
Abstract
Background/Objective
To assess athletes’ and coaches’ confidence in knowledge and recognition of Relative Energy Deficiency in Sport (REDs) before and after an education session at the Canadian University Sports (U SPORTS) National Cross-Country Championships (UXC).
Methods
We hosted an education session and panel discussion surrounding causes and risk factors, health and performance outcomes, prevention, as well as personal experiences the day before UXC. A cross-sectional in-person survey (39 pre- and 29 post-session questions) was implemented around the session. Sixty-eight athletes (85% ages 19–24y, 73.5% women) and 20 coaches (30% > 50y, 35% women) completed the survey.
Results
Pre-panel, 80% of coaches and 59% of athletes were able to correctly identify the underlying cause of REDs (low energy availability). However, only 50% of coaches and 13% of athletes were completely confident in their answers. The most common correctly identified symptoms were fatigue (coaches = 40%, athletes = 53%) and amenorrhoea (coaches = 30%, athletes = 57%). However, only 20% of coaches and 7% of athletes were completely confident in their answers. After the panel, confidence levels of coaches in identifying signs/symptoms did not change (p = 0.52; complete confidence = 20%), but significantly improved in athletes (p < 0.001; complete confidence = 32%). Low libido was a commonly identified learned symptom.
Conclusion
An education session and panel discussion surrounding REDs significantly increased the confidence in REDs knowledge among UXC athletes, but not among coaches. Further exploration of REDs knowledge dissemination strategies, that should be different for athletes versus coaches, is needed to improve awareness of REDs.
Introduction
Relative energy deficiency in sport (REDs) is a syndrome of impaired physiological and/or psychological functioning underpinned by exposure to problematic (prolonged or severe) low energy availability (LEA). 1 In contrast, adaptable LEA exposure to a reduction of energy availability that is associated with benign effects (mild, quickly reversible). 1 Athletes participating in aesthetic sports with subjective judging, weight class sports, and/or endurance sports (with high volumes and intensities) are at higher risk of developing problematic LEA from either intentional or unintentional decreased energy intake and/or increased energy expenditure. 1 Consequences of problematic LEA leading to REDs include menstrual dysfunction in females, decreased libido in males, poor bone health, metabolic and haematological issues, psychological disorders, cardiovascular impairments and gastrointestinal (GI) dysfunction. 1 Additionally, LEA can cause performance consequences, such as decreased training response, impaired judgement, decreased coordination, decreased athlete availability and decreased endurance performance. 1
Cross-country runners and other endurance athletes are at increased risk of developing REDs due to prolonged exercise bouts at high volumes and intensities, coupled with sport cultural/societal pressures that “lighter = faster”. 2 For example, one study demonstrated that the burden of bone stress injuries (BSIs) was highest in female National Collegiate Athletic Association (NCAA) cross-country athletes (64%) compared to other sports. 3 Similarly, another study reported a high prevalence of REDs signs and symptoms in NCAA Division I (DI) female cross-country runners, where 75% self-reported a BSI, 58% reported haematological issues, 54% reported GI concerns, 53% reported menstrual dysfunction and 34% reported cardiovascular consequences. 4
Primary prevention of REDs aims to reduce prevalence through education initiatives for the athlete entourage – athletes, coaches, parents, and healthcare professionals.2,5 Primary prevention strategies for athletes include education around identification of REDs symptoms, minimising LEA exposures and reducing behaviours resulting in LEA. 5 Despite increased knowledge of the short- and long-term effects of problematic LEA exposure, translation of education into sport is lagging, as knowledge about REDs and its potential implications for sport is low among athletes and coaches. 6 For example, in a cohort of NCAA female cross-country athletes, coaches and athletic trainers (ATs), the knowledge, confidence and educational impact scores of identifying, screening, treating and preventing REDs were lowest in the athletes and highest in ATs. 7 Subsequently, impact scores (composite score of knowledge and confidence) were higher in athletes with a related academic area of study, those who attended DI institutions, and those with a history of REDs diagnosis. 8 There is some emerging evidence surrounding educational interventions at improving knowledge in athletes. For instance, one study demonstrated that Female Athlete Triad knowledge increased in high school female athletes following a brief, 10-min Social Cognitive Theory-based video. 9 Additionally, another study in competitive male cyclists at risk for REDs demonstrated that an educational intervention and positive changes in nutrition and skeletal loading were associated with an increase in lumbar spine bone mineral density (BMD), whereas negative changes were associated with a significant decrease. 10 Most research conducted on the knowledge and education of athletes and coaches has been focused on the Female Athlete Triad. However, this model was updated in 2014 by the International Olympic Committee to represent the greater physiological/psychological outcomes associated with REDs that go beyond the three aspects of the Triad (menstrual dysfunction, low BMD and LEA) and to reflect that it can also affect males. 11
Therefore, it is important to understand confidence and knowledge levels of coaches and athletes separately, to truly understand the potential impact that education can have on the sport environment. It has been hypothesised that improving knowledge in identifying LEA signs/symptoms, risk factors and diagnosis in athletes and coaches might result in improved Female Athlete Triad and REDs prevention.5,12 However, a systematic review demonstrated that dietitian students (i.e. highly educated on the topic) have a high prevalence and risk of eating disorders (ED) due to their exposure to diet information. 13 Promoting healthy team environments may have a large impact on athlete well-being, health, and predisposition to REDs. Furthermore, it is important that the right type and scope of knowledge is delivered to impact behaviour in a meaningful way. Before implementing a long-term, primary prevention education programme, it is important to understand and establish sport-specific normative knowledge of REDs signs and symptoms in athletes and their entourages. Hosting educational sessions at national championships [e.g. U SPORTS (Canadian University National Championships) or NCAA Championships] may be one way to improve education for athletes and athlete entourages, as they are natural gathering of coaches, athletes, and support team members. The objectives of this acute cross-sectional and intervention study were 1) to assess the baseline knowledge, recognition, and confidence of the signs/symptoms and reporting of REDs in cross-country coaches and athletes, and subsequently; 2) to assess the change in the confidence of knowledge, recognition and reporting after an education session and panel discussion for REDs at the U SPORTS Cross Country Championships (UXC).
Methods
Participants
Potential participants were recruited at the education session and panel discussion held at the UXC on November 11th, 2023 in London, Ontario, Canada (the day prior to the race). A brief description of the study and information session was sent from the meet director to all participating teams three weeks prior to the UXC race and panel discussion, and a reminder was sent one week prior. To be eligible for this study, participants had to be a UXC varsity athlete [ranked Tier 3 (Highly Trained/National) or higher] 14 or a coach on a UXC team and present at the education session and panel discussion. Additionally, participants needed to be able to read and write in English and have access to a mobile device at the time of the panel discussion. Those who were not specifically varsity athletes or coaches (e.g. health care professionals, parents, high school athletes), or who did not attend the education session and panel discussion were not eligible. This study was approved by Western Health Sciences Research Board (HSREB #123749) and conformed to the standards set by the Declaration of Helsinki. All participants provided electronic informed consent prior to beginning the survey.
Education session & panel discussion
The education session and panel discussion were divided into two parts. The first part consisted of a 30-min education session for coaches and athletes in the same room, where two experts in the field (study co-authors TS & JST) gave a presentation on REDs recognition, risk factors, signs/symptoms, diagnosis, and management, specific to the sport of cross-country running. Furthermore, the authors used evidence from recent research and case examples to substantiate their claims. Following the education session, the athletes and coaches were split up into separate rooms to partake in an educational panel discussion (∼1.5 h) that was bespoke and geared to coaches or athletes separately. Each panel had four-to-five members; the athlete panel was comprised of a sport medicine physician, a registered dietitian, a physiotherapist all with research expertise in the field, and two nationally ranked athletes with lived experiences. The coaches panel was comprised of current coaches of club, national and international levels, a current U SPORT athlete, a former nationally ranked athlete with lived experience and a researcher in the area. The panel was interactive, with participants having the opportunity to submit questions anonymously before and throughout the discussion period or ask them directly to the panel in person. Furthermore, questions could be directed to an individual on the panel, or the panel as a whole. A moderator was present to organise and facilitate the discussion. The discussion was based around what the participants wanted to learn more about, therefore it ranged from personal experiences, case examples and education pieces surrounding the different areas of expertise that the panellists had.
