is present among elite athletes compared to non-elite athlete cohorts.33,37
Previous research suggests that limited nutritional knowledge, lack of access to professional support, or reliance on self-directed tools, such as fitness applications may contribute to the development of disordered eating behaviours.38,39 However, the influence of contextual factors such as access to performance nutritionist services is often unexplored. The reported overall EDE-Q score in this study is low for an elite athletic cohort, and may be attributed to the level of professional nutritional support reported available to the participants. The current study found 99% of players had access to a full-time performance nutritionist, with 60% having attended at least three 1-1 consultations.
Although the association between nutrition knowledge and disordered eating symptoms appears weak, 40 it is plausible that access to and the application of behavioral science theories by performance nutritionists to address athlete dietary adherence in high performance settings (as opposed to focusing solely on knowledge exchange) may play a meaningful role in mitigating the risk of eating disorders. 41 Contextual insights collected regarding nutrition service support and the main motivators for measuring energy intake in this study, combined with reported EDE-Q eating concern rates among forwards, shed light on resource considerations to mitigate eating disorder risk in professional rugby union pathways.
Sex drive
The current study reported prevalence rates of 20.6% for symptoms of low sex drive among elite male rugby union players; however, no associations were found with risk of eating disorders or exercise compulsion. Reduced libido and frequency of morning erections are recognized indicators of LEA, 18 which is a known precursor to the development of the male athlete triad. This condition may result in suppression of the hypothalamic-pituitary-gonadal axis.42,43 Athletes experiencing suppression of the hypothalamic-pituitary-gonadal axis may enter a chronically suppressed hormonal state referred to as the exercise hypogonadal male condition, where symptoms such as reduced sex drive are commonly observed.44,45 The prevalence rates of low sex drive status in the current study align closely with previous findings, such as the 23% self-reported prevalence of symptoms consistent with the exercise hypogonadal male condition across both individual and team sports athletes, identified using the androgen deficiency in aging males questionnaire. 46
Consistent self-reported symptoms of low libido in males have been associated with LEA risk,45–47 but the majority of evidence to date investigating sex drive status and libido is among athletes engaged in aesthetic, endurance, or weight-sensitive sports, with limited investigation among team-based athletes. 48 The sex drive section of the LEAM-Q has been identified as the most indicative self-reported method for determining whether a male athlete may benefit from additional clinical evaluations for low energy availability. 23 However, confounding factors such as fatigue, psychological stress (e.g., performance expectations/life stress), over-training, and medication use that may impact symptoms of low sex drive, as well as the intersection of common mental health disorders (anxiety and depression) associated with LEA symptomology should be considered. 6 These factors, which were not considered within the scope of the current study, may be a reason why so few participants with symptoms of low sex drive did not indicate a risk of eating disorders or exercise compulsion (Fig. 2).
Compulsive exercise
A risk of compulsive exercise behaviour was identified in 16.5% of participants, aligning closely with reported prevalence rates of 18.5% among elite male athletes across endurance, ball, and power sports. 49 Compulsive exercise, interchangeably referred to as exercise addiction, may arise independently of disordered eating behaviours. 50 The current study reports similar results, as no association was found between participants at risk of compulsive exercise and those scoring above the cut-off for eating disorder risk. This suggests that primary exercise dependency is possible among elite rugby union players, similar to other elite athletic cohorts, 51 and the absence of disordered eating behaviour may not mitigate the risk of compulsive exercise.
Additionally, masculinity and idealised physique expectations within elite rugby union environments may impact exercise and eating behavior. Physique ideals and expectations in sports are known mediators of body image concerns that can drive changes in eating behaviours, exercise compulsion, and EA status in athletes.2,6,35,36 Although investigations are limited among elite rugby union players, the presence of body image and physique concerns has been indicated, with 27% of male players reporting body dissatisfaction. 28 In the context of male rugby union, the risk of primary exercise dependency among elite rugby union players may be driven by sporting factors such as the positional physique requirements of the game, age, socio-cultural pressure to obtain professional status, or the psychological mediators of body image concerns. However, further research is required to understand the intersection between these factors.
Monitoring concurrent risk
Assessing the concurrent risk of eating disorder symptoms, low sex drive, and exercise compulsion is crucial for identifying athletes who are most vulnerable to health complications. Although not the objective of this study, applying the available IOC REDs CAT2 stratification would flag only 1% of participants at risk for all three indicators, indicating this method may serve as a starting point rather than a comprehensive solution. We propose that this very low-risk percentage may be due to the high accessibility of sports nutritionists within this cohort. To ensure early identification of those requiring support, practitioners could integrate screening tools that include contextual questions appropriate to their cohort of interest, similar to those used in this study, such as combining examinations of eating concerns with dietary monitoring experiences and physique goals. This approach prevents overlooked cases that may not be flagged through the IOC REDs CAT2 stratification system, but identifies those who may present with a significant health risk at a vulnerable time in their career.
