
Abstract
Background:
Among Black women (BW), HIV prevalence is higher among women aged ⩾45 than among those aged <30 years. Pre-exposure prophylaxis (PrEP), a highly effective biomedical HIV prevention method, could be effective at reducing HIV incidence among this population.
Objectives:
To identify PrEP program features most important to aging BW and to examine how these preferences can inform program design using discrete choice experiment.
Design:
We employed secondary data analysis using a choice-based conjoint analysis (CBC), a discrete choice experiment technique.
Methods:
Between June and August 2024, 390 cisgender BW were recruited online, screened for eligibility, provided e-consent, and completed a one-time CBC survey of 14 choice tasks across 6 PrEP program attributes: (1) administration method, (2) access location, (3) healthcare integration, (4) provider demographics, (5) payment options, and (6) support services. We examined PrEP program preferences only among those aged ⩾45 (N = 83 of N = 390). Hierarchical Bayes model estimated attribute importance; latent class multinomial logit analysis grouped participants by similar preferences.
Results:
PrEP administration method was the top-ranked attribute (39%), followed by provider demographics (14%) and payment options (13%). Preferences were clustered into three distinct groups. Group 1 (n = 8) showed higher proportions of worry about acquiring HIV and preferred only a daily pill by a doctor’s office. Group 2 (n = 35) faced descriptively higher HIV vulnerability and favored injectable PrEP via telehealth supported (in-person) injection delivery from a female provider. Group 3 (n = 40) had the strongest interest and intention to use PrEP, preferring injectable PrEP from a pharmacist of the same race. Compared to the full sample, aging BW valued PrEP administration, prioritized gender matching alone, and payment options.
Conclusion:
PrEP program preferences are not uniform among aging BW. Rather than relying on a single PrEP delivery model, programs should be tailored to specific preferences for aging women who consider multiple factors and may need personalized support in PrEP decision-making.
Introduction
HIV disproportionately affects Black adults in the United States, with aging adults (⩾45 years) experiencing persistent disparities. While HIV incidence among individuals ⩽24 years has declined by ~30% in recent years, rates among those ⩾45 remained stable.1–4 Black adults represent the largest proportion of people over 40 living with HIV, with Black women (BW) being especially impacted.1–4 In fact, aging BW represent the majority of new HIV infections among all women older than 40.1–4 Despite these disparities, BW have the lowest pre-exposure prophylaxis (PrEP) uptake relative to need,5,6 highlighting a critical gap in HIV prevention for this population.
PrEP, an FDA-approved antiretroviral medication, reduces HIV acquisition via sexual contact by more than 95% when taken as prescribed.7–12 PrEP has been available as a daily oral pill13,14 for 10 years, and as a bi-monthly injection (long-acting injectable (LAI) PrEP) for 4 years in the United States (December 2021).7–9,11–15 Yet, only an estimated 2% of PrEP-eligible BW use PrEP.5,6 This inequity persists as BW, especially aging BW, remain underrepresented in US PrEP research and interventions compared with other priority populations.16–23 Multiple barriers hinder uptake, including individual (e.g., low perceived HIV vulnerability, low PrEP awareness and knowledge, medical mistrust), interpersonal (e.g., PrEP and HIV stigma, social norms), and structural factors (e.g., cost, access, discrimination, limited marketing, and PrEP messaging).16–19,22,24–29 Targeted research is needed to identify intervention strategies that both reduce HIV vulnerability and improve PrEP uptake among aging BW. 30
Few interventions address the needs of aging BW,16,19,23,31–35 who have been rarely prioritized in PrEP campaigns.21,35–39 This neglect is largely due to misconceptions and ageist stereotypes, 40 portraying aging women as sexually inactive,41,42 and by the false narrative that HIV only affects young people.30,43 These assumptions overlook the fact that many adults over 45 have active sex lives, 44 with some engaging in sexual behaviors (i.e., condomless sex, multiple sexual partners) that increase their vulnerability for acquiring sexually transmitted infections (STIs), including HIV.30,45–48 A systematic review identified multiple contributors to HIV vulnerability among aging BW, including behavioral (inconsistent condom use, sexual partners with undisclosed sexual encounters/behaviors), psychological (low-risk perception, depression/stress, trauma, low self-esteem), social (economics, education, and drugs/alcohol-use), and relationship factors (power imbalances, intimate partner violence, difficulty negotiating condom use). 30 Additional barriers include discomfort discussing sexual health and/or sexual practices with providers or partners, stigma, inadequate provider training, and cultural norms that limit open communication about sexuality. 49 Given the unique combination of behavioral, psychological, social, and relationship factors, PrEP offers an important opportunity to reduce persistent HIV disparities and enhance sexual health autonomy among aging BW. Moreover, PrEP was approved in the United States in 2012, making it a relatively new prevention method compared with condoms, which aging BW have known about for many years. If PrEP is not discussed within their social networks, this can contribute to lower awareness and utilization among this group. Many aging BW also lived through or were deeply affected by the early HIV epidemic of the late 1980s and early 1990s. Their lived experiences should be central to research on newly developed biomedical interventions. Tailoring PrEP interventions to their lived realities acknowledges their often-overlooked HIV vulnerability and affirms their right to comprehensive HIV prevention. Understanding their specific needs and preferences is essential to ensure that PrEP programs are both accessible and effective for this population.
