
Abstract
Relative Energy Deficiency in Sport (RED-S) is a complex syndrome that occurs as a result of prolonged Low Energy Availability (LEA) leading to health and performance impairments. However, whilst the coach plays an important role when working with athletes with RED-S, no research exists specifically exploring their role. Therefore, this study investigates the role of the coach from the athletes’ perspective within an ultrarunning context. Ultrarunners are at risk of LEA due to large training volumes and record high incidences of psychological and physiological conditions linked to RED-S, such as disordered eating and bone stress injuries. Two female ultrarunners who had experience with RED-S each participated in three semi-structured interviews. The findings highlight the multifaceted role of the coach which changes depending on the stage of the athletes’ RED-S Journey. Of primary importance was that the coach should be educated on RED-S in order to provide value throughout. Secondly, for effective recovery, the coach should embrace working with a multidisciplinary support team of experts. Thirdly, the coach should actively work on establishing strong relationships with the athlete and their support network. This will propagate trust and honest conversations, a key requirement for recovery from, and ongoing training post, RED-S.
Keywords
Introduction
Ultramarathons are running races longer than 42.2 km, with successful performances typically associated with athletes completing high training volumes.1,2 These training behaviours require a high exercise energy expenditure and will result in low energy availability (LEA) when nutritional intake is insufficient. 3 Such LEA increases risk factors for Relative Energy Deficiency in Sport (RED-S). RED-S is the result of insufficient caloric intake and/or excessive energy expenditure (EEE). 4 A large energy deficit caused by EEE or inadequate energy supply can result in a cascade of pathophysiological maladaptive reactions. 5 Negative health and performance outcomes associated with RED-S include impaired bone health, reduced training adaptation, and behavioural/mental-health implications 6 (Figure 1). RED-S shares underlying aetiology elements of both LEA and Overtraining Syndrome (OTS). 7 OTS can manifest after a period of high training load, negatively impacting the immune function and/or prolonged fatigue resulting in reduced performance. 8 These complex and intrinsically linked syndromes have many of the same symptoms and thus present challenges in diagnosis. 7 Although an International Olympic Committee (IOC) consensus statement on RED-S exists, 6 the condition lacks recognition by healthcare professionals9,10 and coaches. 11 There is a clinical assessment tool for RED-S, 12 however, with, at times, no clear delineation between LEA, OTS and RED-S, athletes, coaches, and healthcare professionals can struggle to correctly identify RED-S9–11.
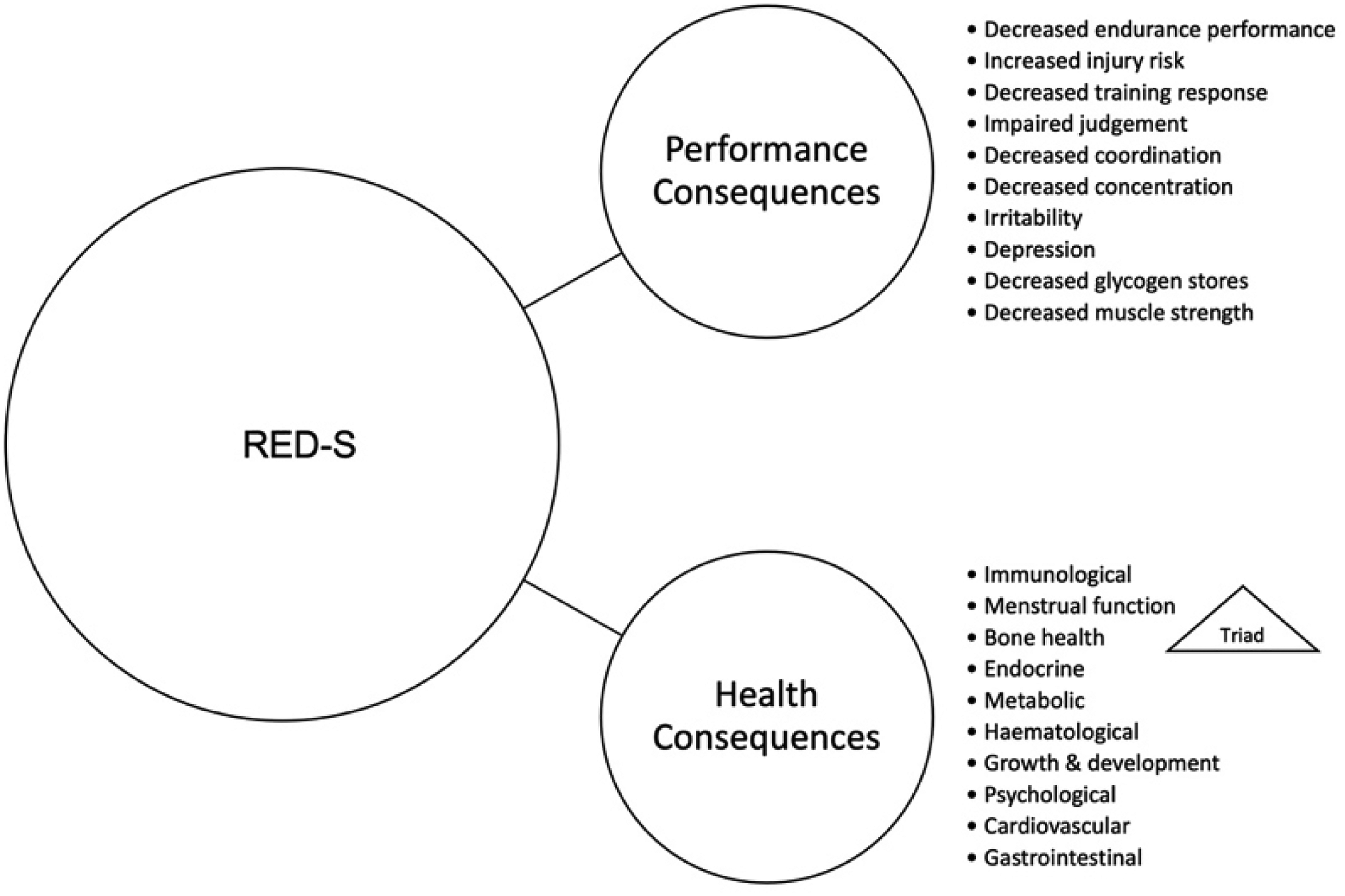
Performance and health consequences of RED-S (adapted from Mountjoy et al., 2018).
Identifying prevalence of RED-S is challenging, partly because RED-S is a poorly recognised condition by medical practitioners and coaches.9,11 Furthermore, little is known about the role of the coach when working with athletes who are at risk of or suffering from RED-S. Therefore, this study sought to explore ultra-running athletes’ experiences of RED-S and the runners’ perspectives on the coach's role when managing it.