Study design/survey development
A cross-sectional interventional study design was used to examine the knowledge and confidence related to REDs risk factors, signs/symptoms, diagnosis, and management. The English-only survey was adapted from a previous study that developed a survey to measure coaches’ knowledge about the Female Athlete Triad, 15 as well as a subsequent study that expanded upon the first survey by including specific questions related to REDs. 7 These studies determined that both surveys showed good content validity and reliability (intraclass correlation = 0.68, Cronbach α = 0.914). We expanded these surveys to include more questions related to experiences with REDs diagnosis and management, and confidence in these areas. We also added a post-panel aspect of the survey to determine if the education session was successful in improving knowledge and/or confidence. Our survey was developed and reviewed by experts in sport medicine and REDs; a sport medicine physician and endocrinologist, a sport physiotherapist, current/former UXC athletes and coaches, and researchers (e.g. physiologist, postdoctoral researcher). All co-authors were involved in survey development, and it was piloted by 10 external experts (the panellists from the education session, as well as graduate students in our laboratory). Changes to better address the objectives of the study were implemented and a final survey was developed after a few iterations.
The anonymized, self-report questionnaire consisted of three parts and 68 questions (39 questions on the pre-education session and panel discussion survey and 29 questions on the post-education session and panel discussion survey). The questions were quantitative, on a Likert scale (n = 22; rank confidence on a scale of 1–5 where 1 represents not at all confident and 5 represents complete confidence) or select all that apply (n = 8; e.g. select members of the REDs health care team), with some open-ended text boxes to capture participant rationale (n = 13). Part one of the questionnaire characterised the participants by their role on the team, age, gender, race, and athletic or coaching background. The second part asked participants about their knowledge of REDs, as well as experience with management of REDs, and whether participants felt there are any barriers to accessing care for REDs. Display logic was used to differentiate between coaches and athletes and in some instances, coaches and athletes received slightly modified wording for questions (therefore, they did not receive the full 68 questions each). For instance, athletes were asked about their comfort levels in telling coaches if they were exhibiting signs/symptoms of REDs, whereas coaches were asked about their comfort levels in developing modified training programmes for those who had early and severe signs/symptoms of REDs. However, most (n = 23) questions were similar between coaches and athletes. Coaches were asked additional questions surrounding resources and responsibility for removing an athlete from sport if they are exhibiting REDs signs/symptoms. Athletes were asked additional questions pertaining to their thoughts about the underlying cause of their REDs diagnosis. Upon conclusion of the panel, participants were asked to complete the third and final part of the questionnaire. This questionnaire section evaluated the effect of the education session and panel discussion by reassessing participants’ confidence in knowledge, recognition and reporting of REDs. For example, coaches were asked again to report on their comfort levels in developing a modified training programme, whereas athletes were asked again to report on their comfort levels in reporting signs/symptoms to their coaches. Finally, both were asked on their opinions on the session and potential implementation of REDs education at the U SPORTS level. The survey was distributed using Qualtrics (Qualtrics, Provo, UT; https://www.qualtrics.com). A copy of the full survey, as well as a table differentiating questions between coaches and athletes, can be found in the Supplemental Material.
Statistical analyses
Demographics, as well as knowledge, confidence and experiences with REDs, both pre- and post-education session and panel discussion were analyzed using percentages and descriptive statistics. To analyze the effect of the education session and panel discussion on changes in knowledge and confidence of REDs, a Wilcoxon signed-rank test was employed, as all data were non-parametric. Data analyses were conducted using Excel and R. 16
Results
Demographics
There were 60 coaches and 365 athletes registered (187 males and 178 females) to participate at the UXC, representing 35 Universities. Roughly 200 people attended the panel discussion / education session held the day before the race, however; not all were eligible for the study (e.g. parents, members of the healthcare team, high school athletes and coaches). Furthermore, not all Championships participants travelled to the race the day before competition began. A total of 153 participants accessed the survey, and 88 participants (20.7% of registrants and ∼44% of panel discussion/education session attendees) which was composed of 68 UXC athletes (85% ages 19–24y, 73.5% women) and 20 UXC coaches (30% > 50y, 35% women), consented to participate, and completed the survey (Table 1). The race divisions were separated by sex (i.e. males/females), and we further collected information regarding gender (men/women). All athletes that identified as men raced in the male division, whereas all athletes that identified as women raced in the female division.
Participant demographics.
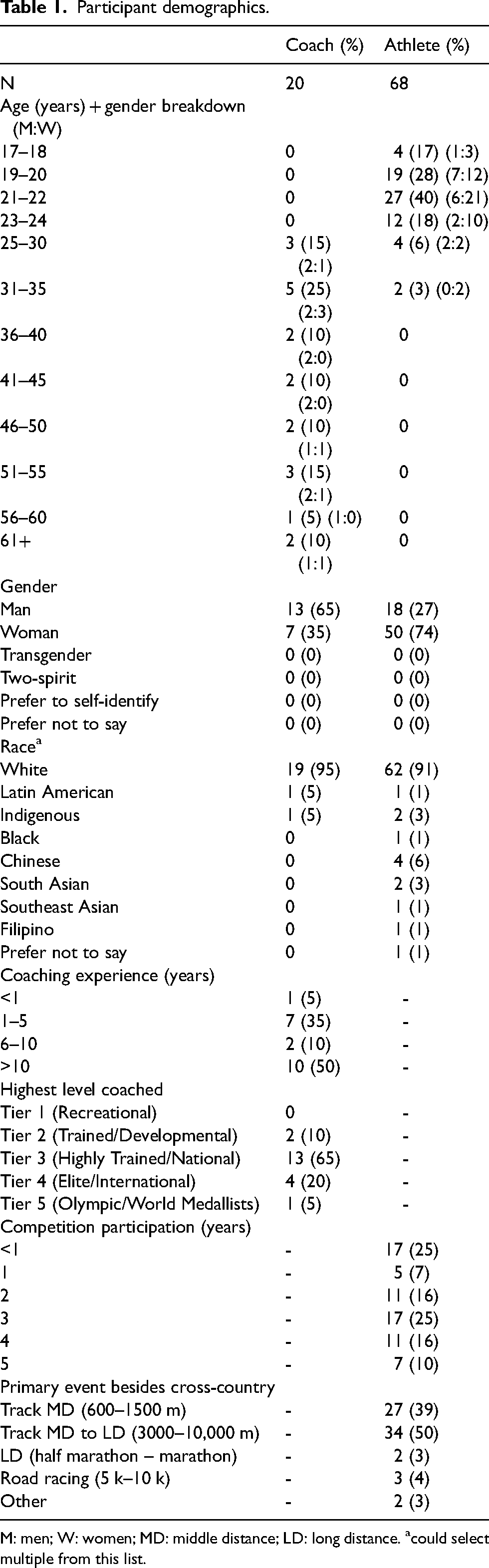
M: men; W: women; MD: middle distance; LD: long distance. acould select multiple from this list.
REDs knowledge
Pre-education session and panel discussion
When asked to identify the underlying cause of REDs (answer = LEA), 80% (n = 16) of coaches and 59% (n = 40) of athletes identified it correctly. However, when asked to rank their confidence in identifying the underlying cause (not at all confident to completely confident), 40% (n = 8) of coaches and 13% (n = 9) of athletes were completely confident in their answers (Table 2).
REDs knowledge.