Few studies have examined which PrEP intervention program features aging BW prioritize.29,50–53 To address this gap, the current study used discrete choice experiment (DCE) to evaluate BW’s preferences for specific PrEP program attributes. DCEs have been widely used in HIV research to quantify stakeholder preferences and inform program development, including preferences related to HIV testing, care and service delivery, antiretroviral therapy, and PrEP programs.50,53,54 This method assumes individuals evaluate an intervention as a set of attributes (e.g., administration method, access location) and assign value to each. Using these value estimates, we conducted a segmentation analysis to identify groups of aging BW with similar preferences to inform the design of more responsive PrEP delivery models. The purpose of this secondary data analysis was to inform optimal program design by using choice-based conjoint analysis (CBC), a type of DCE, to: (1) assess PrEP interest among aging BW (i.e., aged ⩾45); (2) compare key PrEP program preferences of aging BW (N = 83) with those of the full sample (N = 390); and (3) provide suggestions on how these preferences can inform better-designed programs in the US South.
Methods
Recruitment and eligibility criteria
The reporting of this study conforms to the STROBE statement. 55 This article reports a secondary analysis of the ⩾45 subgroup from a broader online DCE (parent N = 390; June–August 2024). Participant flow and derivation of the analytic sample are shown in Figure 1. All study activities were conducted online and in English. The Institutional Review Board at Florida International University (IRB-23-0283-AM01) and the University of Texas Health Science Center at San Antonio (STUDY00001802) approved the study protocol. Study participants were recruited through social media ads, printed flyers, email listservs, and snowball sampling. Flyers were placed in locations frequented by BW, and study information was also shared through listservs from community-based organizations, HIV service agencies, and health agencies. To be eligible, participants had to self-report being: (1) at least 18 years old; (2) a cisgender woman; (3) Black (i.e., African American, Caribbean American); (4) HIV-negative or unknown serostatus; (5) residing in a US Southern state (Alabama, Arkansas, Delaware, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia); and (6) engaged in at least one behavioral indicator of HIV exposure that may increase vulnerability to acquiring HIV within the past 6 months ((i.e., condomless vaginal and/or anal sex with a male partner; injection drug use; sex exchange; diagnosed with a STI) (not including HIV)). These indicators of HIV exposure were chosen based on HIV “risk” and PrEP eligibility criteria established by the National Institutes of Health (NIH) and the Joint United Nations Programme on HIV/AIDS (UNAIDS), which include condomless vaginal or anal sex (particularly with a partner whose HIV status is unknown), injection drug use, recent STI diagnosis, and sex exchange.56–58 These indicators are commonly used in clinical and public health settings to guide PrEP eligibility and were included to describe participants’ sexual behavior profiles rather than to generate a validated HIV risk score.

Enrollment flow chart for parent study and secondary data analysis study samples.
Enrollment procedures
Interested individuals accessed the study webpage via Qualtrics (Qualtrics, Provo, UT, USA) where they received study details, completed electronic consent, and were immediately directed to the eligibility screener. Eligible individuals who provided consent were directed to a one-time Qualtrics survey that collected demographic and characteristic information, HIV vulnerability, and PrEP awareness, interest, and intention. The survey included a CBC task housed in Sawtooth®. Participants who completed the survey and CBC task, and passed all validity procedures, received a US $50 electronic gift card by email.