RED-S prevalence and symptoms
There are several conditions with symptoms and aetiologies similar to, or overlapping with, RED-S, such as the LEA 3 or OTS. 7 In a study including national and world-class female endurance runners, prevalence of LEA was 28%, with LEA-likelihood increasing the greater the distances athletes ran. 13 Rogers et al., 14 identified that up to 80% of elite and pre-elite female athletes exhibited at least one symptom associated with RED-S, whilst over a third exhibited two or three symptoms. Three common symptoms of RED-S for female athletes are LEA, decreased bone mineral density, and menstrual dysfunction, collectively known as the Female Athlete Triad (FAT). 15 Whilst covering some of the potential outcomes of prolonged LEA, such as low bone mineral density, the FAT is not comprehensive enough as it does not include other symptoms that athletes experience. Therefore, the development of RED-S encapsulates the FAT, and highlights further associated physiological and psychological implications (Figure 1). 6
Risk factors for RED-S, such as LEA, bone stress injuries/low bone density, low BMI are prevalent in ultrarunners.7,16 In addition, these athletes have a higher risk of disordered eating. 17 Whilst the prevalence of RED-S in ultrarunners is not known, Folscher et al., 18 identified that 44% of the ultrarunners in their study were at risk of the FAT. Therefore, with the prevalence of the FAT in ultrarunning, and the intrinsic relationship (as per Figure 1) between the FAT and RED-S, it is important for coaches to learn about RED-S.
When RED-S is identified, the multifaceted nature of recovery from RED-S is equally challenging because psychological factors interact in complex ways with physiological ones. 19 Psychological consequences may include depression or irritability 6 and sufferers have discussed being on an emotional roller coaster. 20 Stellingwerff et al. 7 suggest a multi-disciplinary support network may be helpful to treat RED-S, however, they recognise that most athletes do not have access to such support. For example, treatment may not be readily available where there are diagnostic challenges, arbitrary clinical-thresholds, and other treatment barriers. 21 Many medical practitioners are inadequately equipped to support sport-related conditions and other support staff, such as physiotherapists, have been found to lack knowledge of RED-S and how to manage it. 22 Whilst it is important to increase the awareness amongst medical professionals, as they are often the primary professional for the athletes’ care, 23 binary approaches to diagnosing disordered behaviours are not overly helpful. 24 Rather, transdiagnostic approaches to address complex aetiologies are advocated, where suitably trained non-medical people help provide support when resources are limited. 24 Coaches are one such member of an athlete's support network. Coaches could, therefore, play a critical role in the prevention and treatment of RED-S as they are an important influence on athletes’ behaviours, particularly when working on an individual basis. 25
The coach and RED-S
In ultrarunning the coaching process includes prescribing healthy training loads and providing guidance relating to appropriate energy intake. Research, however, frequently focusses on the actions of coaches as a contributor to athletes’ poor mental and physical health 26 which may heighten the risk of RED-S. For example, negative personal rapport between the coach and athlete, has been shown to raise athletes’ anxiety levels. 27 Female athletes competing in individual sports with an unsupportive coaching environment used disengagement-orientated coping strategies (such as expressing unpleasant emotions) to deal with pressure. 28 Plateau et al. 29 found coaches promoted negative eating behaviours and excess training volumes in the belief that they are critical to performance. Heather et al. 30 identified that >10% of elite female athletes had been told by their coach that they needed to lose weight. In a study of female physique athletes (athletes judged on symmetrical appearance and low-fat mass, rather than physical performance), 31 the coach was identified as the greatest influence on dieting behaviour and bodyweight loss. 32 Multiple studies (e.g.,33,34) have demonstrated the potentially harmful power the coach holds in the coach-athlete relationship, and the pressure athletes can feel when trying to speak out on sensitive topics. Furthermore, athletes’ maladaptive eating approaches, including disordered eating, have been attributed to pressure from coaches, with the aim of manipulating body size or shape.35,36 In contrast, athletes who perceive themselves to be more compatible with their coach have been shown to experience fewer negative emotions. 37 Furthermore, athletes in individual, rather than team, sports have been shown to have a more committed and closer relationship to their coach. 38 These findings suggest that the relationship between the coach and athlete may be critical to ensuring there are opportunities for open discussion about how best to train and prepare for ultrarunning performances. In fact, a strong coach-athlete relationship has been shown to mitigate some of the perceived pressure on body weight related to the development or increase in severity of disordered eating. 39
This evidence suggests the actions of coaches can have a strong influence on athletes’ energy availability (EA) through influences on eating behaviour and training load. Energy intake and, importantly, EA is key for both avoiding and causing RED-S. Athletes report several challenges to achieving adequate EA. 40 This includes knowledge of and actual volume of food to be consumed, the financial impact of higher food consumption needs, and lack of time for food preparation and consumption. 40 Moreover, athletes have perceived coaches’ knowledge on nutrition and bodyweight to be insufficient, but advice from dieticians helps increase some athletes’ understanding on these topics. 41 It has been argued that coaches and athletes’ knowledge is socially constructed and influenced by their relationships42–44 with varying forms of knowledge influencing athletes’ awareness of nutrition differently. 41 Consequently, diverse experts, such as a coach or dietician, may impact athletes’ nutritional approaches in varying ways.
Distinguishing between intentional (disordered eating or eating disorders) versus un-intentional under-fuelling is important because those un-intentionally under-fuelling their training may not be aware of this discrepancy in EA and its consequences. 6 To support athletes, coaches (not athletes) are likely to initiate discussions around fuelling and performance. 40 However, a recent scoping review suggested that training for coaches on RED-S from National Governing Bodies 45 was not common, albeit considered paramount to support athletes’ health. Therefore, although there is evidence that education of coaches can help to identify eating disorders and lead to positive interventions for athletes’ health, 46 further research into athletes’ ‘lived’ experiences of RED-S is needed to develop a deeper understanding of the biopsychosocial elements linked to RED-S. 47 Moreover, it should include exploration into athletes’ recovery from RED-S20.
Therefore, the aim of this research was to explore athletes’ perspectives on the role of an ultrarunning coach in supporting ultrarunners with RED-S. Developing this understanding could establish the importance of the role of the coach in RED-S aetiology, prevention, and recovery and assist coaches to better support athletes’ performance, health, and wellbeing.
