
Abstract
Background
In Ethiopia, young women’s pregnancy is a serious public health issue that hurts the health outcomes of both the mother and child. However, no research has been done on the use of contraceptives to delay first birth and associated factors among married young women aged 15-24 in Ethiopia.
Objectives
This study aimed to assess the contraceptive use to delay first birth and its associated factors among married young women in rural parts of central Oromia, Ethiopia, in 2024.
Design
A community-based cross-sectional study design was employed.
Methods
The sample size for the study was 422 married young women. A census was conducted to obtain a sample frame, and a simple random sampling method was used to select the study participants. Data were collected using interviewer-administered structured questionnaires. The collected data were entered into EpiData version 4.6 and exported to SPSS version 23 for further analysis. Binary logistic regression analyses were performed to identify variables associated with contraceptive use to delay first birth, with a p-value of less than 0.05 considered significant.
Results
The overall contraceptive use to delay first birth among married young women was 16.3%, with a 95% CI (12.8, 20.3). The following were found to be factors associated with the use of contraceptives to delay first birth among married young women: exposure to contraceptive information. [AOR=4.36; [95% CI: (2.14, 8.86)], p=0.001], a favorable attitude toward contraceptive methods (95% CI: (1.72, 7.31)), and p=0.001]; intention to use contraceptives [AOR=4.16; (95% CI: (1.96, 8.84); p < 0.001)]; perceived social approval [AOR=3.48; (95% CI: (1.65, 7.35)); p=0.001]; beliefs about contraceptive myths at the community level) [AOR=3.74; 95% CI: (1.82, 7.66); p < 0.001); and family planning counseling [AOR=5.19; 95% CI: (2.43, 11.08); p < 0.001) were among the significant variables associated with contraceptive use to delay first birth among young married women.
Conclusions
The contraceptive use to delay first birth among married young women was low. Healthcare providers, policymakers, and program designers should intensify their efforts to create awareness about the importance of contraceptive utilization among young married women to delay their first birth.
Plain language summary
Young married people with exposure to contraceptive information were four times more likely to be contraceptive users than those with no exposure to contraceptive information. Furthermore, having a favorable attitude toward contraceptive methods, intention to use contraceptives, perceived social approval, good beliefs about contraceptive myths at the community level, and family planning counseling by healthcare providers were among factors that enhanced contraceptive use to delay first birth among young married women.
Introduction
Globally, it has been estimated that 16 million females aged 15–24 give birth each year, with 90% occurring within marriage. 95% of these births occur in low- and middle-income countries (LMICs), including Sub-Saharan Africa (SSA). 1 The use of modern contraceptives is crucial for individuals and couples to realize their fundamental right to choose freely and responsibly whether to have children, when to have children, and how many children to have. 2 In addition to improving health-related outcomes, including lower maternal and neonatal mortality, monitoring rapid population growth, gender inequity, improvements in schooling, and opportunities for economic empowerment. 3 However, global gender disparities place young women at a disadvantaged social position, and sexual and reproductive health and rights issues disproportionately affect women. 4 Their lower social status within their families and communities often undermines young women’s decisions about whether, when, and how many children to have, leading to early and unwanted pregnancies. 5
Approximately 14 million young women in low- and middle-income countries would like to prevent, delay, or avoid pregnancy by utilizing modern contraceptives. 6 Furthermore, studies have indicated that young women who have never been married are more likely to use modern contraceptives to prevent unintended pregnancies, while married women are often confronted with pressure to have a child soon after marriage.7,8
As a result, approximately 21 million young women in LMICs become pregnant every year, of which 50% are unintended, leading to an increased risk of eclampsia, puerperal endometritis, systemic infections, neonatal morbidities, and maternal death, particularly among those aged 15-19 years. 9 Furthermore, most girls leave school following marriage and focus on domestic duties, pregnancy, and raising children.10,11 Nowadays, more young women exist in the world, with approximately one in every five people, mostly in developing countries. 12
In Ethiopia, about 63.5% of women ages 15-24 who are currently married are not using contraception. 13 As a result, unwanted pregnancies among young married women are more than double that of married women over 25 years old.14,15 A mixed-method study conducted on contraceptive prevalence rate and associated factors among married young women in four emerging regions of Ethiopia showed that 11.7%, 38.6%, 25.5%, and 8.8% for Afar, Benshangul Gumuz, Gambela, and Somali regions, respectively. 16
According to a report by Population Services International (PSI), four out of five girls in Ethiopia become mothers by age 20 without considering the financial consequences. 17 Additionally, three out of four Ethiopian females between the ages of 15 - 24 years use their first contraceptive after giving birth to two or more children.18,19 As a result, it hurts maternal and neonatal mortality, school attainment, productivity, and poverty. 20 Thus, contraceptive use to delay first birth among married young women is crucial to reducing maternal and child mortality, preventing married young women from falling into poverty, and achieving sustainable development goals. However, most research conducted in Ethiopia has been limited to contraception use for spacing of births among women of reproductive age, not among married young women. Therefore, this study aims to assess the contraceptive use to delay first birth and its associated factors among married young women in rural parts of central Oromia, Ethiopia.