Fraud detection and validity procedures
All survey responses were monitored for potential fraud from the start of data collection. An expanded version of fraud detection protocols developed by the PI of this study 59 was used to screen for duplicate or multiple survey entries, remove participants who did not meet eligibility criteria (e.g., not living in the US South), and detect and remove automated responses from bots. Speeder rules were applied to flag respondents who completed the survey in an unreasonably short time relative to the median completion time (i.e., less than 10 min); these cases were reviewed and excluded if data quality appeared compromised. Missing-data handling was enforced by preventing item skipping within the Qualtrics survey; any incomplete or invalid responses were excluded from analysis. The participation flow was tracked, including the number of individuals who accessed the survey, met eligibility criteria, and completed the survey. A $50 incentive was provided to participants who completed the survey and passed all validity checks, ensuring compensation for verified respondents. These fraud detection and validity control protocols have been previously published. 59
Survey measures
Participants self-reported demographic information, including age, ethnicity, employment, education, household income, health insurance, sexual orientation, relationship status, and primary mode of transportation. Relationship status was self-reported and categorized broadly (e.g., in a relationship vs not in a relationship); additional details regarding relationship stability, or partner characteristics were not collected. Among those who reported being in a relationship, they also self-reported their relationship type and length. Participants also completed a 3-item discrimination subscale from the Group Based Medical Mistrust Scale (GBMMS),60–62 which assessed perceived racial bias in health care (e.g., “Black people are treated the same as people of other groups by doctors and health care workers”) 61 using a 5-point Likert scale (5 = Strongly Agree to 1 = Strongly Disagree) (Cronbach’s α = .91). Sexual behaviors associated with HIV exposure that may increase vulnerability to acquiring HIV were also captured (i.e., condomless vaginal or anal sex, HIV and STI testing frequency, injection drug use; sex exchange). 14 All participants were provided a definition of PrEP, and information about PrEP efficacy, effectiveness, modality, and the general process used to obtain PrEP, prior to answering any PrEP-related questions. PrEP-related measures included prior awareness (dichotomous: yes/no), interest in learning about PrEP (5-point Likert scale: 1 = Not at all interested, 5 = Extremely interested), comfort discussing PrEP with a provider (5-point Likert scale: 1 = Very comfortable, 5 = Very uncomfortable), and intentions to talk to a provider about PrEP and obtain a PrEP prescription within the next 6 months (4-point Likert scale: 1 = I definitely will not do, 4 = I definitely will do).
Choice-based conjoint task
The CBC task was designed using Sawtooth Software, SSI Web 8.2, to ascertain preferences for PrEP program attributes. Attributes (and their levels) were selected based on the literature16,17,20,22,35,63 and findings from qualitative focus groups using nominal group technique (NGT). 64
The NGT is a consensus method 65 ideal for generating quantitative rankings (real-time consensus scoring) while also collecting in-depth qualitative information within a short timeframe. NGT is commonly used in complex decision-making scenarios65–68 and is adaptable across different settings and methodologies.66,69 Unlike traditional focus groups, NGT ensures equal participation, fosters group discussion, and reduces researcher bias by limiting dominant voices in the conversation. 67 NGT sessions were conducted in two online focus groups with adult BW without HIV (n = 14) to identify and prioritize key barriers and facilitators (identified from the literature review) influencing BW’s potential PrEP use. Participants ranked 16 barriers and 16 facilitators related to PrEP, by importance 1–16, followed by a group discussion to review rankings, clarify reasons, and consolidate options. Findings identified BW’s top ranked concerns about PrEP: (1) side effects; (2) potential interactions with other medications; and (3) lack of health insurance coverage for PrEP. 64 Key factors influencing BW’s potential PrEP use included the following: (1) discussing PrEP with a doctor of the same race; (2) discussing PrEP with a doctor of the same gender; and (3) receiving regular text or email reminders to take PrEP. 64 Group discussions highlighted key concerns regarding PrEP use: potential side effects, interactions with other medications, and PrEP accessibility, particularly health insurance coverage. 64 Participants emphasized the importance of having race- and gender-concordant providers, which significantly influenced their consideration of PrEP; and for targeted community outreach and culturally relevant advertising to increase PrEP appeal among BW. 64 Findings from the NGT, in addition to findings from prior published literature, were then used to assist in the identification and description of the PrEP program attributes (and their levels) used for parent study.
Before the study began, the CBC task was piloted with 8 BW to obtain their feedback about whether they perceived the attribute levels to be understandable, relevant, and logical when combined to create a PrEP program. Women provided feedback on wording, clarity of instructions, and survey length. Their feedback led us to make minor modifications to the content (e.g., word choice used to describe the attributes and their levels) and format (e.g., presentation of PrEP information, exclusion of pictures/images) of the CBC task before starting study recruitment.
The final CBC instrument covered six modifiable attributes of a potential PrEP program (and associated levels): (1) administration method (daily pill, bimonthly shot, monthly vaginal ring), (2) access location (doctor’s office, community clinic, pharmacy, telehealth (with mailed meds)), (3) healthcare integration (family planning, women’s health checkups, STI care), (4) provider demographics (any provider, same race, same gender, or both), (5) payment method (one-time fee, income based, cost assistance), and (6) support services (text support, online group, help disclosing PrEP to partner) (Table 1). LAI PrEP requires in-person administration; as such, for the current study, telehealth supports screening, counseling, prescribing, and follow-up only.
Description of choice-based conjoint attribute categories and associated levels for PrEP programming.