Methods and methodology
Participants
Potential participants were recruited via a post on social media. This sampling was deemed appropriate, as due to the difficulties with diagnosis of RED-S, it was important that participants self-identified as having lived with RED-S and were willing to discuss their experiences. Two female ultramarathon runners responded to the post and subsequently volunteered to participate in this study. Although a small sample, there was no limit set by the authors in terms of numbers or sex, but rather only two female ultrarunners responded to the advertisement within the timescales. This enabled the researchers to explore participants’ information-rich experience. 48
At the time of the research both participants were in their 40's, in the recovery phase of RED-S, and not racing, but had plans to continue with the sport once recovered. Whilst self-identified, initial screening revealed both participants were working with multiple experts on symptoms associated to RED-S, such as bone stress injuries, hormonal imbalance, nutritional intake, and menstrual cycle dysfunction.
Participant 1 had been competing in ultra-marathons for over 5 years and had won multiple major competitions and qualified for World Championships. She had been diagnosed with anorexia nervosa and had been an in-patient in a specialist treatment centre. This had coincided with a sudden loss in weight, in-part due to a stress fracture meaning training was not possible.
Participant 2 had been participating in ultrarunning for 2 years. She was participating for enjoyment rather than competing for wins and had come from a road running background.
Both participants had worked with coaches previously, with Participant 1 working with a new coach at the time of the research. The participants had extensive support networks including professionals such as endocrinologists, medical practitioners (for bone stress injuries), physical therapists, and dieticians. Participant 1 was also working with a psychiatrist.
Ethical approval was provided by the General University Ethics Panel of the host university. Participants gave informed consent prior to data collection. Due to the sensitive nature of interviews, the participants were assured that their identities would only be known to the first author. They could also review transcripts and subsequent draft manuscripts to ensure that they felt that interpretation was fair and that they could not be identified by the stories they told. Participant 2 accepted this offer and reviewed her transcript.
Procedure
Following institutional ethical approval, the advertisement was posted on social media, and participants were identified for the study. Dates and times for the interviews were arranged to fit with participants’ schedules. This resulted in interviews being conducted over a 5-week period. All interviews took place via MS Teams. Interviews lasted between 55 and 70 min and were transcribed verbatim.
Data collection
To enable in-depth exploration of the participants’ lived experience with RED-S, three semi-structured interviews were conducted with each participant. 49 This enabled sustained participants’ engagement in the study as well as providing time for preliminary analysis of the transcripts between interviews. In doing so, the researchers were able to reflect on the points raised and, in subsequent interviews, follow up on comments and explore additional areas. 49 It also allowed participants to reflect on the conversations. This approach resulted in both the interviewer and the participants referring to previous interviews and exploring topics in more detail.
Provisional topics for the interviews were developed through reviewing existing literature and, in recognition of the complex ‘interdisciplinary’ causation of RED-S, using the biopsychosocial model. 50 To encourage the participants to tell their story, the interviewer adopted the role of ‘active listener’. 51 Active listeners display empathy, understanding, and support the interviewee in sharing feelings and thoughts. 52 A reflexive process 53 was used to better understand how the participants’ experiences influenced their perceptions and understanding of RED-S, its impact on their training and broader life.
Data analysis
An abductive method of data analysis, generating theories from qualitative data, was used. 54 Abductive analysis facilitates exploration into the degree to which the data upheld existing theories (i.e., deduction), whilst also allowing the freedom to create new understandings or elucidations (i.e., induction). 55 This approach encouraged qualitative exploration of the complex syndrome of RED-S, its antecedents, and consequences. Through a process of indwelling, 56 the first author became familiar with the content, listening to the audio whilst cross-checking the transcripts to ensure accuracy, followed by reading each transcript twice. Indwelling involves the interviewer conducting the research, and then removing themselves and reflecting on the investigation and findings. 56 After developing an understanding of each participant's experience, the transcripts were reviewed for appropriate quotes relating to the onset of RED-S to return to running, to produce initial codes. Grouping of similar codes was undertaken, creating sub-themes, and this approach was replicated to produce more substantive themes and ensuing predominant categories.
Trustworthiness
The themes and categories were reviewed by all authors to ensure accuracy and improve trustworthiness. Trustworthiness is a term describing the methods adopted to enhance the quality of qualitative research. 57 It relates to the level of credence in the methodologies used and research findings. 58 The first author is a coach with experience and expertise within ultrarunning. His perspective permeated into the research, influencing the questions asked, the data analysis59,60 and interpretation. Being immersed in ultrarunning, experience, understanding and perceptions created over time results in greater comprehension and discernment of the culture and causal mechanisms for the participants. In this scenario it is impossible to remove research biases.61,62
To improve the trustworthiness, and ensure key points made by the participants were not missed, the second and third author acted as a critical friend (providing critique, alternative perspectives and reducing the likelihood of bias in the research and analysis 63 ) throughout the analytic process, providing balance and facilitating greater reflexivity through appraisal and discussion. 64
Results
For both participants RED-S is an ongoing journey, from the onset of RED-S to the Lived Experience, and Recovery and Return to Play. Within each of these categories, there are themes that are consistent across both participants and their perceptions of the role of the coach. The findings highlight the complexity of RED-S, with the role of the coach, in the eyes of the athlete, changing throughout the journey. The coach is at times seen as an ally, able to assist where appropriate, but the participants had also experienced negative influences from coaches.
The onset of RED-S
The consistent themes identified influencing the onset of RED-S were psychological drivers, educational influence, sport-specific pressures, physiological drivers and social environment (see Table 1). Participant 1 reflected on a perceived need for control, social approval and restrictive eating practices: “I would say that I have always been controlling, and sometimes restricting for that matter, my eating since my teenage years. I was always worried about my appearance, thinking I am not in shape, looking too fat.” Participant 2, however, experienced LEA due to unintentional under-fuelling and being unaware of the risks: “I was trying to achieve the same level of performance and gain I had on that nutritional pattern, and I didn’t understand that that wasn’t sustainable.” There were differences in the onset of RED-S, with Participant 1 having been clinically diagnosed with a pre-existing eating disorder whilst Participant 2 was unintentionally under fuelling.
Categories, themes and sub-themes linked to the onset of RED-S.
