
Abstract
Background:
Black cisgender women in the United States experience a disproportionate burden of human immunodeficiency virus acquisition. Pre-exposure prophylaxis is an effective oral daily medication that reduces the risk of human immunodeficiency virus through sex by 99% when taken as prescribed. However, less than 2% of eligible Black cisgender women take pre-exposure prophylaxis. The purpose of this scoping review was to describe the types of research studies done in this area, gaps in knowledge, and potential areas of research needed to increase pre-exposure prophylaxis use among Black cisgender women in the United States.
Methods:
We conducted our search in MEDLINE (PubMed), Embase (Elsevier), CINAHL (EBSCOhost), PsycINFO (EBSCOhost), and Scopus (Elsevier) using a combination of keywords and database-specific subject headings for the following concepts: pre-exposure prophylaxis, African American/Black or minority, and women. We used the Joanna Briggs Institute’s Reviewers’ Manual process for Scoping Reviews and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews to ensure comprehensive and standardized reporting of each part of the review.
Results:
Fifty-nine studies were included in the final review. Results of the study were classified according to the three phases of the Human Immunodeficiency Virus Prevention Cascade—demand side, supply side, and adherence and retention. The majority of studies (n = 24, 41%) were cross-sectional quantitative surveys and 43 (34%) focused on the demand-side phase of the Human Immunodeficiency Virus Prevention Cascade. Fifty-eight percent of studies either assessed women’s pre-exposure prophylaxis knowledge, attitudes, and intentions to use, or assessed perceived barriers and facilitators. Seven studies (12%) tested pre-exposure prophylaxis uptake and adherence among Black cisgender women.
Conclusion:
This review found multiple missed opportunities to increase women’s demand for pre-exposure prophylaxis and health care provider screening and referral for pre-exposure prophylaxis. Additional studies are needed to effectively assess pre-exposure prophylaxis uptake and adherence among Black cisgender women.
Introduction
The incidence of human immunodeficiency virus (HIV) in the United States has trended down over the past decade, 1 yet Black cisgender women in the United States continue to experience a disproportionate burden of HIV acquisition. 2 In 2019, Black women, who make up 13% of the US female population, 3 accounted for 58% of new infections among women. 4 In 2019, the rate of Black women living with HIV (WLWH) was 17.4 times higher than White women. 5 The majority of new diagnoses among Black women are due to heterosexual transmission (85%), 6 emphasizing the need for more HIV prevention options that are not solely male-centric. Furthermore, Black women have the highest rates of sexually transmitted infections (STIs) 7 and experience intersectional stigmas 6 that impede their engagement in the HIV Status Neutral Treatment and Prevention Cycle. 8
Several factors contribute to the epidemic among Black cisgender women, including structural (e.g. higher rates of poverty, a lack of access to health care, and residential segregation), 9 social (e.g. HIV-related stigma, broad cultural values and belief systems about gender roles, social norms, and attitudes toward safer sex practices), 10 interpersonal (e.g. relationship power dynamics, domestic and sexual abuse, intimate partner violence, patient–provider relationships, and social networks), 11 and personal factors (e.g. higher rates of some STIs, smaller sexual networks, and a lack of awareness of HIV status), 2 emphasizing the need for more focused, innovative, and strengthened efforts to address this disparity. Black cisgender women’s vulnerability to HIV reflects a complexity of experiences based on intersecting systems of oppression. 8 For example, due to racially discriminatory housing policies, there is a subgroup of Black women who are more likely to live in segregated neighborhoods with fewer health resources, fewer employment and educational opportunities, and higher rates of poverty. All of these factors can affect access to HIV care and prevention while also increasing HIV risk. 12 Racialized criminal justice policies disproportionately place Black people in correctional facilities with higher rates of HIV transmission, ultimately affecting Black women’s social networks and potential HIV exposure. 13 Intimate partner violence, which impacts women’s ability to negotiate sexual relationships, is often higher among women with fewer economic or educational resources and therefore can increase the risk of HIV for Black cisgender women. 11
Tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) pre-exposure prophylaxis (PrEP), the only effective oral daily medication approved by the US Food and Drug Administration for women, reduces the risk of HIV through sex by 99% when taken as prescribed. 14 Both the Centers for Disease Control and Prevention (CDC) and the American College of Obstetricians and Gynecologists 15 (ACOG) issued clinical practice guidelines for PrEP use among women, including women who have partners living with HIV, women who are sexually active in areas with high HIV prevalence, and women who use condoms infrequently with male partners. Estimates suggest that in 2015, nearly half a million heterosexually active women aged 18 to 59 were eligible for PrEP, meaning they are objectively at high risk of HIV infection. 16 Yet, in the United States, PrEP is prescribed to just 2% of the ~468,000 women who could benefit from it. 16 Black women represent 26% of female PrEP users while constituting 58% of new HIV infections among women.6,16 As such, Black cisgender women vulnerable to heterosexual HIV acquisition have not significantly benefited from PrEP, which may be partially responsible for recent reductions in new HIV infections among gay, bisexual, and other men who have sex with men (MSM).
The purpose of this scoping review was to (1) describe characteristics (e.g. study design, focus) of studies that have focused on PrEP and Black cisgender women in the United States, (2) categorize the major findings of those studies, (3) identify gaps in research needed to enhance HIV prevention efforts for Black cisgender women in the United States, and (4) define future directions for research in this area.