Methods
Study area and period
The study was conducted in Goro woreda of Southwest Shewa Zone, Oromia Regional State, 135 km away from Addis Ababa, the capital city of the country. The woreda has 19 rural kebeles with four primary health centers, 19 health posts, and 5 private clinics providing primary health care services, including family planning services. The total population is 66,815, of which 32,739 are male, and 34,076 are female. The estimated number of women aged 15-24 was 8,280 in rural kebeles. The study was conducted from August 1 to September 30, 2024.
Study design
A community-based cross-sectional study design was employed.
Source population
All married females aged 15-24 years residing in the Goro woreda.
Study population
All selected married females aged 15-24 residing in the Goro woreda.
Sample size calculation
The sample size was determined using the single population proportion formula, with the following assumptions: Z = 95% confidence interval (1.96), d = margin of error (5%), and proportion of participants (p = 50%) because no study had been done before on this concept.
n
Sampling techniques
Initially, a simple random sampling technique was used to select 9 kebeles, assuming the kebeles were homogeneous. Then, married women aged 15-24 were identified by conducting a house-to-house listing by selected community health workers to have a sampling frame. The calculated sample size was proportionally allocated to select kebeles based on the number of married women aged 15-24 identified and the calculated sample size for the study. Due to inadequate resources or the absence of funding, study samples were selected using a simple random sampling technique from a sampling frame. Three times, a repeat visit was made for women who were not at home during data collection to reduce the non-response rate (Figure 1). The schematic diagram representation of sampling procedures to identify the prevalence of delaying first birth and associated factors among young married women in Goro Woreda, central Oromia, Ethiopia, in September 2024.
For proportional allocation of a sample:

Study variables
Dependent variable
Contraceptive use to delay the first birth
Independent variables
Sociodemographic and economic status, Knowledge, Attitude, intention to use, exposure to information, perceived social approval, and community-level factors (belief and support).
Inclusion and exclusion criteria
Inclusion
Women aged 15 to 24 years, of marital status, residing in the study area for at least six months, who consented to participate, were included in this study.
Exclusion
Women with serious health conditions in previous births and non-consent were excluded from this study.
Operational definition
Data collection tools and procedures
The collection tools were adapted from different literature after being modified to the local context, and content validity was checked by the Delphi method23,24,26,28,31,32 (Supplementary tools). The tools contain socio-demographic and economic status factors associated with contraceptive use, such as knowledge, attitude, intention, perceived social approval, beliefs, myths about contraception, and community support. Data were collected using an interviewer-administered structured questionnaire. Unique identification number for an eligible household used to locate young married women. Finally, data were collected by three midwifery professionals trained on the objectives and methods of the study and one supervisor.