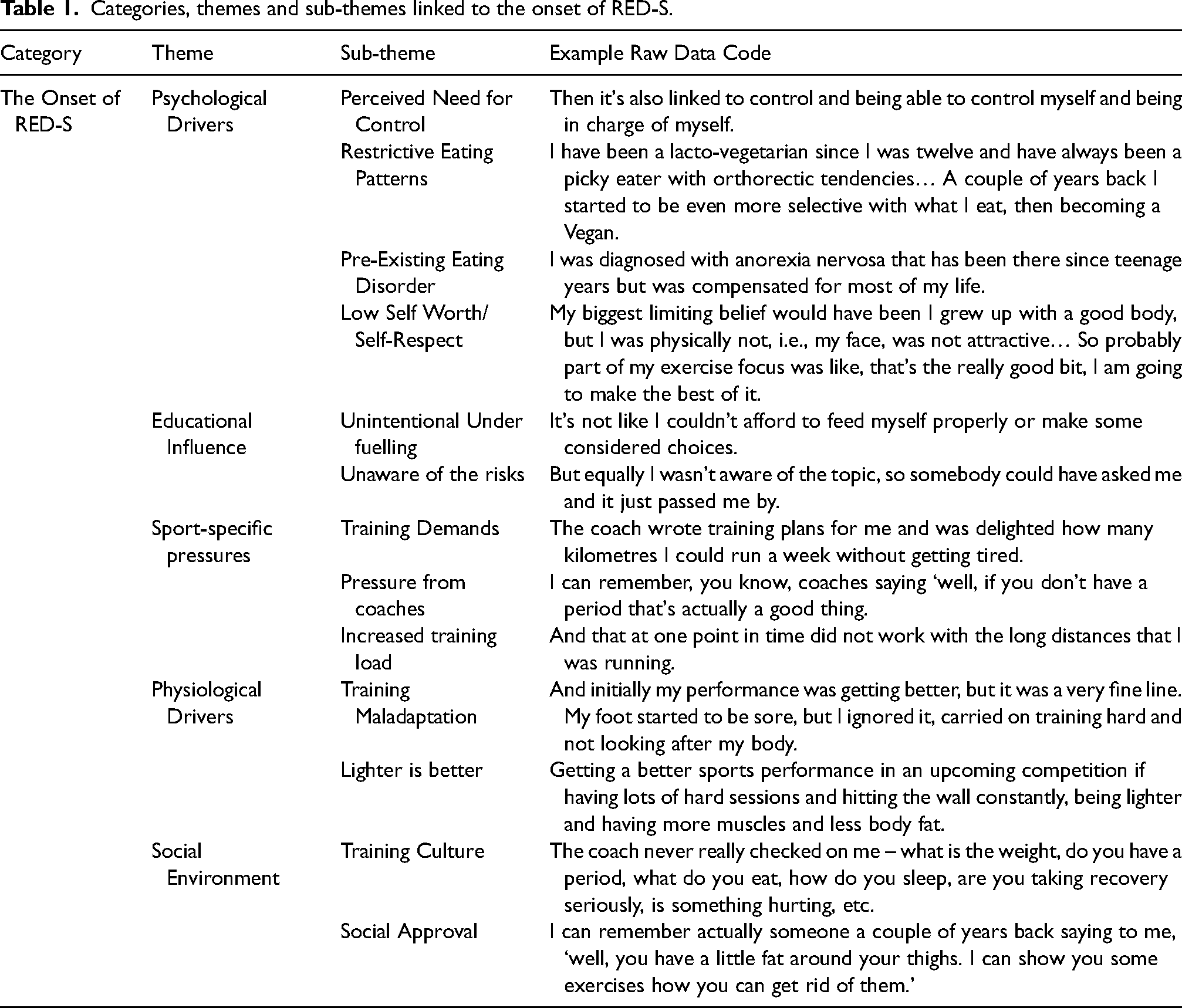
Both participants discussed low self-worth/self-respect. Their beliefs were not linked to sporting performance, but to appearance and a fear of ‘being fat’. However, the impact of training and the surrounding environment was prevalent, with training culture along with the training demands, and a mindset that being lighter is better important to them. These beliefs were influenced by pressure from coaches.
“We would always kind of try to restrict eating to become lighter. And we were also encouraged by our coaches to do this to a certain degree… but no one was aware back then that this is RED-S.’ (P1)
Consequently, with an increased training load training maladaptation resulted in an acknowledgement that something was wrong. “I tried to up my training to sustain something I had achieved. But because I didn’t get the gains from it, I was like ‘well I must be eating too much’, but in actual fact I wasn’t fuelling my body enough” (P2). Initially, both participants were unaware of the risks or of RED-S, however, acknowledgement helped change this: “I think that when you understand something, that means you’re going to have a different relationship with it.” (P2).
The lived experience of RED-S
Living with RED-S comprised three themes: physiological impact, psychological impact and social impact (see Table 2).
Categories, themes and sub-themes linked to the lived experience of RED-S.
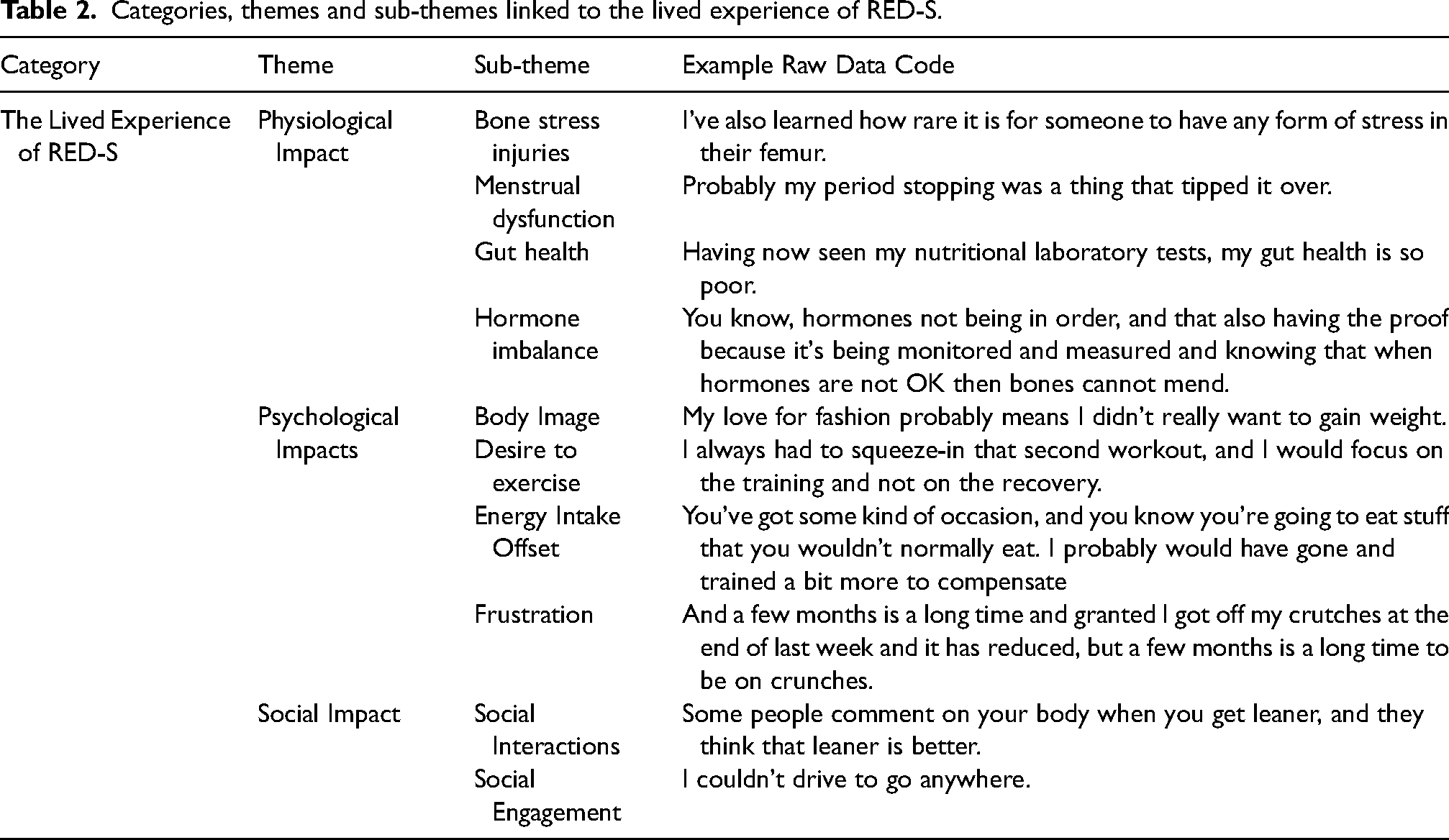
Both participants experienced bone stress injuries, menstrual dysfunction, gut health issues, and hormone imbalances. “The endocrinologist is helping a lot on this. They’re also kind of explaining the link between bone health, health, weight, and hormones.” (P1)
Furthermore, these symptoms, especially the injuries, led to frustration coupled with a desire to exercise; “I was still walking 10 km everyday to make sure I was ready to run a race. When in actual fact I had stress in my bone” (P2). “I was doing cycling and I was doing weight training and so on because no one really said ‘hey, this is the point where you need to stop and you need to gain weight.’ Only then, when the stress fracture did not mend, and we started to realise that there is more not OK than just a stress fracture and I needed to stop training” (P1).