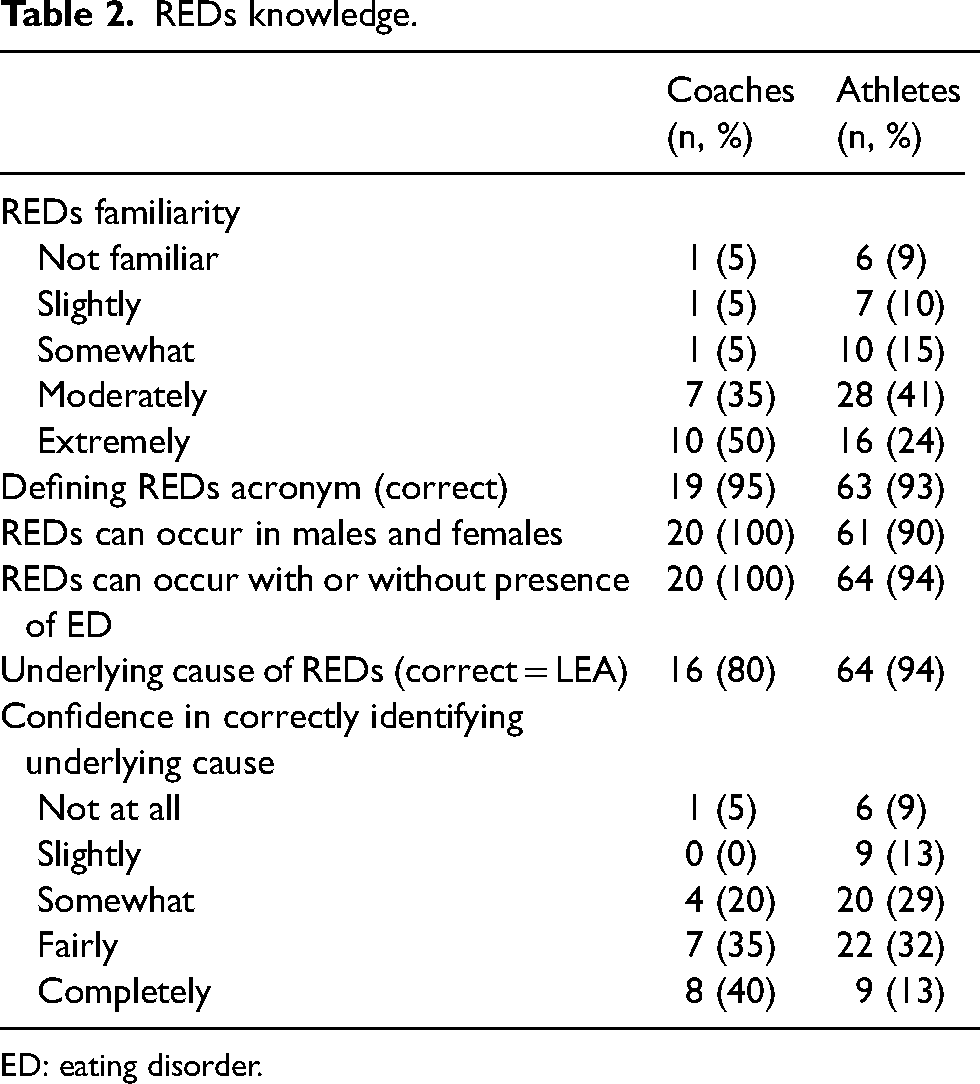
ED: eating disorder.
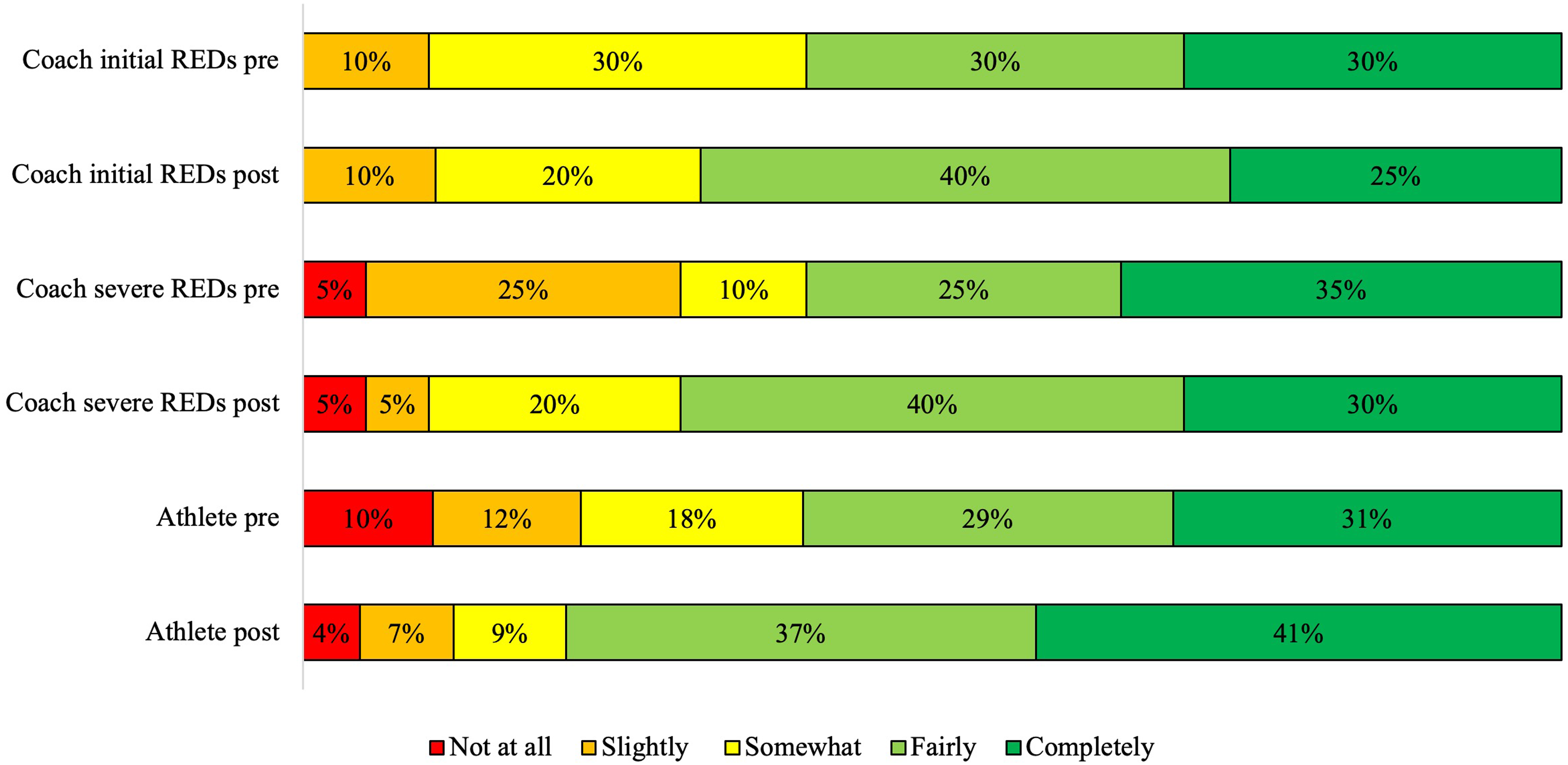
The most commonly identified signs/symptoms of REDs included performance/training decreases, injuries (including those bone-related), amenorrhoea, fatigue/tiredness, and low energy (Figure 1). When asked to rank their confidence in identifying signs/symptoms of REDs, 20% (n = 4) of coaches and 7% (n = 5) of athletes were completely confident in their answers, whereas no coaches and 4% of athletes (n = 3) were not at all confident (Figure 2).