Data quality
The questionnaire was prepared in English and then translated into local languages (Afan Oromo and Amharic) and then back-translated to English by independent language experts to ensure clarity and consistency of the tools. To ensure the quality of data, a day of training was given for data collectors on the objective and methods of the study, data collection procedures, the content of the questionnaires, and ethical issues. A pretest was conducted on 5% of the total sample to assess the tool’s simplicity and flow outside the study area to prevent information contamination. Based on the findings from the pretest and mock interview, necessary modifications have been made to the tool whenever needed. The data were checked for completeness and consistency before leaving the household, and necessary checks were done before data entry, cleaning, and analysis. The supervisors made ongoing checkups during the data collection.
Ethical considerations
This study was conducted in accordance with the declarations of Helsinki and was approved by the Institutional ethical review board of the Jimma University Institute of Health, Institutional Review Board with ethical approval reference number JUIHIRB 75/24. The study participants were informed on the study's objectives, procedures, potential risks, benefits, and voluntary participation,n and confidentiality was maintained. This study included participants with poor literacy levels, as a result, written consent was waived, and verbal informed consent was secured from the study participants before data collection. For participants under 18, consent from parents or guardians was waived, as the Ethiopian National Research Ethics Review Guidelines allow married or parenting minors to give consent themselves.
Statistical analysis
The STROBE checklist was used to report findings from this study (Supplementary file: STROBE checklist). 33 The data were checked, coded, and entered into EpiData version 4.6 and then exported to SPSS version 23 for further analysis. Descriptive analysis was used for the presentation of socio-demographic data and the prevalence of contraceptive use to delay first birth. A binary logistic regression analysis was conducted to identify variables that were candidates for multiple logistic regressions, having a p-value ≤ 0.25, to control for confounding factors. 16 All candidate variables were entered together into a multivariable logistic regression using the enter method to determine the factors associated with contraceptive use to delay first birth by controlling for potential confounders. The independent variables were checked for multicollinearity by using the variance inflation factor. (VIF) and tolerance test (TT). All variables yield a variance inflation factor <10 (VIF < 1.323) and tolerance>0.1(TT>0.756), and they were not removed from multivariable analyses. Hosmer and Lemeshow’s test was used to determine the model’s fitness (p = 0.445). Finally, independent variables’ AOR with a 95% confidence interval at a p-value < 0.05 were used to declare the statistical significance.
Results
Shows the sociodemographic and economic status of study participants in rural kebeles of Goro District, central Oromia, Ethiopia, 2024.

*Daily laborer/car driver, USD, United States Dollar.
Prevalence of contraceptive use to delay first birth among married young women
Only 66 (16.3%) of the respondents, with a 95% CI (12.8-20.3), were using modern contraceptives to delay their first birth. Among them, Depo-Provera was the most commonly used method, 39 (9.4%), followed by implants, 16 (4%), and contraceptive pills, 11 (2.7%).
Knowledge status of participants
Knowledge level of study participants about modern contraceptive methods in Goro Woreda, central Oromia, Ethiopia, September 2024.

Attitude status of participants
Attitude of study participants about modern contraceptive methods in Goro Woreda, central Oromia, Ethiopia, September 2024.

SA: Strongly agree, A: Agree, U: Unknown, D: Disagree, SD: Strongly disagree.
Intention to use contraception status
Shows the respondents’ level of intention to use modern Contraceptives in Goro Woreda, Oromia, Ethiopia, September 2024.