Social interactions around appearance and weight and concerns over body image, and increasing weight linked to lower training volume, were frequently mentioned. Social interactions were sometimes uncomfortable as they could result in discussions around body weight and eating; “many people made remarks around, well, you know, - ‘I think you're a little thin, you should be eating more’” (P1). Participant 1 highlighted the interconnected nature of RED-S. “This disease is so complicated. Especially when, well, especially when you have an eating disorder that is underlying RED-S. There are so many different experts that help in different areas and only when putting all of that together it will actually become something that is useful and is helping me to address the eating disorder and RED-S.”
The RED-S recovery journey
The RED-S Recovery journey comprised six themes: education, training changes, support network, coach support, psychological adaptations, and challenges (see Table 3).
Categories, themes and sub-themes linked to the RED-S recovery journey.
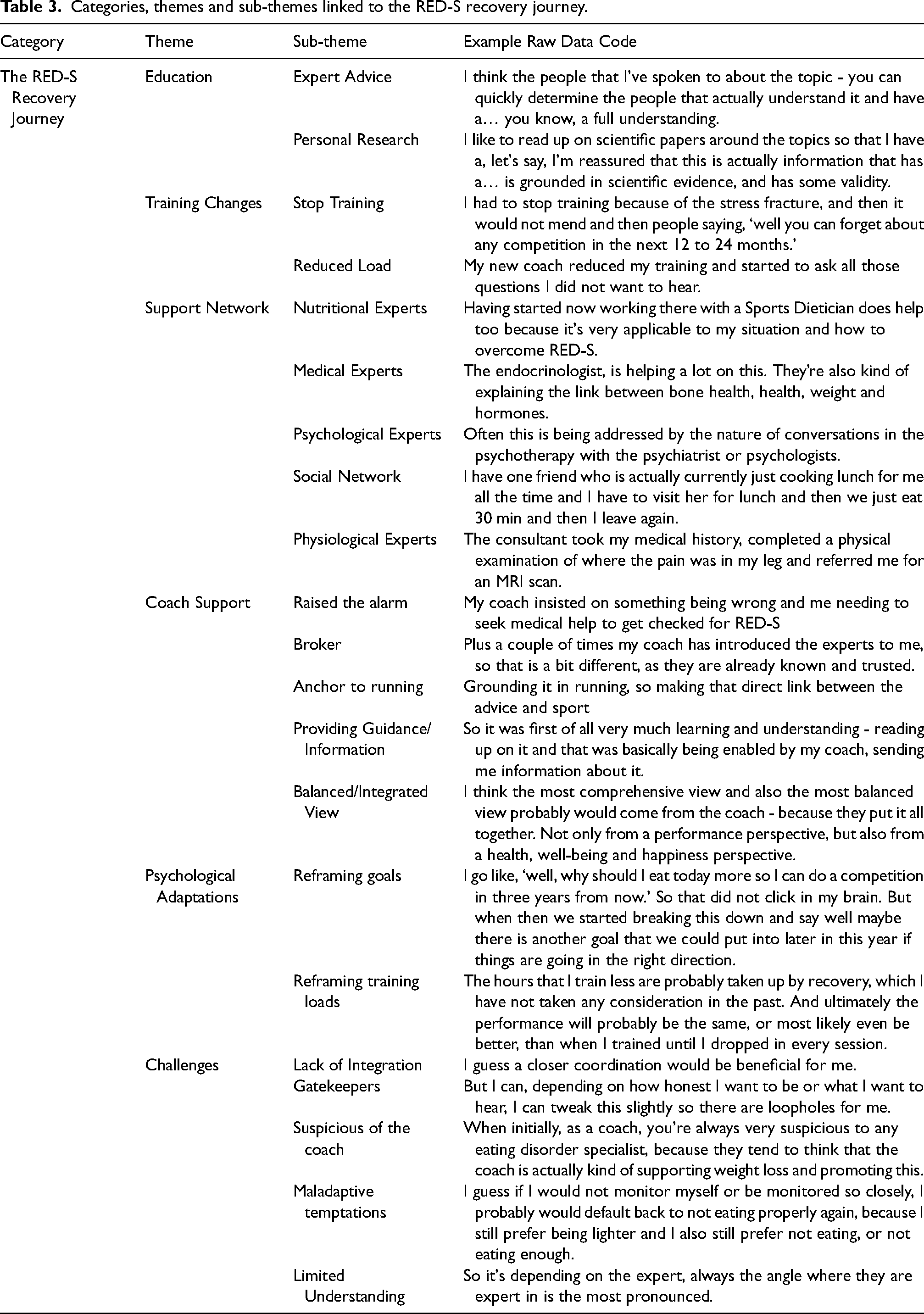
The participants relied on social networks, including friends, their coach and family. They augmented guidance from experts including nutritionists, medical practitioners, psychologists, and physiologists with research of their own. Coaches were sometimes encouraging and helped orchestrate guidance/information that was linked to ultrarunning or training. Participant knowledge changed the relationship they had with RED-S and was partly responsible for an initial stop to training before returning with a reduced load. Additionally, it resulted in nutritional changes that saw an increased energy intake, proactively fuelling workouts and optimising nutritional timing: “Understanding that if I do bring these three elements together, so training smarter, respect recovery and fuel well before, during and after training, then actually it does help with getting better training adaptation” (P1).