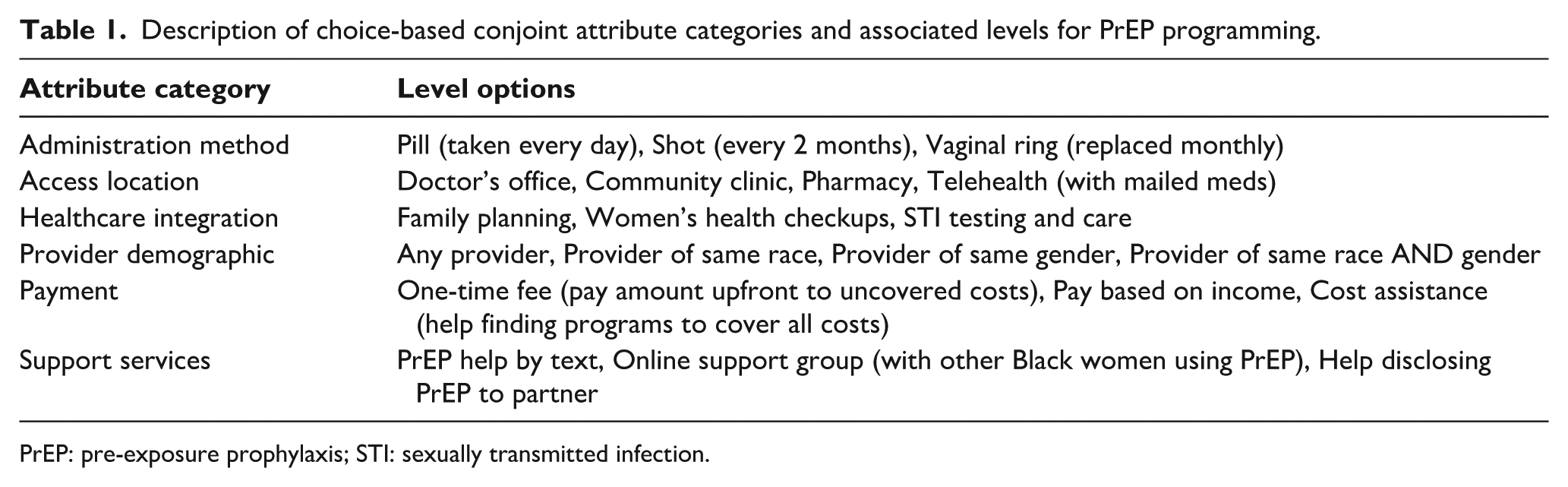
PrEP: pre-exposure prophylaxis; STI: sexually transmitted infection.
Preferences for PrEP program attributes were solicited through 14 choice tasks presenting experimentally varied combinations of the study’s attribute levels. Participants were asked to select their preferred option among two possible PrEP programs, displaying the 6 attributes and select levels. A “None” option was included to allow participants to opt out of a proposed program (see Figure 2) such that respondents could indicate that they would not select any of the presented PrEP programs in a choice task. This is commonly included in market simulations to estimate this portion of the sample. Sawtooth Software’s experimental design module generated 450 different versions of the survey according to three principles: (1) each attribute level appeared only once per task; (2) levels appeared equally often across tasks; and (3) levels were chosen independently of each other. Utility scores from these tasks were then used to predict preference shares for hypothetical PrEP programs.

Example of computerized participant view of choice-based conjoint task survey.
For the parent study, the target sample size was calculated using the standard formula for estimating a proportion:

where

where

Thus, we projected needing a sample size of ~400 participants to provide adequate power for both the survey analysis and the CBC attribute-level analyses, and to account for potential incomplete survey responses.
Statistical analyses
Conjoint and latent class analysis
All CBC analyses were conducted using Sawtooth Lighthouse Studio 9.16.10, using the Hierarchical Bayes model to estimate part-worth utilities (PWUs) for 20 attribute levels to evaluate respondents’ prioritization of importance between attributes and their associated levels. PWU is the value respondents attach to a specific level of a particular attribute. These PWUs are zero-centered, with larger absolute values indicating stronger positive or negative preferences relative to other levels of the same attribute. Mean relative importance scores (RIS) were rescaled to 100 to reflect how much each attribute influenced decision-making (e.g., a RIS of 27% implies that the attribute drives 27% of a participant’s preference). Latent class multinomial logit analysis then grouped respondents based only on their PWUs (not considering responses to demographic and other characteristic questions), identifying segments with similar preferences. The segment group solution (N = 3 groups) was chosen based on the Akaike information criterion (AIC), consistent AIC, Bayesian information criterion (BIC), and adjusted BIC.
Demographics
Utilities were entered into the SAS software (version 8.2, Cary, NC, USA) and merged with the respondents’ demographics and characteristics. We used RStudio (2022.02.0 Build 443, Boston, MA, USA) to conduct descriptive statistics for sample demographics and characteristics, by segmentation group. Independent variables were summarized overall and by segment group; means, standard deviations, frequencies and percentages are provided, where applicable. A comparison between groups was made with respect to the respondents’ characteristics and demographics, using Pearson’s chi-squared or Fisher’s exact tests with p-values <0.05 considered statistically significant.