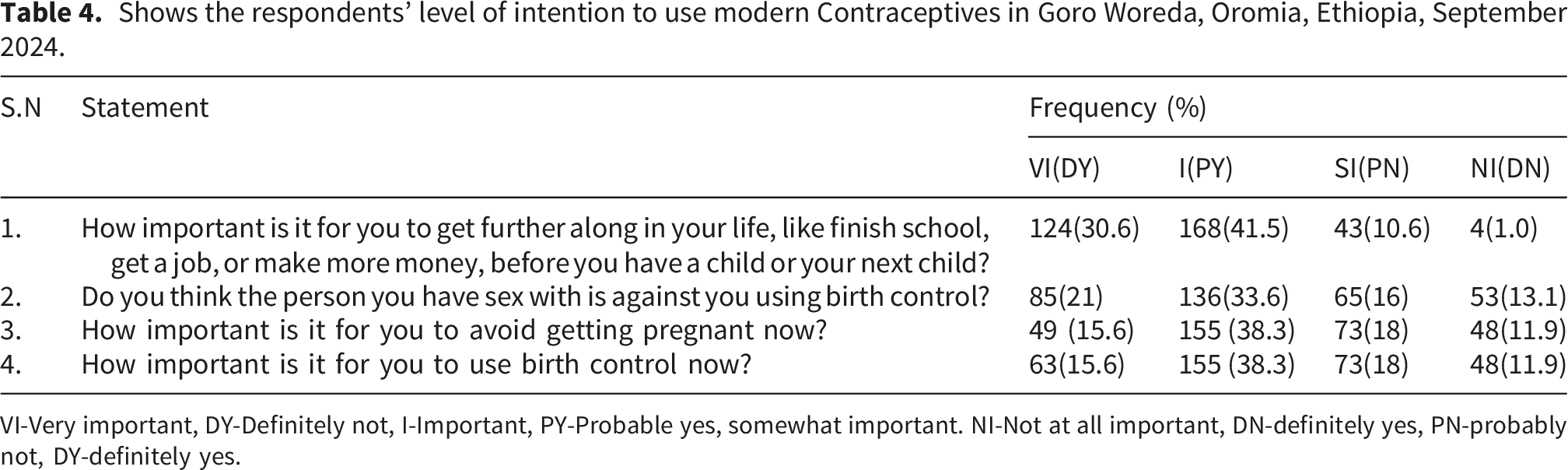
VI-Very important, DY-Definitely not, I-Important, PY-Probable yes, somewhat important. NI-Not at all important, DN-definitely yes, PN-probably not, DY-definitely yes.
Perceived social approval
Shows the level of perceived social approval regarding contraceptive use of the respondents on modern contraceptive methods in Goro woreda, Oromia, Ethiopia, September 2024.

SA: Strongly agree, A: Agree, U: Unknown, D: Disagree, SD: Strongly Disagree.
An individual believes in contraception myths
Shows community-level beliefs in contraception myths on modern contraceptive methods in Goro Woreda, Oromia, Ethiopia, September 2024.

SA: Strongly agree, A: Agree, U: Unknown, D: Disagree, SD: Strongly disagree.
Community-level enhancing factor to use of modern contraceptives to delay the first birth
Shows community level support to use modern contraceptives to delay first birth in Goro woreda, Central Oromia, Ethiopia, September 2024.

Counseling on modern contraceptive methods.
Around 157 (43.2%) of respondents had been counseled by healthcare professionals on modern contraceptive methods, while 248 (56.8%) were not counseled.
Factors associated with contraceptive use to delay the first birth
Bivariate logistic regression analysis for factors associated with contraceptive use to delay the first birth among married young women at Central Oromia, Ethiopia,2024.

In multivariable analysis, variables such as exposure to information about contraceptives, attitude towards contraceptives, intention to use contraceptives, perceived social approval, beliefs in contraceptive myths, and counseling on contraceptive methods were found to be factors associated with contraceptive use to delay first birth at a P value of less than 0.05 and 95% CI. Multi-collinearity among independent variables was checked using the variance inflation factor (VIF), and model fitness was evaluated using Hosmer-Lemeshow’s goodness-of-fit test.
Women who had information about modern contraceptives were 4.4 times more likely to use contraceptives than their counterparts (AOR=4.36; 95% CI: 2.14-8.86). Women who had favorable attitudes towards modern contraceptive methods were 3.54 times more likely to use contraceptives to delay first birth than those women who had unfavorable attitudes (AOR=3.54; CI: 1.72, 7.31). Regarding the intention to use contraceptives by young married women who had the intention to use contraceptives were 4.16 times more likely to use contraceptives to delay their first birth than those who had no intention to use contraception (AOR=4.16; CI: 1.96, 8.84).