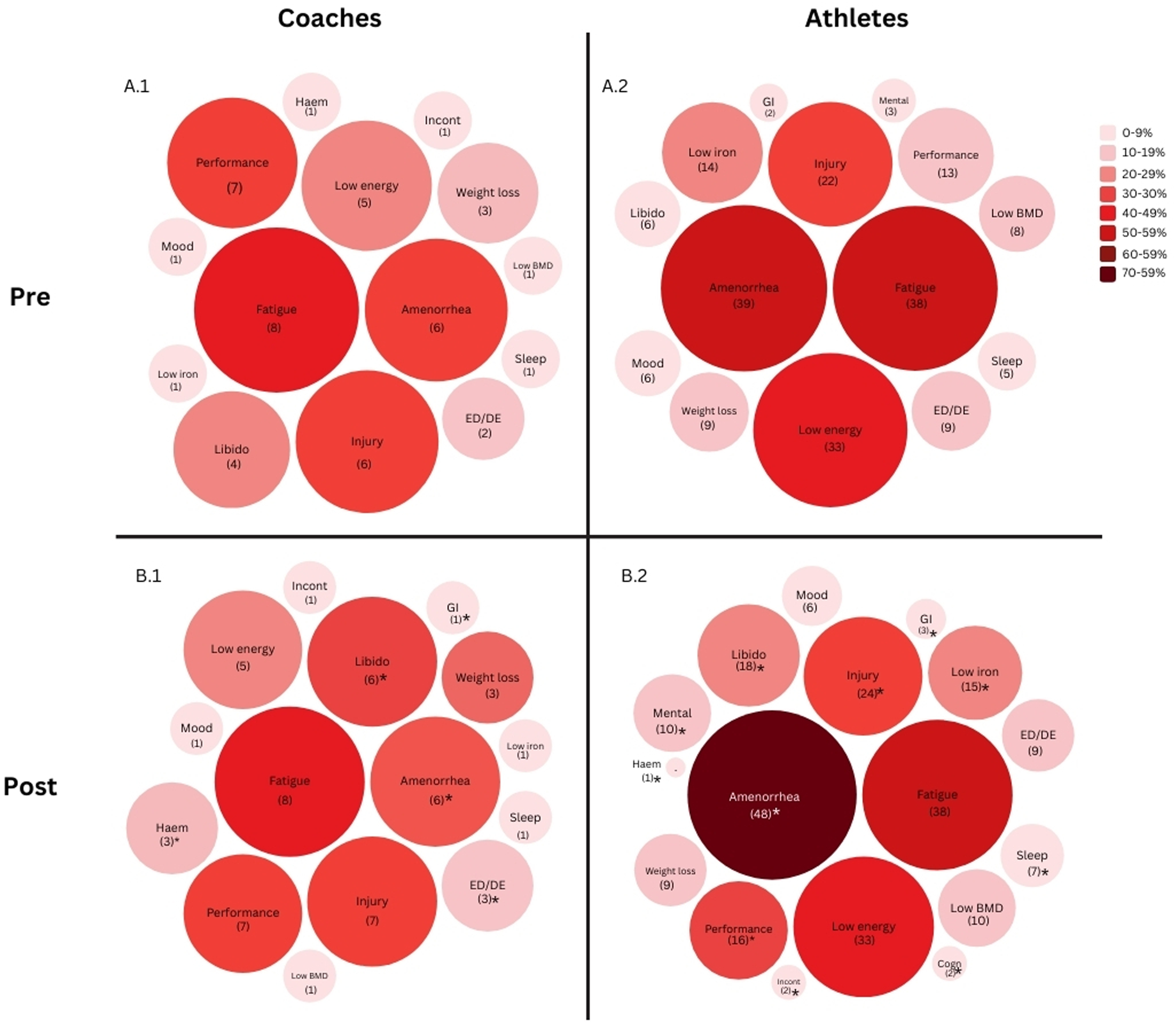
Pre-education session and panel discussion known (A) and post panel discussion learned (B; pre + new) signs/symptoms in coaches (1) and athletes (2). Number of respondents represented in brackets. *denotes changed from baseline known signs/symptoms. BMD: bone mineral density; ED: eating disorder; DE: disordered eating; Mental: mental health issues; GI: gastrointestinal; Haem: other haemotological impairments; Incont: incontinence; Cogn: cognitive impairments.
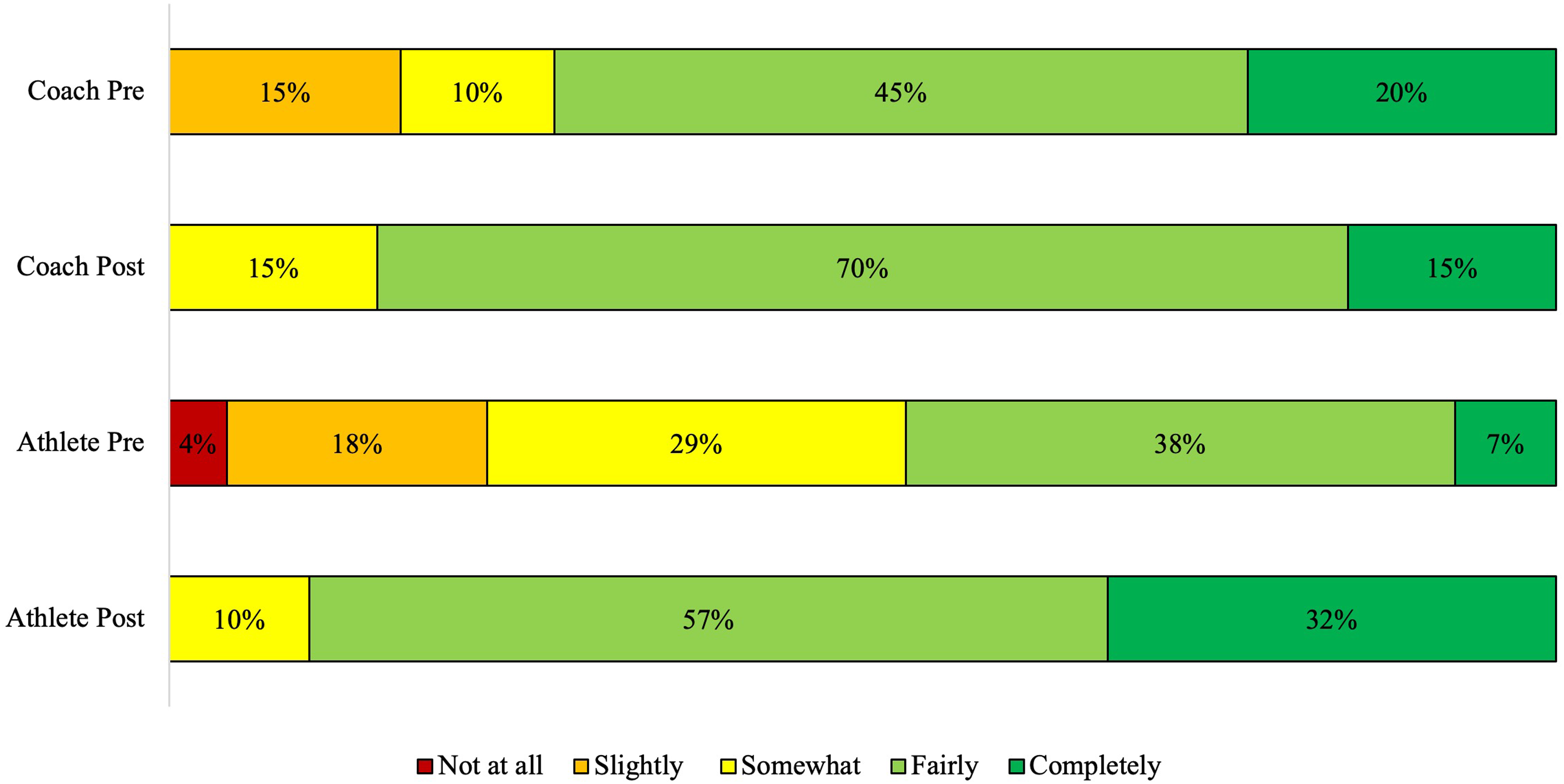
Confidence levels of coaches and athletes in identifying REDs signs/symptoms pre- and post- education session and panel discussion, ranging from not at all confident to completely confident. *denotes significant difference from pre- education session and panel discussion (p < 0.001).