Strengths, limitations, and future research
A key strength of this study is our reach of all available elite male rugby union players across four professional clubs in Ireland, providing valuable insight into this specific national population. The inclusion of validated screening tools, combined with contextual data on nutrition service access and dietary practices, offers a multidimensional perspective on the risk factors for eating disorders, low sex drive, and compulsive exercise in elite male rugby union. These findings offer applied value for interdisciplinary support teams working in similar high-performance settings.
This study had several limitations. Although the sample is one-third of an entire national cohort, generalisability to other countries, levels of competition, or cultural environments is limited. As a cross-sectional survey based on self-reported data, the findings may be influenced by response bias or underreporting owing to the sensitive nature of the topics. Cross-sectional data, reflective of a single snapshot in time, limits causal inference and therefore findings highlight the need for longitudinal studies to track how risk factors evolve over time. The study was also conducted during a potentially high-stress period where university exams and selection pressure for international competitions may have acutely influenced factors such as mood, anxiety, sleep, and libido. Additionally, the study did not account for confounding factors such as mental health conditions, medication use, or training load, which may have influenced the symptoms assessed.
Future research should adopt mixed methods or longitudinal designs to explore how psychosocial and physiological risk factors interact over time in elite rugby unions. Qualitative investigations are particularly warranted to uncover the lived experiences of players and to better understand the influence of cultural, positional, and career-stage pressures on health behaviours. Interviews with elite rugby union players investigating their experiences of disordered eating behavior and symptoms of low sex drive, may help add meaning to the findings of non-significant relationships found in this study between these LEA proxy indicators. Further, examining how interdisciplinary teams in professional rugby screen for and manage eating disorders, low sex drive and related conditions such as LEA could support the development of more targeted prevention and intervention strategies.
Practical implications
Given that over 45% of elite rugby players report a lack of access to specific psychological support measures, routine screening for both low sex drive and common mental health concerns is recommended. 52 While self-reported tools may serve as valuable indicators for further assessment, using sex drive alone as a proxy for low energy availability may lead to false positives if broader physiological and psychological factors are not considered. 53 Emphasising the gap in education and awareness of REDs among coaches and athletes, 54 we propose that rugby union organisations should incorporate player and staff awareness of eating disorders, low sex drive, exercise compulsion, and their interconnection with problematic low energy availability and REDs to mitigate risk prevalence. Additionally, a systematic interdisciplinary approach with best practice guidelines should be implemented in training environments to identify and manage known moderating risk factors, notably, addressing the management of sociocultural norms around peer-pressured physique ideals and weight stigmatization associated with elite rugby union players attempting to attain professional status, particularly young aspiring forwards. The implementation of such an approach underpinned by education should be integrated into all elite male rugby union training environments, resourced and managed in an interdisciplinary approach by qualified health care professionals with specialized knowledge to ultimately support the players’ psychological and physiological health.
Conclusion
This study identified that the risks of eating disorders, low sex drive and exercise compulsion are prevalent among elite male rugby union players in Ireland. This cohort of players, at the group level in Ireland, is not at a pronounced risk of REDs. The self-reported prevalence rate of 9.3% for eating disorder risk, 20.6% for low sex drive, and 16.5% for exercise compulsion with non-significant relationships found between them, suggests that individual elite players may be susceptible to these issues in isolation. Raising risk awareness among staff and players should be encouraged within professional and non-professional environments, to ultimately support player health and wellbeing. Further research is needed to understand the moderating factors driving symptomology among players within the context of professional and non-professional rugby union environments.
Supplemental Material
sj-docx-1-spo-10.1177_17479541251412343 - Supplemental material for Exploring the prevalence of eating disorders, low sex drive, and exercise compulsion among professional and non-professional elite male Rugby union players
Supplemental material, sj-docx-1-spo-10.1177_17479541251412343 for Exploring the prevalence of eating disorders, low sex drive, and exercise compulsion among professional and non-professional elite male Rugby union players by Gary Sweeney, Siobhain McArdle, Danielle Logue, Nessan Costello and Kieran Collins in International Journal of Sports Science & Coaching
Footnotes
Acknowledgments
The authors would like to acknowledge and thank the Irish Rugby Football Union and the participating clubs for their support throughout this study.
Ethical declaration
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and approved by the Technological University Dublin Research Ethics Committee (REC 22-62).
Consent for participation and publish
Written (electronic) informed consent to participate and for aggregated, deidentified results to be published was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.