Women who had perceived that their referents approved of their contraceptive use were 3.48 times more likely to use contraceptives for delaying their first birth than those who did not perceive referent approval (AOR=3.48; 95%CI: 1.65, 7.35). Respondents living in a community that does not believe in contraceptive myths were 3.74 times more likely to use contraceptives to delay their first birth compared to those living in a community that holds such beliefs (AOR = 3.74; 95% CI: 1.82, 7.66).
Multivariate logistic regression analysis for factors associated with contraceptive use to delay the first birth among married young women in Central Oromia, Ethiopia,2024.

FP Family planning, 1 reference group, CM/M Contraceptive myths or misconceptions, Referents: close family or friends encourage to use contraceptives *(p<0.25) in bivariate, **= statistically significant in multivariable at p-value <0.05.
Discussions
Young women’s pregnancy is a serious public health issue that negatively affects both the mother’s and the child’s health. However, limited studies have been done on the use of contraceptives to delay first birth and associated factors among married young women aged 15-24 in Ethiopia.
This study revealed that the magnitude of contraceptive use to delay the first birth was lower when compared to studies conducted in four emerging regions of Ethiopia (22.2%) and India (21.49%), in Latin America and the Caribbean (29.0%).16,21,33 The reason for the discrepancy might be due to fear of infertility and the pressure from family to conceive immediately after marriage in the study area, different study settings, and sample size.
In multivariable analysis, having exposure to information about contraception, attitude towards FP, intention to use contraception, perceived social approval, belief in contraception myths, and counseling on contraceptive methods were factors affecting contraceptive use to delay first birth among respondents.
In this study, women who had exposure to family planning messages from at least one media platform were over four times more likely to delay the first birth than those who did not. This finding is supported by studies conducted in Nigeria, Senegal, the Philippines, and Myanmar.34–36 This might be because mass media remains a vital source of information, and can raise awareness, increase knowledge levels, influence attitudes towards contraceptive use to delay first birth, and address social and cultural barriers to contraceptive use. 37
Current contraceptive use is over three times more likely among those who had a favorable attitude towards modern contraceptives used to delay their first birth than those who had an unfavorable attitude. This finding is supported by studies conducted in low- and middle-income countries, Nigeria, and Northwest Ethiopia.22,32,38 This might be due to pro-natal attitudes, which act as social scripts that women are expected to follow and may discourage the use of contraceptives through increased pressure on young women to secure their marriage and gain respect.39,40
The study also revealed that the odds of modern contraceptive use delaying first birth among married young women were higher among respondents who intended to use modern contraceptives than their counterparts. This finding is in line with a study conducted in Kpando Municipality, Ghana. 41 The possible explanation might be that the intention to use family planning is a motivational factor that influences family planning use, and greatly influences contraceptive use behavior. Therefore, it is an important indicator of the potential demand for services. 42
This study showed that the odds of contraceptive use to delay the first birth were three times more likely among married young women who strongly perceived their referents’ approval of their contraceptive use than those who did not perceive their referents would approve of their contraceptive use. This finding is in line with studies conducted in Nigeria, Guinea, Bale Zone, and rural Ethiopia.23,29,43,44,45 This indicates that perceived approval or disapproval by the woman is a much stronger determinant of modern contraceptive use, due to the socio-cultural pressure to prove fertility immediately after marriage and norms that encourage large family size in rural settings of some low- and middle-income countries.32,46,47
Respondents who lived in communities where there was a strong belief in modern contraceptive myths had at least three times fewer odds of using contraceptives to delay their first birth than those who lived in communities where there was no belief in contraceptive myths. This is consistent with the findings of studies conducted in Kenya and rural Ethiopia, which show that the fewer young women who believe in contraceptive-related myths and misconceptions, the higher the likelihood of reporting contraceptive use.23,48 A possible explanation might be that contraceptive-related myths and misconceptions are learned from social networks, which leads to social disapproval of contraceptives at a young age and prevents young women from using modern contraceptive methods. 49