The recovery journey included adopting the expert advice of a reduced load and reframing training load. Doing so included understanding that previous volumes were unsustainable. Coupled with lower training volumes, reframing goals was important to their recovery strategies “acknowledging that there are different training sessions and different goals for each of the training session and not every session needs to be a very tough one” (P1).
Participants perceived that certain experts had limited understanding of RED-S: “I don’t think that many of them give a very comprehensive view, if at all” (P1). This resulted in participants orchestrating the support process themselves, making sense of differing advice and perspectives, which focused on treating the signs and symptoms of the individual pathology that related to the boundaries of practitioner expertise. Maladaptive temptations, such as “not eating properly” (P1), were present, especially when the participants felt the support network was not performing at a level they would have liked.
The role of the coach support was deemed crucial. For Participant 1, her coach “was adamant about something being very wrong with my health and my eating. He insisted that I seek medical help which I finally did.” A coach knowledgeable on RED-S was instrumental in providing guidance/information for both athletes “Because as a client you could also have absolutely no awareness at all of this thing called RED-S” (P2). At times they served as a broker, introducing the athletes to relevant experts, or resources; “My coach introduced me to the Sports Dietician and their team, that helped a lot as they talked to me about recovery and training” (P1). Furthermore, the support of the coach was successful when providing a balanced/integrated view that at times served as an anchor to running, by discussing support to and providing a link “back to running, always showing me the link between the intervention and the impact it will have on my running” (P1). However, participants suggested that experts could be suspicious of the coach and that they were a negative influence on body weight: “I always need to defend my coach a lot in front of the eating disorder specialist” (P1).
‘Return to play’
The themes identified influencing ‘Return to Play’ were successful support, coach's role, and independence (see Table 4).
Categories, themes and sub-themes linked to the ‘return to play’.
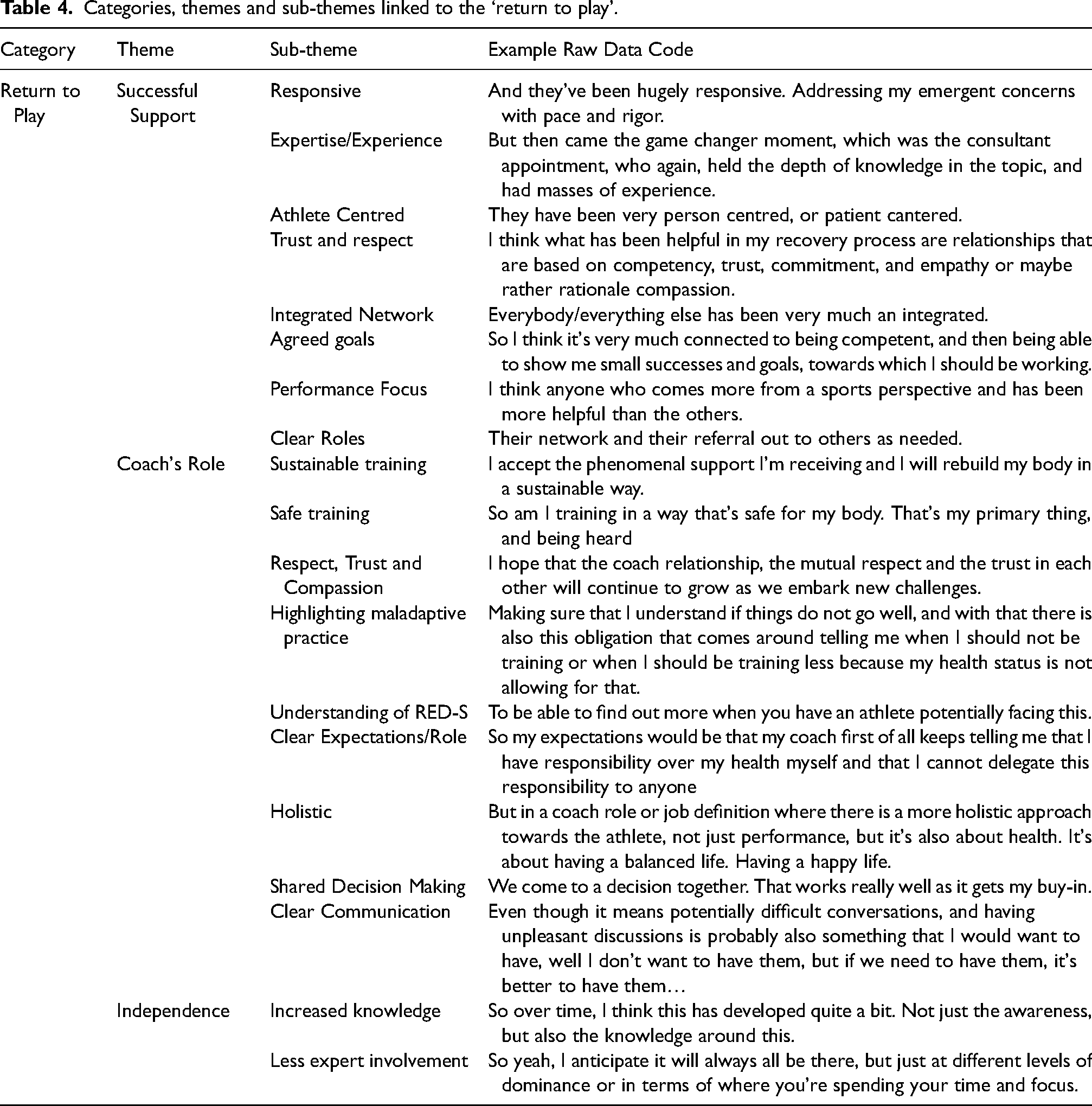
Participants valued support in which professionals were responsive and demonstrated broad expertise. Clear communication and knowledge helped develop trust and respect in relationships. Furthermore, participants valued practitioners who were athlete-centred and recognised the importance of performance – i.e., they spoke to the participant as an athlete, not as a patient: “I think anyone who comes more from a sports perspective has been more helpful than the others” (P1).