Post-education session and panel discussion
Low libido was the most commonly identified sign/symptom learned at the education session and panel discussion. Others included incontinence, mental health, GI issues, cognitive impairments and other hematological abnormalities (Figure 1).
The confidence levels of coaches in identifying the signs/symptoms did not significantly change from pre-panel (p = 0.52, Figure 2), however; significantly improved in athletes from pre-panel (p < 0.001, Figure 2).
Experiences with REDs
Pre-education session and panel discussion - coaches
Diagnosis/Healthcare involvement
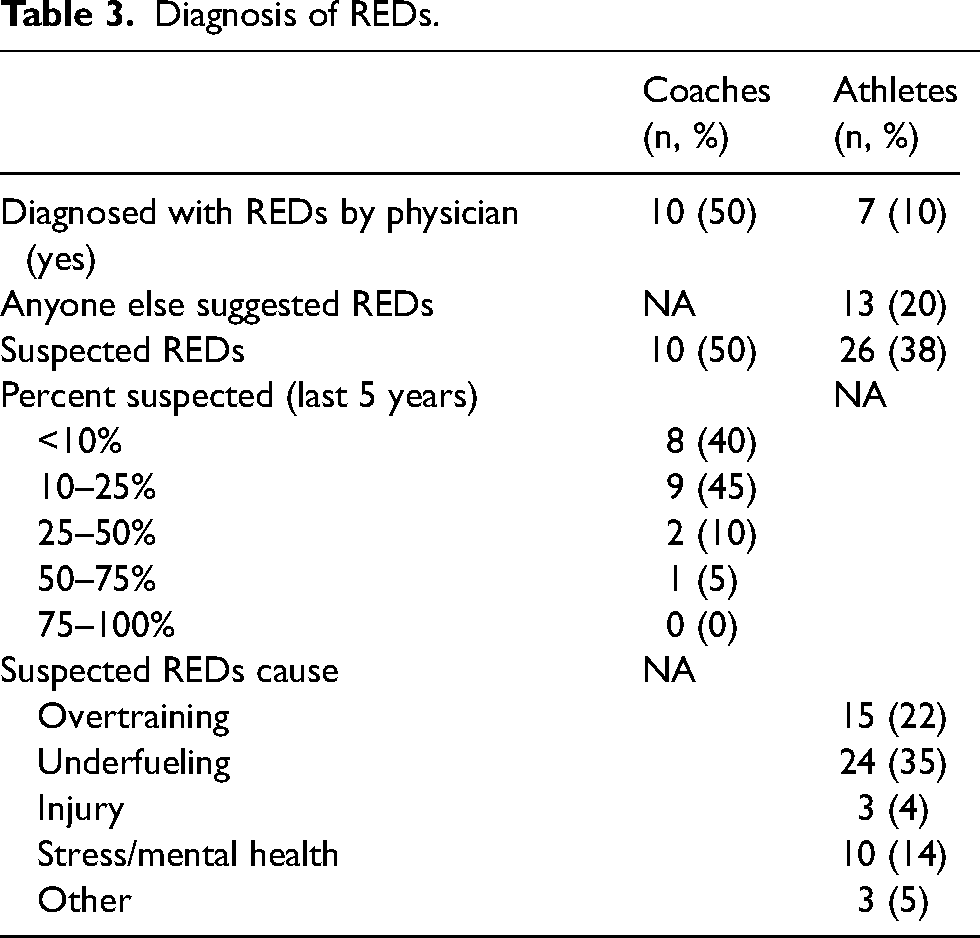
All coaches reported having experience or potential experience with an athlete having REDs in their career [50% (n = 10) responded yes, and 50% (n = 10) said no but suspected], and 45% (n = 9) suspected 10–25% of their total lifetime athletes had REDs (Table 3).
Diagnosis of REDs.
A total of 80% of coaches indicated they would recommend their athlete see a Sport Medicine Doctor for REDs treatment/management, and 70% also indicated they would recommend their athlete see a Sport Medicine Doctor for REDs treatment/management if they had unlimited resources (Table 4). The coaches’ most selected barrier for seeking REDs management/treatment was resources [e.g. limited access to specialists; 65%, n = 13] (Table 5). All coaches (100%, n = 20) stated they would seek immediate healthcare professional attention if their athlete were exhibiting signs/symptoms of REDs.
Involvement of healthcare practitioners in REDs treatment/management.
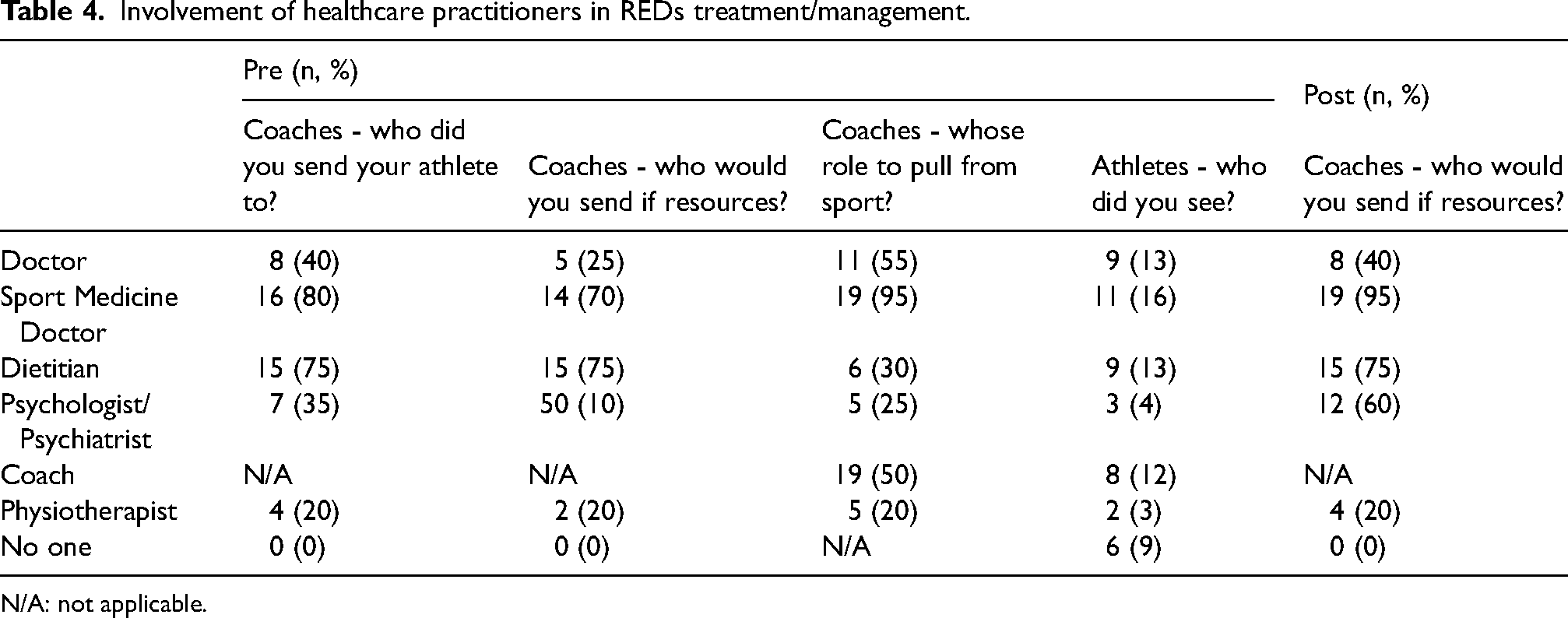
N/A: not applicable.
Barriers to care.