Results
Of the 390 BW enrolled in the parent study, 83 were aging BW (mean age = 51.8 years, SD = 6.20) who are the focus of this secondary analysis (Table 2). Most identified as non-Hispanic (n = 82, 98.9%), heterosexual (n = 78, 94.0%), had at least a bachelor’s degree (n = 44, 53.0%), were employed (n = 64, 77.1%), had a household annual income between $35k–$99k USD (n = 40, 48.2%), and were universally insured (i.e., had health insurance, primary care provider and a family planning provider). Most used a car as their primary mode of transportation (n = 78, 94.0%), were in a relationship (n = 62, 74.7%), and had high levels of perceived discrimination and group-based disparities in health care (M = 3.94).
Demographic characteristics of the sample, stratified by segmentation group identified from latent class analysis.

PrEP: pre-exposure prophylaxis; STI: sexually transmitted infection.
Perceived discrimination and group disparities in health care: 5-point Likert scale from 1 = Strongly Disagree to 5 = Strongly Agree.
Worry about acquiring HIV: 5-point Likert scale from 1 = Not at all to 5 = A lot.
Interest in learning about PrEP: 5-point Likert scale from 1 = Not at all interested to 5 = Extremely interested.
Comfort discussing PrEP with a provider: 5-point Likert scale: 1 = Very comfortable, 5 = Very uncomfortable.
Intentions to talk to a provider about PrEP: 4-point Likert scale from 1 = I definitely will not do, 4 = I definitely will do.
Intention to obtain a PrEP prescription within the next 6 months: 4-point Likert scale from 1 = I definitely will not do, 4 = I definitely will do.
p < .05. **p < .01. ***p < .001.
Increased HIV vulnerability was reflected in reported behaviors: 94.0% (n = 78) engaged in condomless vaginal sex in the past 6 months, 63.9% had not tested for HIV in that period (n = 53), and 65.1% had not tested for STIs (n = 54). Approximately half had heard of PrEP (n = 41, 49.4%). Participants reported moderate interest in learning more about PrEP (M = 2.80), were comfortable discussing PrEP with a provider (M = 2.01), had somewhat high intentions to talk to a provider about PrEP (M = 2.37), but were unlikely to obtain a PrEP prescription (M = 2.14). Scale anchors for each measure are provided in Table 2. Differences in mean values should be interpreted within the context of each scale rather than compared directly across constructs.
Relative Importance Scores and Part Worth Utilities
Attribute importance estimates for the full sample and the subsample are presented in Table 3. Zero-centered part-worth utility estimates for full sample, subsample, and each segmentation group are shown in Table 4. Based on latent class analysis, a three-segment solution was identified as the best-fitting model for the subsample (N = 83). Model fit indices for one- to five-class solutions are summarized in Table 5. For the selected three-class solution, fit statistics included AIC = 1716.73, CAIC = 2011.66, BIC = 1964.66, and adjusted BIC = 1815.36, with a log-likelihood of −811.36. Classification quality was high, as indicated by an average maximum posterior membership probability of 0.997, although overall percent certainty was modest (42.24%). Model fit statistics included a χ2 value of 1186.77 and a relative χ2 of 25.25.
Attribute importance, by segmentation group; compared with the full sample from the parent study.

Bold represents the top 3 important attributes for each group.
Part worth utility scores (zero-centered values) across each segmentation group; compared with the full sample.

PrEP: pre-exposure prophylaxis; STI: sexually transmitted infection.
Interpretation: negative values imply negative preferences for the program attribute and the magnitude of the preference is associated with the strength.
PrEP: pre-exposure prophylaxis.
Italics represent the most preferred item within each attribute.
Summary of best replications from latent class analysis (N = 83).

Pct Cert: percent certainty; AIC: Akaike information criterion; CAIC: Consistent Akaike information criterion; BIC: Bayesian information criterion; ABIC: sample-size-adjusted Bayesian information criterion.
PrEP administration method was the top-ranked attribute (39%), with a preference for LAI PrEP over the daily oral PrEP pill and the vaginal ring (Table 3). Provider demographics ranked second (14%), with a stronger preference for gender-matched providers over race-matching. Payment options ranked third (13%), with preferences split between a one-time fee and cost assistance.
