
Abstract
Background:
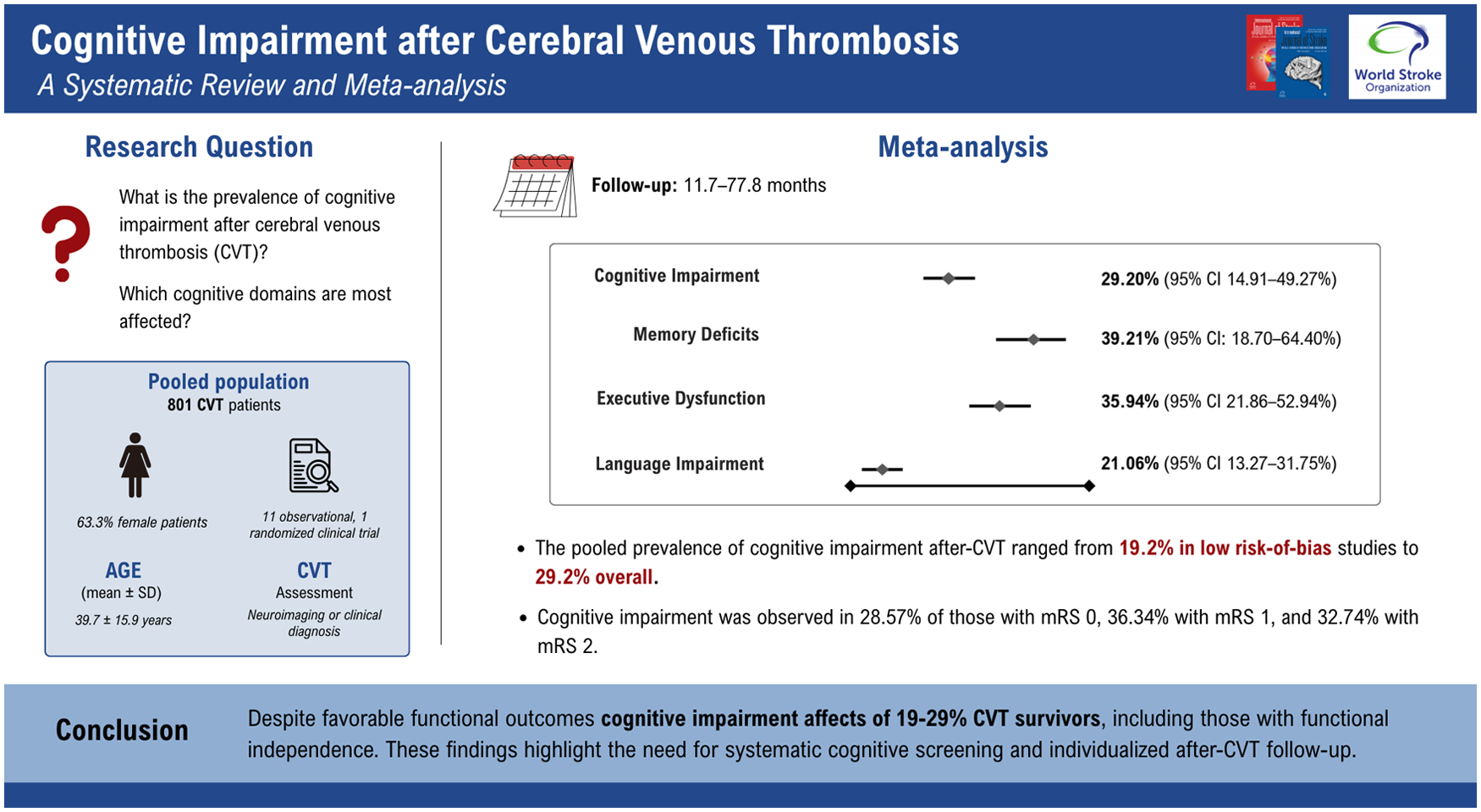
Cerebral venous thrombosis (CVT) is a less common type of stroke that predominantly affects young adults, particularly women. Although CVT is generally associated with more favorable functional outcomes than other stroke subtypes, its cognitive consequences remain poorly understood.
Aims:
We aimed to perform a systematic review and meta-analysis evaluating the prevalence and characteristics of cognitive impairment in patients after CVT.
Summary of review:
A systematic review was conducted in accordance with PRISMA guidelines. We searched PubMed, Embase, and Cochrane databases up to May 2025 for studies assessing cognitive impairment in patients with cerebral venous thrombosis (CVT), with a minimum follow-up of 6 months. Data extraction was performed independently by two reviewers. Pooled prevalence estimates were calculated using random-effects generalized linear mixed models with logit transformation as the primary approach, with Freeman–Tukey (double arcsine) transformation applied only in analyses with zero events or extreme proportions. Heterogeneity was evaluated using the I² statistic. All statistical analyses were conducted in R (version 4.5.2). Eleven observational studies and one randomized clinical trial involving 801 post-CVT patients were included. The pooled prevalence of cognitive impairment after CVT ranged from 19.25% (95% CI: 7.15–42.47%) among studies at low risk of bias to 29.20% (95% CI: 14.91–49.27%) in the overall analysis. Memory loss and affected executive function and visuospatial domains occurred in 39.21% (95% CI: 18.70–64.40%) and 35.94% (95% CI: 21.86–52.94%) of patients, respectively. Among functionally independent patients, cognitive impairment was observed in 28.6% (95% CI: 21.0–37.6%) of those with mRS 0, 36.3% (95% CI: 26.5–47.5%) with mRS 1, and 32.7% (95% CI: 15.5–56.3%) with mRS 2.
Conclusions:
Cognitive impairment affects roughly one-fifth to one-third of CVT survivors (19–29%), including those with minimal or no functional disability. These findings highlight the need to move beyond the mRS when assessing recovery and planning follow-up care.
Keywords
Get full access to this article
View all access options for this article.