Moreover, there were agreed goals, the support network would work in partnership with the participants and were open to discussion: “Everybody has been very receptive to all my questions. All of my curiosity” (P2). Another key attribute for successful support centred on clear roles and integration between the experts as Participant 2 explained: “The experts will also direct me to the correct person to clarify something… Everyone respects their professional boundaries and their… limits in their knowledge and they welcome the input from the other specialists, which is really amazing.”
However, the participants recognised that there would be less expert involvement in the future, whilst acknowledging their desire to draw upon their support network when required. Participants recognised that their increased knowledge of RED-S and its symptoms gave them more autonomy: “You can do strength and conditioning, you can run, but it's finding a sustainable way to do that and that's I guess what I'm doing at the moment” (P2).
Participants believed that the coach-athlete relationship was central to the ‘return to play’. They recognised that coaches would support sustainable training, safe training and highlight maladaptive training practices when doing so. Through clear communication and clear expectations/role within the coach-athlete relationship, this would reduce the risk of the return of RED-S: “I guess what helps is if the coach is pointing out when kind of these wrong behaviours come into play and they're being very honest and blunt, right? Even though I get upset” (P1). Shared decision making was also a component that participants believed was beneficial and a key element of the coach's role. Through “discussing the options, removing any which I propose that the coach knows are non-beneficial and then discussing with me the alternative options” (P1) athlete buy-in is achieved for the decisions made. Participants recognised that coach education was important to help them understand RED-S and to develop the requisite skills to apply their knowledge: “the academic curriculum definitely needs, in my opinion, to equip coaches with the very basic knowledge and information that you need in order to have the awareness around RED-S” (P1).
Holistic coaching practice was also important in this regard: “I think it's a coach that can help ensure you're considering all aspects in a rounded way and treating your body as an integrated whole, which again is potentially easier said than done” (P2).
However, it was acknowledged by Participant 1 that, whilst a holistic approach is favoured, “unfortunately still a lot of coaches limit their coaching activities on just the performance aspect regardless of any health aspects or happiness aspects or mental aspects.”
Whilst clear expectations/roles were important to define, Participant 1 reflected on the ideal role for the coach, acknowledging this did not reflect her experience: “Ideally the coach can also help the athlete understand where this help can be found… basically being a bit of a broker of information… I don't think it should be the athlete's responsibility to link different experts and source this information back to the coach. But this is actually reality, because only as an athlete, or as a patient, you are seeing all these experts and you develop the first-hand relationship.”
Discussion
This study sought to provide insight into athletes’ personal and social experiences as ultrarunners with RED-S and their perspective on the role of the coach. The findings demonstrate greater prominence of the importance of their social network, including coaches, than is reflected in the literature (e.g., Mountjoy et al. 6 ), and that they are fundamental to manage complex aetiologies. 24
The participants’ RED-S experience
The participant narratives confirm that RED-S is a multi-faceted condition which is not susceptible to simple description or explanation. The challenges in definition, diagnosis of and delineation between similarly complex conditions such as LEA, OTS, and RED-S7,9,10 are likely to remain elusive unless there is greater recognition of the ontologies used to construct knowledge of complex aetiologies. The data in this study demonstrated that causality and treatment of RED-S emerges through complex biological, psychological, and social interactions. Thus, arbitrary diagnostic thresholds may not be best suited when working with ultrarunners with RED-S.
Participants discussed clinically diagnosable conditions including bone stress injuries, and menstrual cycle disfunction. 6 Additionally, exercise dependency, a separately diagnosable condition, 65 is often linked to RED-S and makes treatment more challenging. The participants struggled to cope with reduced training volumes, with stress negatively impacting recovery in athletes. 66 The participants also highlighted the impact of psychosocial elements including limited social engagement and comments on their appearance. For example, P1 failed to manage the cause of her stress fracture, by cycling and strength training to control her weight.
The role of the coach
The participants perceived the role of the coach as changing throughout the RED-S Journey and a key member of a support network. The findings highlight that multi-disciplined treatment teams are required, echoing the findings of Stellingwerff et al., 7 whilst revealing that the team must not demonise the coach, and embrace an integrated approach. Moreover, the coach, or other individuals within the treatment team, must help the athlete with introductions to relevant experts.
Coach education
The participants articulated that awareness and understanding of RED-S within their social networks, and with some of their previous coaches, was poor. This finding is consistent with the literature, which suggests increased awareness and education can help in the prevention of syndromes such as OTS and RED-S.6,45,67 The recommendations of Bar et al. 68 for more education on eating disorders are typical in this regard. However, researchers in many areas relating to sports performance and health will suggest that other people need to be educated in their disciplinary interest, without considering the pathways to deliver this education or coaches’ preferences for learning. However, ultrarunning is a relatively new sport, where limited traditional governing bodies exist to deliver education. Furthermore, coaches prefer to learn through experience and unmediated sources69,70 rather than formal pathways. Few ultrarunning coaches or athletes are in well-funded professional programmes with access to multi-disciplinary teams or have the skills to administer screening tools such as the Low Energy Availability in Females Questionnaire 71 or the RED-S Clinical Assessment Tool. 12
Solutions partly emerged when athletes worked to reframe training loads and goals with their coaches. Coaching beliefs surrounding training loads can be part of the cause of RED-S. Furthermore, the signs, symptoms and causes of RED-S are often shared with other syndromes such as OTS. Therefore, approaches to management of signs and symptoms will also be similar. Such approaches require a comprehensive understanding of appropriate training load, nutrition, menstrual function and what to do when things go wrong. Therefore, developing better coaching knowledge relating to the dose-response to training load may be salutary in terms of performance and health, and could be considered a transdiagnostic approach to multiple conditions.
Greater recognition that the coach will often orchestrate processes to prevent, manage and treat RED-S may be fundamental to successful outcomes in some cases. Notwithstanding, a previous coach of P1 believed that disrupted menstrual function was a positive thing. However, P1 felt the need to defend her subsequent coach when the practitioner providing treatment assumed that he was a negative influence on body mass. This was despite it being the coach that had suggested the athlete sought help. Both participants reported a lack of cohesion and communication within their support network, which was detrimental to their recovery. This suggests that medical professionals will often prescribe interventions without adequate appreciation of the role of the coach in tackling the causes of illness in sport. Co-creation of interventions between coaches, athletes and medical practitioners is advocated, in which learning is likely to emerge from collaboration. Furthermore, transdiagnostic approaches advocated by Patel et al. 24 may be better suited to the management of complex conditions where resources are low and specialist guidance is provided on an irregular basis.