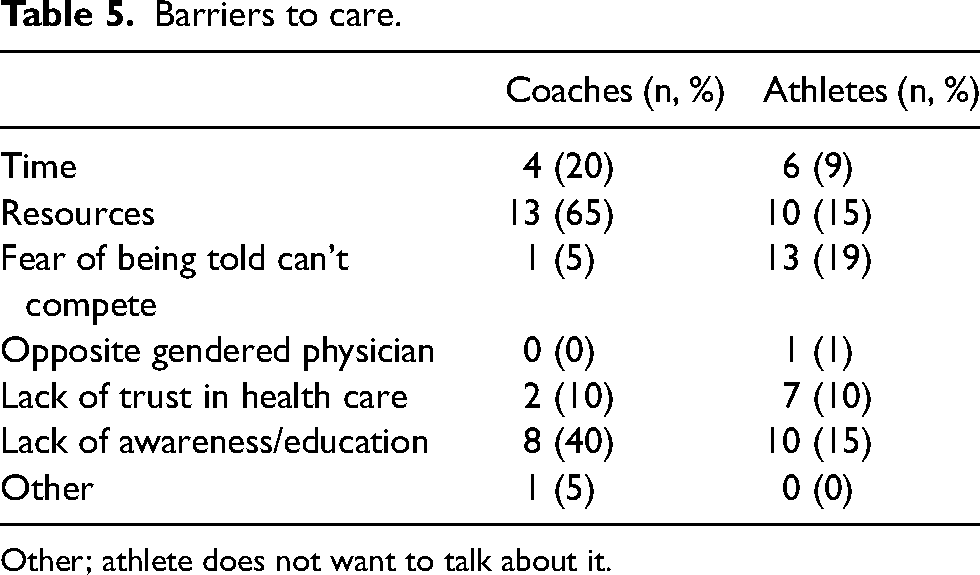
Other; athlete does not want to talk about it.
Training
The majority of coaches were somewhat (25%, n = 5) to completely comfortable (30%, n = 6) in providing a modified programme for an athlete exhibiting initial signs of REDs, however; were slightly comfortable (25%, n = 5) for an athlete with severe REDs/eating disorder (Figure 3). For those who felt fairly and completely comfortable, a common element in open text boxes included the importance of the athlete's health, whereas those who felt slightly or not at all confident stated they would appreciate medical guidance and that it can be a challenging conversation to have with their athlete.
Comfort levels of coaches and athletes in developing/asking for a modified training programme pre- and post- education session and panel discussion, ranging from not at all confident to completely confident. Initial REDs = exhibiting initial signs/symptoms, severe REDs = athletes with severe REDs and/or eating disorders. *denotes significant difference from pre- education session and panel discussion (p < 0.001).
Pre education and panel discussion – athletes
Diagnosis/Healthcare involvement
Survey responses indicated 10% (n = 7) of athletes had been diagnosed with REDs by a physician and 38% (n = 26) suspected they had REDs. When asked who the athlete saw for REDs treatment/management (select all that apply), 16% (n = 11) selected Sport Medicine Doctor and 9% (n = 6) selected received no treatment/management (Table 3). When athletes were asked what barriers have prevented them from seeking REDs treatment/management (select all that apply), 19% (n = 13) selected fear of being told they can’t complete (Table 5).
Training
A total of 35% or athletes indicated they were completely comfortable in telling their coaches if they suspected they had REDs (Figure 3). Similarly, 31% stated they were completely comfortable in asking for a modified training programme if they suspected they had REDs (Figure 4). Some common elements in open text boxes can be found in Figure 5.
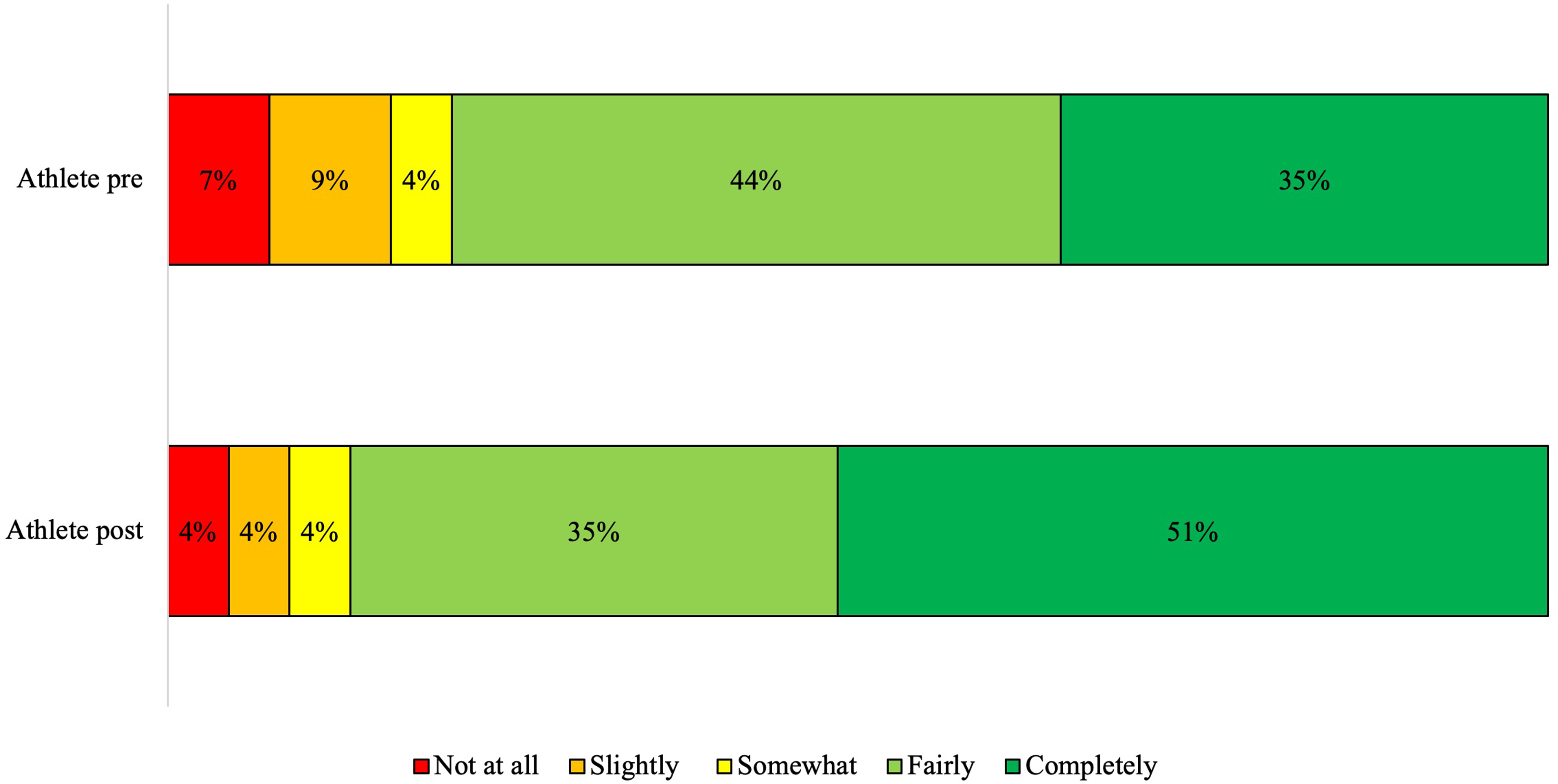
Comfort levels of athletes in telling coaches if they exhibited signs/symptoms of REDs pre- and post- education session and panel discussion, ranging from not at all confident to completely confident. *denotes significant difference from pre- education session and panel discussion (p < 0.001).
Post-education session and panel discussion
The comfort level in coaches developing a modified training programme for initial signs/symptoms (p = 0.77) or severe REDs/eating disorder (p = 0.19) did not significantly change after the education session and panel discussion (Figure 3).
The comfort level of athletes in telling coaches if they believed they were exhibiting signs/symptoms of REDs significantly improved (p < 0.001) after the education session and panel discussion, where most athletes at least fairly confident (86%, n = 59, Figure 4 and 5). Likewise, the comfort level of athletes asking for modified training programmes from their coaches significantly improved (p < 0.001), where most athletes were fairly (37%, n = 25) or completely (41%, n = 28) confident (Figure 4 and 5). Finally, when athletes were asked compared to before the education session and panel, if they were more likely to seek help, all athletes selected it depends (6%, n = 4), probably yes (41%, n = 28) or definitely yes (51%, n = 35). Some common elements in open-text boxes can be found in Figure 5.