Findings from the latent class analysis identified three distinct groups (Table 4). Group 1 (n = 8) (Unaware but open) included more women under age 55, reported relatively greater worry of acquiring HIV, and were unaware of PrEP before the study. After learning about PrEP, women in this group reported high interest and comfort discussing PrEP with a provider and moderate intentions to use it. They preferred a daily pill from a doctor’s office with cost assistance. Group 2 (n = 35) (Women who could benefit from PrEP, but disengaged) had more women with an annual household income over US$100k, reported a higher prevalence of behaviors associated with HIV exposure and lower perceived worry about acquiring HIV. Despite being comfortable discussing PrEP with a provider, they were the least interested in learning more about PrEP. Women in this group strongly favored LAI PrEP but were also open to the daily pill. They preferred telehealth-supported (in-person) delivery from a provider of the same gender and a one-time payment. Despite these preferences, many participants in this group chose “none” in the conjoint tasks and thus would likely decline PrEP if it were offered to them. Group 3 (n = 40) (Proactive and interested) included more women over age 50, single, and recently tested for HIV/STIs. They reported the strongest interest and intention to use PrEP, preferring LAI PrEP from a pharmacy, with cost assistance and a pharmacist of the same race.
Compared with the full sample (N = 390), aging women still valued the PrEP administration method (i.e., pill (taken every day), shot (every 2 months), vaginal ring (replaced monthly)), though slightly less (48% vs 39%), with the vaginal ring strongly disliked across all groups. While the full sample preferred providers who matched both race and gender, aging women prioritized gender matching alone. Access location ranked third in the full sample (N = 390), but was replaced by payment options among aging women. The full sample also showed a more defined ranking of the secondary attributes (with PrEP administration as the dominant factor), but aging women gave them all roughly equal importance.
Discussion
This article reports findings from a secondary analysis of a subgroup of BW aged ⩾45 from a broader online DCE (parent study, N = 390; June–August 2024); one of the few studies to examine preferences for key features of PrEP delivery among aging BW in the US South, a population that is disproportionately affected by HIV and often overlooked in the literature. The purpose of this analysis was to identify the most influential attributes of PrEP programming among aging BW, aged ⩾45, and how these preferences can better inform program design. Descriptive comparisons with the full sample showed that differences in PrEP preferences: Aging BW weighed secondary program attributes more evenly, prioritized gender over racial concordance in providers, and placed greater emphasis on payment structure. The segmentation analysis revealed diverse preference patterns among aging BW, which descriptively varied by levels of PrEP awareness, perceived HIV vulnerability, and behavioral intentions. The finding that key subgroups favor pharmacist and telehealth-delivered LAI PrEP highlights a concrete, yet underexplored, opportunity for program design tailored to aging BW.
The PrEP administration method was the most influential factor in PrEP decision-making among this sample of aging BW, with a strong preference for injectable PrEP. Consistent with Elopre et al., 50 injectable PrEP was highly valued among BW in their sample; however, our findings among aging BW suggest a more multidimensional decision-making process in which provider characteristics and cost considerations play a comparatively larger role than modality alone. Similarly, Knight et al. 52 found that age played a significant role in women’s preferred PrEP modality such that BW aged 30–44 preferred injectable PrEP while BW aged 18–29 preferred oral PrEP. LAI PrEP has also shown appeal among subsets of BW facing social and structural barriers, such as cost or stigma.29,50,51,70 These findings suggest that offering diverse long-acting options for HIV prevention may be beneficial for aging BW. Notably, among aging BW, PrEP administration remained important but was less dominant than in the full sample, suggesting a more holistic decision-making process that also weighed provider characteristics and costs. As such, uptake and persistence in this group may depend on the overall clinical care experience. PrEP implementation efforts should include multi-component strategies, and information about PrEP should emphasize the complete package, not just the efficacy or convenience of LAI PrEP.
Provider demographics also shaped PrEP preferences, demonstrating the significance of the patient–provider relationship to the decision to choose PrEP among aging BW. Findings indicate that aging BW prioritized gender matching alone, whereas BW in the parent study preferred providers who matched both gender and race. Prior research shows that provider characteristics influence BW’s decisions about PrEP.71,72 For instance, some BW seek care from providers of the same gender and/or race to mitigate anticipated or past healthcare discrimination, while others value such congruence for greater relatability and cultural humility from their provider.73,74 For aging BW, gender aligned care may be needed to build trust and comfort in discussing PrEP or other sexual health needs with a provider. These findings suggest that tailoring PrEP interventions to consider provider demographics, particularly gender congruence for aging BW, may enhance patient–provider rapport and improve PrEP uptake within this population.