The findings of this study are inconsistent with the study conducted in urban Africa, which showed that increased community-level belief in myths regarding contraceptives among women was positively associated with contraceptive use in Nigeria. This difference might be due to the correct information about the mechanism of action and potential side effects of modern methods provided, the socio-geographic difference in which all of the participants were urban residents, and there might be measurement errors during data collection among these urban Nigerian populations. 10
Furthermore, using contraceptives to delay the first birth was more than five times more likely among respondents who had been counseled on modern contraceptive methods than those who had never been counseled. This study result is in line with a related study conducted in rural Uttar Pradesh (India) and the Metekel Zone in Northwest Ethiopia.24,50 This might be due to counseling providing opportunities for information exchange to support a choice that fits the reproductive needs and goals of women and helps them to be aware of social norms regarding marriage and fertility expectations, as well as other cultural barriers, to make informed decisions about family planning service utilization. 50
Limitations
Due to the nature of the cross-sectional study design, the causal relationship of contraception use to delay first birth and its associated factors was not examined. So, strong study designs like follow-up and randomized control trial studies are recommended for future researchers to address causal relationships. 51
Implications of the study
The findings from this study can inform the stakeholders in the development of targeted interventions, such as exposure to contraceptive information, having a favorable attitude, intention to use contraceptives, perceived social approval, and good beliefs about contraceptives and family planning counseling by healthcare providers, which were among the factors for delaying first birth among young married women. The study highlights the need for behavioral interventions (KAP) aimed at changing mindsets by educating the public about the health benefits of delaying the first birth in young married women. Moreover, the results from this cross-sectional study were instrumental in designing an intervention to enhance the uptake of modern contraceptive methods by young married women to delay their first birth in Ethiopia.
Conclusions
This study indicates a low prevalence of contraceptive use to delay the first birth among married young women. Exposure to information, attitude, and intention to use contraceptives, perceived social approval, belief in contraceptive myths, and counseling on modern contraceptive methods were some of the factors associated with contraceptive utilization among young married women. Therefore, healthcare providers, policymakers, and program designers should work on raising awareness of contraceptive use to delay the first birth among young married women.
Supplemental material
Supplemental Material - Prevalence of contraceptive use to delay first birth and its associated factors among married young women in rural parts of central Oromia, Ethiopia: A community-based cross-sectional study
Supplemental material for contraceptive use to delay first birth and its associated factors among married young women in rural parts of central Oromia, Ethiopia: A community-based cross-sectional study by Hawi Gobena, Desta Workneh, Zinash Teferu, Bontu Mathewos, Endashaw Fantaye, Meseret Birhanu, Gadisa Bekele and Rebuma Sorsa in Women’s Health.
Footnotes
Acknowledgments
Our heartfelt gratitude also goes to all data collectors, supervisors, and respondents, without whom this thesis would not have been realized.
Ethical considerations
This study was conducted in accordance with the declarations of Helsinki and was approved by the Institutional ethical review board of the Jimma University Institute of Health, Institutional Review Board (JUIHIRB) approval number 75/24. As the study was community-based and involved participants with poor literacy levels, written consent was waived, and verbal informed consent was secured from all participants before data collection.
Consent for publication
The informed consent provided by the participants included the use of their anonymous data for study documents and the communication of the study results.
Author contributions
Hawi Gobena, Desta Workineh, and Gadisa Bekele were involved in the selection of articles, proposal writing, designing the study, data extraction, and statistical analysis. Rebuma Sorsa, Zinash Terefu, Meseret Birhanu, Bontu Mathewos, and Endashaw Fantaye were variously involved in the conceptualization, writing the first draft of the manuscript, and editing of the manuscript. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to this article.
Data Availability Statement
Supplementary materials and data can be provided based on your reasonable request to the corresponding author via
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.