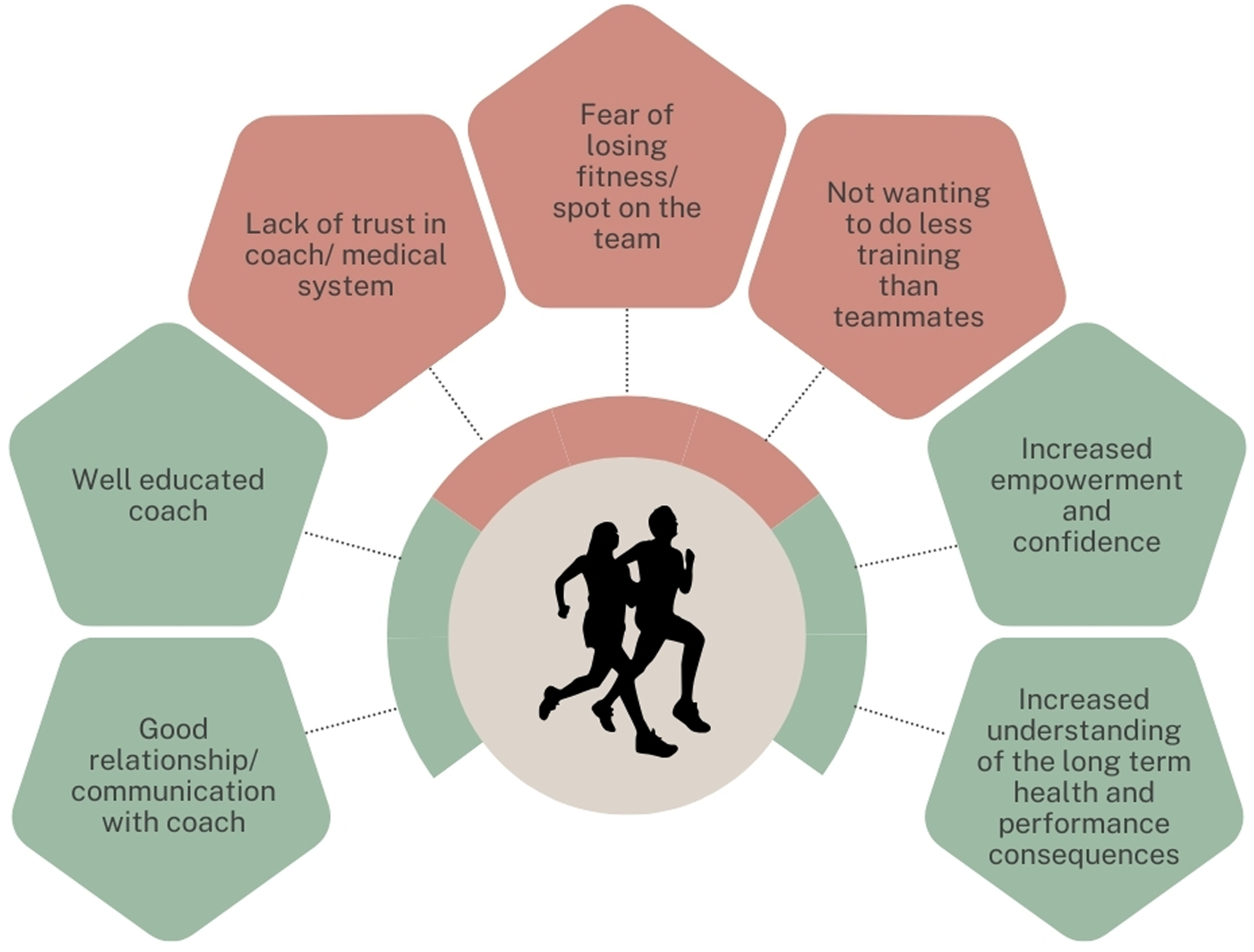
Common elements from open text boxes from athletes surrounding telling coaches if they believed they were exhibiting signs/symptoms of REDs, and comfort in asking for modified training programmes. One coach reported feeling more comfortable and empowered to make decisions surrounding modifying training loads.
Future directions
Most coaches (95%, n = 19) and athletes (74%, n = 50) strongly agreed that both coaches and athletes would benefit from more education surrounding REDs. Most also strongly agreed that the session was educational and helpful [coaches; 85% (n = 17), athletes; 81% (n = 55)] and something they would like to see implemented at the U SPORTS level [coaches; 80% (n = 16), athletes; 66% (n = 45)].
Discussion
The results of this study demonstrated that a panel discussion and education session given at the 2023 UXC was successful at improving athlete's confidence in recognition and reporting of REDs, but not coaches.
Prior to the education session and panel discussion, most coaches and athletes had adequate knowledge of the definition of REDs, the notion that REDs can affect both males and females, and the underlying cause of REDs. However, only 40% (n = 8) of coaches and 13% (n = 9) of athletes felt completely confident in their ability to correctly identify the underlying cause. Most studies on coaches’ knowledge have been surrounding the Female Athlete Triad. These studies have demonstrated that female coaches have more awareness and comfort when communicating with their female athletes about aspects of the Triad (e.g. menstruation) than male coaches.17,18 However, our study had 65% male coaches, which is consistent with Canadian numbers. For instance current coaching data demonstrates that women are underrepresented, with only 26% of U SPORTS and Canadian Collegiate Athletic Association being women. 19 Furthermore, barriers to coaches’ education surrounding the Triad include insufficient time, knowledge, and educational resources. 20 The coaches in this study showed similar results, where lack of resources (65%), lack of awareness/education (40%) and time (20%) were the top cited barriers that prevented them from seeking assistance for REDs management and treatment for their athlete(s). Athletes cited fear of being held back from competition (19%), lack of resources (15%) and lack of awareness/education (15%) as top barriers in seeking care for REDs management/treatment. Therefore, improved education for both coaches and athletes may promote earlier intervention and prevention of REDs.
Notably, athletes in our study who stated having a coach they felt was knowledgeable, supportive, and trustworthy reported they would be comfortable telling their coaches if they were exhibiting signs/symptoms and/or asking for a modified training programme. However, athletes who stated not having a strong relationship with their coaches, did not trust their coaches, did not believe their coaches were concerned about their health or were worried about losing their spot on the team felt less comfortable telling their coaches if they were exhibiting signs/symptoms and/or asking for a modified training programme. Previous qualitative studies have examined the athlete-coach relationship. For instance, a study on endurance athletes’ experiences with REDs demonstrated that a lack of professional support and information inhibited recovery. 21 Another study exploring rowing athletes’ experiences with low back pain demonstrated that athletes were more likely to conceal their pain from their coaches, peers and medical staff if they did not have a trusting relationship with their coach, or felt that it would influence their team selection. 22 However, athletes were more likely to disclose their pain if they had a good relationship with their coach, felt their coach was supportive and felt that there was a culture of openness. 22 Another study demonstrated that female athletes with eating disorders were less likely to seek assistance when they perceived a lack of emotional support from coaches, as they believed they did not know how to deal with them. 23 The coach can often be the first contact point for the athlete, and therefore should be knowledgeable in how to recognise REDs signs/symptoms early in order to mitigate long-term consequences.24,25 Furthermore, it is important that the athlete feels safe, supported and protected, and education of athletes and the athlete entourage can help keep sport safe. 26 Those in positions of leadership should take the responsibility onto themselves to support autonomy and create healthy, safe environments for athletes. 27 The results of our study and previous studies14–16 demonstrate that the coach can have either a positive or negative influence on an athlete's experience with REDs, depending on their openness, knowledge, communication and athlete-coach relationship. A focus of improved education for coaches and athletes can help protect athletes from both emotional and physical harm.