Payment method was the third most influential factor, underscoring the role of affordability in PrEP uptake. In this study, interest in PrEP shaped preferred payment methods: BW less interested in PrEP favored a one-time fee while those more interested in PrEP preferred cost assistance. For many BW, disproportionate financial burdens make PrEP cost a barrier to initiation.23,51,75,76 Even when there is interest in PrEP and comfort with providers, financial constraints alone can deter PrEP use.23,51 In this sample, the group most interested in PrEP (Group 3) had a higher proportion of aging BW with household incomes below $35,000 and without health insurance. Consistent with prior research, out-of-pocket costs and lack of insurance are major deterrents to PrEP uptake in marginalized communities.75,77,78 Offering flexible payment options and expanding access to financial support programs, like PrEP assistance programs,79,80 could help address these barriers. Clear communication about available financial support and insurance navigation support is essential to empower BW to make informed PrEP decisions. Because payment preferences varied by PrEP interest level, outreach should reflect these differences. For those less interested, a one-time, low-hassle payment option may reduce complexity and resistance. For those more interested, emphasizing ongoing cost assistance could support continued engagement. Tailoring payment messaging in this way may address financial concerns, enhance feasibility, and improve uptake and persistence among aging BW.
Addressing financial barriers is only part of the solution; delivery models must also align with aging BW’s preferences and logistical needs. The preference among some aging BW for LAI PrEP delivered through pharmacies or via telehealth-supported models highlights an important opportunity for service innovation. Pharmacist-led and hybrid telehealth models could expand access by combining remote prescribing and follow-up with in-person administration at convenient, community-based sites. Such approaches may reduce logistical barriers, increase privacy, and leverage trusted access points for aging BW. Demonstration projects are needed to evaluate the feasibility, acceptability, and cost-effectiveness of these delivery models, as well as their potential to improve uptake and persistence in this population.
Findings also revealed substantial variability in preferences across the three latent groups, indicating that PrEP interest and delivery priorities among aging BW are not uniform. While LAI PrEP was generally preferred, PrEP modality, payment method, and provider demographics influenced PrEP acceptability in different ways. Group 1 preferred daily oral PrEP, cost assistance, and a race-congruent provider. Group 2 favored injectable PrEP combined with a one-time payment method and gender-concordant providers. Group 3 prioritized injectable PrEP coupled with cost assistance and a race-congruent provider. These differences emphasize the need for PrEP programs tailored not only to preferred administration methods but also to the complex interplay of these secondary PrEP program attributes. Additionally, the inverse scores for willingness to use PrEP suggest that even highly favorable program formats may not overcome possible perceived or anticipated discrimination, HIV vulnerability misperception, or structural barriers unless coupled with targeted educational and behavioral interventions that are age- and context-specific.
One important pattern observed in this study was a discrepancy between reported sexual behaviors commonly associated with HIV exposure and participants’ perceived concern about acquiring HIV. For instance, within the “Women who could benefit from PrEP, but disengaged” group, despite engaging in behaviors associated with elevated HIV vulnerability, women in this segment reported low worry about acquiring HIV and limited interest in PrEP. One reason for this misalignment could be due to socioeconomic status, such that belonging to a higher income bracket and being in an “upper echelon” segment of society sometimes carry an heir of invincibility that is linked to feeling insulated and protected. 81 On the other hand, Life Course Theory suggests that this misalignment may be influenced by accumulated life experiences, social roles, and transitions that shape risk interpretation and health prioritization among BW over time.82–84 Specifically, these developmental and social factors operate across the lifespan, influencing how HIV “risk” is understood and prioritized in the context of competing demands and cultural expectations. Thus, the resulting cognitive dissonance (between actual behaviors and acknowledged risk) may manifest as dismissal or the minimization of vulnerability, especially when such behaviors are discreet and culturally coded as “lady like” or private. 84 This misalignment underscores the need for communication strategies that bridge the gap between objective risk and personal risk perception. Messaging should draw on lived experiences and situational contexts relevant to aging BW, framing HIV prevention as an affirming, empowering health choice rather than solely a response to “risk.” Non-stigmatizing approaches that emphasize autonomy, discretion, wellness, and the role of PrEP in maintaining long-term sexual health may be particularly effective in increasing receptivity among this group.
Ultimately, these findings show that successful PrEP programs for aging BW should prioritize diverse PrEP modalities, gender congruent providers, and accessible payment options to improve equity in PrEP access and potential use among aging BW. PrEP programs targeting aging women will need to be tailored using direct input from this population, and aim to balance multiple factors rather than emphasizing one dominant feature (i.e., a one-size-fits-all approach), which may be less effective 85 and off putting.
Implications for clinical practice and public health
These findings have important clinical implications. First, with only half of participants having previously heard of PrEP, continued PrEP education is necessary to raise awareness of this biomedical prevention strategy and its suitability for BW. Low awareness remains a barrier to PrEP initiation, underscoring the importance of proactive outreach. Aging BW commonly obtain health information from multiple sources, including healthcare providers, family and social networks, community organizations, and media. 86 Trusted interpersonal relationships also serve as primary channels for knowledge dissemination,87,88 making social networks crucial for spreading awareness, with accuracy, about PrEP and sexual health. Understanding these information pathways is essential to tailor PrEP outreach and education for maximum impact. Relatedly, it is important for aging BW to know about PrEP because they may occupy central caregiving roles within their families and communities, including educating their children, grandchildren, and other younger people in their care and/or community. As trusted sources of knowledge and guidance, aging BW can help normalize conversations about HIV prevention and PrEP use, dispelling stigma and misinformation. Moreover, by understanding PrEP themselves, they can act as advocates and educators, extending prevention knowledge beyond clinical settings into social and familial networks where PrEP awareness may otherwise be limited. This ripple effect can enhance intergenerational dialogue about sexual health and reinforce protective behaviors among younger community members.