Training loads and eating behaviours
There were different levels of intentionality in training-load management and fuelling behaviours between the participants. This finding was consistent with Bloodworth et al. 72 in elite gymnastics, who suggest that extreme training and eating behaviours may be desirable and functional to an athlete's performance. Thus, the capability to control or manipulate their disciplined eating practices can be viewed as a performance requirement rather than a pathology. Some athletes may be willing to compromise medium-to-long-term health for short-term performance. 73 If the pervading performance discourse relates to high-load and low-mass, then the coach and athlete may ignorantly conform to such customs, where compliance is based on partial or slanted information. 74 The panacea for both athletes in this study occurred when RED-S became non-functional, and they committed to treatment because of more physical manifestations of the syndrome. The participants highlighted a coach, and support in general, as more efficacious when linking support to running and performance. ‘Safe’ and ‘sustainable’ were two common terms used by the participants when discussing their return to running and ongoing training behaviours. This collaborative approach, with expert input from areas identified in Table 4, may enhance training, through embracing a holistic attitude linking to what is important.
The coach–athlete relationship
Bloodworth et al., 72 suggest that the level of autonomy athletes have in choosing their behaviours is key. The coach-athlete relationship is key to this autonomy, with the 4C's, Closeness, Commitment, Complementarity and Co-Orientation, of a successful Coach–Athlete relationship 75 highlighted throughout by both participants. Specifically, co-orientation involves agreeing on shared goals and effective communication, factors that both athletes agreed were important in their coach relationship and recovery process. Furthermore, respect, trust and compassion were highlighted by the participants as fundamental for the coach-athlete relationship. Jowett & Cockerill 76 suggest that, although a professional partnership exists, the presence of these feelings, on both sides, establishes the bonds required for generating a close environment. Through developing Closeness, the coach will be better placed to support their athletes through greater understanding, especially from a psychological and social perspective. Emotional health is also reflected in Complementarity through providing emotional support. 77 Both participants expressed frustrations and concerns around their clinically desired weight gain as these contradicted beliefs surrounding training volume and low body mass. The coach, through developing Complementarity within the relationship, can act as emotional support, helping further improve the relationship. This could help show the athlete the coach's Commitment to their recovery and return to the sport. Moreover, a strong coach–athlete relationship will allow for open and sometimes challenging conversations. The desire for high-volume training and hard-to-lose beliefs surrounding race weight, have potential for regression in behaviours that lead to maladaptation and the return of RED-S. 20 Coaches need to recognise the complex aetiology of RED-S where athletes may not always behave rationally or logically, potentially resulting in training behaviours which lead to maladaptation. Through the development of a strong relationship, and awareness of not just the physiological, but also socio-psychological elements, the coach can provide true value by promoting health and wellbeing in addition to performance.
Limitations and future directions
As with any research, there are limitations. Whilst this paper focussed on the athletes’ perspective of RED-S and the coach's role, the coach's perspective remains unexplored. Indeed, this appears to be a limitation of many original research pieces with one journal publishing over 1100 studies in sports and physiology, with less than 0.5% investigating the coach. 78 The small sample size of female ultrarunners may not be reflective of the experience of other athletes who have experienced or currently have RED-S. Therefore, future research should examine the lived experiences of other endurance athletes including male ultrarunners, as well as athletes competing in other sports. The first author's link to and knowledge of ultrarunning is likely to have influenced the interpretation of the data. However, although this may be viewed as a limitation, his ‘insider’ knowledge was also helpful in building rapport with participants and understanding of their experiences. Furthermore, the second and third authors input sought to reduce bias and the review of her transcript by one participant provided an opportunity to ensure fidelity in the interpretations of the data.
Based on both the limitations and the findings within the current study, several potential areas for further research are proposed. First, researchers exploring RED-S may benefit from involving coaches who have experience of working with athletes with RED-S as they are an untapped resource across sports studies. 78 Furthermore, with limited structured educational programmes for ultrarunning coaches, there is an opportunity to research how coaches learn about RED-S and how athletes construct their knowledge on nutrition and RED-S. 41 This may help inform more structured education programmes going forward. Secondly, quantitative and physiological research is dominant in the area of RED-S, and therefore further research investigating the socio-psychological elements of RED-S is required. 20 Adopting a mixed method approach may prove of value due to the complex integrated nature of the syndrome. There is limited application of this to date, but the work of Schofield 79 integrating quantitative research to explore the physiological impact and qualitative research for socio-psychological impact, provides evidence of the advantages of such an approach. Finally, although female ultrarunners were selected for the reasons previously given, male athletes are underrepresented67,80 and should be considered in future RED-S research.
Conclusion
For the first time, this investigation provides an insight into the role of a coach, from an athlete's perspective, when working with ultrarunners that have experienced RED-S. Illustrating this complex biopsychosocial condition, the current research underlines the critical role of a multidisciplinary framework of experts to assist athletes’ recovery and ‘return to play.’ Key to this coach support is appreciating the multifactorial, namely the biological, psychological, and social elements influencing the syndrome. The coach's role changes depending on where the athlete is on their RED-S journey, however, underpinning all stages is improving coach education to allow coaches to provide appropriate support.
Ultrarunners with RED-S are looking to return to training and racing without prolonging or re-encountering the negative impacts they have experienced. To facilitate this, the coach must develop strong relationships with the athletes and experts involved in their recovery from RED-S. Only by embracing the expert knowledge and incorporating it into the support, do they provide the appropriate level of help. The coach should ensure that this information is linked to running, making it meaningful for the athlete, whilst also involving the athlete in shared decision making, thus ensuring their buy-in. By incorporating the multiple sources of information, including the athlete, the value a coach can bring will be enhanced, and will benefit their recovery and ongoing post RED-S ultrarunning.
Supplemental Material
sj-docx-1-spo-10.1177_17479541231179301 - Supplemental material for Relative energy deficiency in sport and the role of ultrarunning coaches according to two female ultrarunners
Supplemental material, sj-docx-1-spo-10.1177_17479541231179301 for Relative energy deficiency in sport and the role of ultrarunning coaches according to two female ultrarunners by Douglas G Stewart, Justine B Allen and Andrew Kirkland in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-2-spo-10.1177_17479541231179301 - Supplemental material for Relative energy deficiency in sport and the role of ultrarunning coaches according to two female ultrarunners
Supplemental material, sj-docx-2-spo-10.1177_17479541231179301 for Relative energy deficiency in sport and the role of ultrarunning coaches according to two female ultrarunners by Douglas G Stewart, Justine B Allen and Andrew Kirkland in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-3-spo-10.1177_17479541231179301 - Supplemental material for Relative energy deficiency in sport and the role of ultrarunning coaches according to two female ultrarunners
Supplemental material, sj-docx-3-spo-10.1177_17479541231179301 for Relative energy deficiency in sport and the role of ultrarunning coaches according to two female ultrarunners by Douglas G Stewart, Justine B Allen and Andrew Kirkland in International Journal of Sports Science & Coaching
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.