After an education session and panel discussion, the confidence in REDs knowledge and recognition among coaches did not significantly change. A previous study in NCAA DI coaches demonstrated that low bodyweight-sport coaches (cross-country, rowing) had greater knowledge and confidence than other sports, 28 therefore coaches in this study may have high knowledge and/or confidence due to the high-risk nature of cross-country. A review demonstrated that out of 600 websites with potential resources for coaches on eating disorders/disordered eating, only 24 were considered reputable, and none provided official training. 29 Therefore, although coaches may feel confident in their ability to recognise and manage REDs, there is a need for more comprehensive training resources and/or educational modules. This will help ensure a safe environment for athletes to train and compete, and will promote long-term athlete health and development.
After the education session and panel discussion, athletes were more confident in recognising the signs/symptoms of REDs, felt more comfortable in telling their coaches if they believed they were exhibiting signs/symptoms of REDs, asking for a modified training programme, and were more likely to seek help. Experience, communication, empowerment, knowledge, education, context and sport culture all play fundamental roles in injury prevention in elite athletes. 30 Additionally, education sessions in other areas, such as concussion, have been shown to improve knowledge, reporting and facilitation of attitudinal changes31,32 as well as associated with more favourable perceived social norms surrounding concussion care 33 in collegiate athletes. Furthermore, some studies have demonstrated improvements in knowledge of the Female Athlete Triad 9 and outcomes such as BMD 10 in athletes post-education intervention. Additionally, some peer-led educational interventions in female collegiate athletes have demonstrated improvements in eating disorder risk factors, as well as increased likelihood to seek medical consultation for the Female Athlete Triad. 34 Therefore, the implementation of early, sport-specific and the correct type of education programmes for athletes may improve knowledge, reporting and prevention of REDs and subsequent consequences. Furthermore, hosting education sessions at championships such as U SPORTS/NCAA provides an ideal opportunity to improve athlete and coach education, as it is a natural gathering of all key stakeholders. The education session and panel discussion at the U SPORTS Cross-Country Championships was very well attended and received and is something that athletes and coaches would like to see developed at a national level.
Limitations
There are limitations to this study that should be considered when interpreting the results. We cannot rule out reporting bias, as our sample was collected from athletes/coaches who were interested in attending an education session and panel discussion on REDs. Out of 365 athletes registered at the UXC, only 68 filled out the survey. Furthermore, out of 60 coaches, only 20 filled out the survey, therefore we were not adequately powered to compare results between athletes and coaches. Future studies should aim to increase participation through mandatory USPORTS training modules, and consideration of competition time and/or format changes (i.e. hybrid) to make it more accessible to all athletes and coaches beyond those who were present the day before competition. Additionally, as this was an initial study to explore the possibility of future educational interventions across U SPORTS, an in-depth evaluation of educational outcomes was not practical. It is also important to acknowledge that there may be ceiling effects in the confidence in REDs knowledge, recognition and reporting which may limit interpretation of results. For example, 60% of coaches felt either fairly or completely confident with identifying REDs signs and symptoms before the education session and panel discussion. Additionally, while the low number of women coaches who filled out the survey is consistent with Canadian numbers, there was a larger proportion of women competitors who filled out the survey, despite an almost even distribution of men and women registered for the event. Therefore, the results may not be generalisable to all genders. Furthermore, our sample was quite homogenous where 91% reported their ethnicity as white. Finally, the results of this study are not generalisable to all collegiate sports as we focused on cross-country; however, these results may be generalisable to other endurance sports in which REDs is a common occurrence.
Conclusion
An educational programme including a panel discussion with medical experts, researchers and athletes with lived experiences was effective at improving the confidence in REDs knowledge, recognition and reporting in cross-country athletes, but not coaches. The results of this study support the need for improved ways of reaching coaches to enhance athlete safety, reporting and management of REDs. Furthermore, behavioural changes that increase reporting among athletes and strengthen the athlete-coach relationship should be facilitated. Best practice guidelines to prevent REDs include primary prevention (education) among the athletes, their entourage and sport organisations, who all need to ensure a safe and supportive environment. Therefore, sport-specific, mandatory educational modules and panel discussions should be developed, along with exploration of knowledge dissemination strategies, to improve awareness of REDs in Canadian athletes and coaches and to facilitate long-term athlete health. Future studies implementing validated, educational-based interventions should be conducted to investigate changes in knowledge, behaviour and REDs risk factors, in addition to changes in confidence.
New findings
- An education session and panel discussion surrounding REDs significantly improved athletes’ comfort level in reporting REDs signs/symptoms to coaches and comfort level in asking for a modified training programme if exhibiting REDs signs/symptoms. - The session significantly improved athletes’, but not coaches’, confidence in identifying signs/symptoms of REDs. - Specific knowledge translation strategies should be developed to improve REDs knowledge and awareness, and to promote overall health and safety in sport.
Supplemental Material
sj-docx-1-spo-10.1177_17479541241305389 - Supplemental material for Mapping the gap: A study on the confidence in knowledge and reporting of relative energy deficiency in sport (REDs) in Canadian University cross-country coaches and athletes
Supplemental material, sj-docx-1-spo-10.1177_17479541241305389 for Mapping the gap: A study on the confidence in knowledge and reporting of relative energy deficiency in sport (REDs) in Canadian University cross-country coaches and athletes by Jenna M. Schulz, Chloe M. Hewitt, Trent Stellingwerff, Hilary Stellingwerff, Kathryn E. Ackerman and Jane S. Thornton in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-2-spo-10.1177_17479541241305389 - Supplemental material for Mapping the gap: A study on the confidence in knowledge and reporting of relative energy deficiency in sport (REDs) in Canadian University cross-country coaches and athletes
Supplemental material, sj-docx-2-spo-10.1177_17479541241305389 for Mapping the gap: A study on the confidence in knowledge and reporting of relative energy deficiency in sport (REDs) in Canadian University cross-country coaches and athletes by Jenna M. Schulz, Chloe M. Hewitt, Trent Stellingwerff, Hilary Stellingwerff, Kathryn E. Ackerman and Jane S. Thornton in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-3-spo-10.1177_17479541241305389 - Supplemental material for Mapping the gap: A study on the confidence in knowledge and reporting of relative energy deficiency in sport (REDs) in Canadian University cross-country coaches and athletes
Supplemental material, sj-docx-3-spo-10.1177_17479541241305389 for Mapping the gap: A study on the confidence in knowledge and reporting of relative energy deficiency in sport (REDs) in Canadian University cross-country coaches and athletes by Jenna M. Schulz, Chloe M. Hewitt, Trent Stellingwerff, Hilary Stellingwerff, Kathryn E. Ackerman and Jane S. Thornton in International Journal of Sports Science & Coaching
Footnotes
Acknowledgments
We would like to thank the panellists (Gabriela DeBues-Stafford, Laura Parkinson, Charlotte Prouse, Amanda Truelove, Jessica White and moderator Hana Marmura) for their time and expertise, as well as assistance with survey piloting/development. We would also like to thank Return to Health and Performance Lab members for assisting with survey feedback and usability.
Contributorship
JMS conceptualised the project, analyzed the data, and drafted the manuscript. CH, TS, HS and JST contributed to data collection. All authors contributed to conception, design and critical revision of the article. All authors edited and approved the final version of the manuscript.
Data sharing
Data can be accessed upon request to the corresponding author.
Declaration of conflicting interests
KEA is the Director of the Wu Tsai Female Athlete Programme.
Funding
This study was sponsored by a grant from the Wu Tsai Female Athlete Programme and Athletics Canada. JMS is supported by the Ontario Women's Health Scholars Postdoctoral Award and a Western's Bone & Joint Institute Collaborative Training in Musculoskeletal Heath Programme Trainee Award. JST receives funding as a Tier 2 Canadian Institutes of Health Research Canada Research Chair.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.