Second, there is a need to include BW across the lifespan within HIV-focused research studies. In the current study, the age range of participants was 45–71 years, including 21 participants aged 55 and older, and 3 participants that were over the age of 65. The United States Preventive Services Task Force (USPSTF) currently recommends routine HIV screening for adolescents and adults aged 15–65 years, with screening for those over the age of 65 advised only if they are at increased risk of infection. 89 As such, not having undergone HIV screening beyond age 65 may not be considered a risk behavior per standard clinical practice. Moreover, it is important to recognize that sexual activity continues into older age for many women, and risk factors for HIV may still be present. Future research should therefore prioritize including samples of aging Black women over 65 years of age to better understand their HIV prevention needs. This should be inclusive of PrEP eligibility, awareness, and use; and to inform age-appropriate screening and prevention guidelines that reflect the realities of aging adults’ sexual health.
Third, providers must counteract ageist and stigmatizing assumptions that aging women are not vulnerable to acquiring HIV and address related misinformation. Routine sexual health and HIV vulnerability assessments for aging patients should be normalized to reinforce that age alone is not protective. Also, differences in vulnerabilities, barriers, and needs across subgroups require flexible, patient-centered approaches rather than one-size-fits-all strategies. Program models that provide decision-support tools to guide personalized PrEP choices 85 for aging BW could improve their access and use of PrEP. Finally, PrEP should not pose a financial burden. Patients should receive clear information on costs of their preferred PrEP modality and be offered financial assistance to cover PrEP-associated costs (PrEP medication, HIV/STI testing, etc.).
Limitations
This study does have limitations. First, the latent class analysis was conducted in a relatively small subsample, BW aged ⩾45 living in the southern United States, which may limit class stability and generalizability. As such, identified segments should be interpreted as exploratory and hypothesis-generating rather than as definitive. Larger samples are needed to confirm segment structure and stability. Due to the small sample size, these findings may restrict the transferability to other women outside of these demographics. The accuracy of reported self-behaviors about HIV vulnerability and PrEP-related attitudes could have been affected by social desirability bias. To migrate this bias, anonymous surveys and culturally informed data collection methods were used. The current study also did not capture data on the efficacy of PrEP for people older than 60 with comorbid conditions like kidney disease. Since a side effect of taking PrEP does impact kidney function, capturing this information could have been useful for PrEP recommendations among women in this age range. Overall, due to the consistent underrepresentation of aging BW in HIV and aging literature, prioritizing this population helps address a major gap in the research. Additionally, relationship status was assessed using a broad self-report measure, and the study did not collect detailed information on relationship contexts or partner-level characteristics that may further contextualize HIV vulnerability and PrEP decision-making.
Conclusions
PrEP program preferences are not uniform among aging BW. Factors such as administration methods, provider demographics, and payment options varied across subgroups. By using CBC analysis, a type of DCE, we were able to quantify which features matter most to different groups of aging BW. While injectable PrEP was generally favored, variation existed in how women prioritized different attributes. Rather than assuming a single PrEP delivery model that will meet all needs, programs can be tailored to align with specific preferences – especially for aging women, who weigh multiple factors more evenly and may require more personalized support in decision-making. CBC offers a valuable tool to design more responsive, equitable, and user-centered PrEP programs for BW across the life course.
Footnotes
Acknowledgements
We would like to acknowledge and thank the following organizations for their amazing contributions to the recruitment efforts for this study: Health and Wellness Education Center – Alabama; Five Horizons Health Services; Selma AIR – Alabama; Alabama Department of Health; AIDS Healthcare Foundation – Communication Department; The Well Project; Texas D-CFAR; Florida International University- Research Center for Minority Institutions (RCMI) Community Advisory Board; Black Women’s Health Imperative; Houston Area Women’s Center (HAWC) Houston; and Healthy Start Coalition of Miami Dade. We would also like to thank the participants for their important contributions toward this work.
ORCID iDs
Ethical considerations
The study was approved by the Florida International University Institutional Review Board (IRB-23-0283-AM01) and the University of Texas Health Science Center San Antonio (STUDY00001802).
Consent to participate
Electronic informed consent was obtained from all individual participants included in the study.
Consent for publication
Electronic informed consent for publication was obtained by all individual participants included in the study.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Number U54MD012393, Florida International University Research Center in Minority Institutions. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.