Methods
This scoping review was conducted using the Joanna Briggs Institute’s Reviewers’ Manual process for Scoping Reviews. 17 The process is an extension of that developed by Levac et al. 18 The review process is comprised of the following components: (1) identifying and aligning research questions and objectives; (2) identifying relevant studies by developing inclusion and exclusion criteria that align with research questions; (3) searching, selecting, and extracting studies to be used for the review; (4) charting the data; and (5) collating, summarizing, and reporting findings in alignment with the objectives and research questions. In addition, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist was used to ensure comprehensive and standardized reporting of each part of the review. 19 The present article includes all strategies used to complete the scoping review. The present review was not registered with PROSPERO or similar reporting system as it was not mandatory to do so.
Search strategy
A pilot search of MEDLINE (PubMed) was conducted by a research librarian. The team screened an initial 50 of the search results to ensure the search identified relevant studies and to develop and refine the inclusion and exclusion criteria. The initial search strategy was then refined and approved by the team. The librarian constructed and translated the search in MEDLINE (PubMed), Embase (Elsevier), CINAHL (EBSCOhost), PsycINFO (EBSCOhost), and Scopus (Elsevier) using a combination of keywords and database-specific subject headings for the following concepts: PrEP, African American/Black or minority, and women. The date range for this review was unlimited. Editorials, letters, and comments were excluded. To improve specificity, animal-only studies were excluded. The full, reproducible search strategies for all included databases can be found in the Supplemental Appendix. Additional references were identified by hand-searching bibliographies of included articles.
Identifying and selecting relevant studies
All citations were imported into Covidence, a systematic review screening software (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org); Covidence detected 596 duplicates. The searches yielded a total of 927 citations after removal of duplicates. Covidence was also used to complete dual independent title/abstract and full-text review of articles retrieved from the search. For the initial 30 articles, six research team members met to review the title and abstract screening decisions to train the screeners and help ensure inter-screener agreement. After the initial screening of 30 titles and abstracts, two reviewers independently determined each study’s relevance based on the exclusion and inclusion criteria at both the title/abstract and full-text phases. Any conflicts were resolved through team discussion. Inclusion criteria were primary studies focused on PrEP, HIV, and Black women; majority Black women in the study population; conducted with human subjects; published in English; gray literature, including conference abstracts; and participants who were adult (18 years and older) Black cisgender women in the United States. Exclusion criteria were systematic reviews and literature reviews; commentaries, guidelines, protocols, and letters to editors; laboratory (e.g. in vitro) or pre-clinical studies (e.g. animal studies); research studies estimating drug efficacy and/or drug resistance for people with HIV; and studies focused on PrEP to prevent diseases other than HIV (e.g. other STIs). Criteria were based on the research team’s previous experience and publications on HIV8,20 and a recent scoping review on HIV interventions. 21
Data extraction and charting the data
Data extraction was completed by six reviewers using Covidence’s 2.0 data extraction tool that was modified to suit the study’s criteria. Information extracted from studies included study author, year of publication, title, journal, study purpose, study population, percent Black women, study design, results, significant findings, key words, implications, discussions related to racism and social determinants of health, and suggestions for future studies. Social determinants of health included factors related to or resulting from poverty, discrimination, gender inequity, and racism (inequities based on the oppression of a racial group).2,10 Six reviewers piloted the data extraction form by reviewing and extracting data from a random sample of 15% of the full-text articles to ensure the form captured relevant information. The remaining articles were extracted by two independent reviewers. All conflicts were resolved through discussion with at least two team members. All studies included for the review were stored, managed, and organized in EndNote bibliographic software.
Mapping study topics and analysis
Findings were analyzed and grouped by thematic content analysis, and findings were collated and reported using quantitative and qualitative methods. Thematic content analysis was used to identify patterns in knowledge and findings from studies based on codes developed from keywords abstracted from studies. A total of six themes were developed. Descriptive statistics like frequencies were used to quantify certain types of research designs and studies including racism and social determinants of health in the discussion, as well as to classify categories of findings across studies. The summary of this review’s findings will ultimately clarify what is known about PrEP uptake in Black women and define future directions for research.
Framework
The HIV Prevention Cascade was the framework used to guide categorization of the studies included in this review according to study focus, study results, and gaps in research. 22 The three phases of the Prevention Cascade are demand side, supply side, and adherence and retention (Figure 1). 22 The demand-side phase focuses on programs, interventions, and policies that spread awareness and increase community knowledge about PrEP. Increased knowledge and awareness can improve vulnerable populations’ interest in and willingness to use PrEP. The supply-side phase focuses on enhancing access to PrEP through increased screening, referrals, and availability of locations to receive PrEP. The last phase—adherence and retention—looks at how successful people are at taking their medication as prescribed, for as long as they are at risk for HIV.

HIV Prevention Cascade.
The HIV Prevention Cascade was chosen to frame the results of this review for two reasons. First, it lays out the steps of HIV prevention from awareness to adherence and can therefore clearly illustrate where there are gaps in knowledge and opportunities for research. Second, it is built on the socioecological approach to health which considers individual- and societal-level factors that affect HIV risk. 23 Therefore, each phase of the Cascade allows for the consideration of multilevel facilitators and barriers—including social and structural barriers such as stigma, poverty, and racism—which disproportionately affect Black women and their HIV risk.
Results
The initial search yielded a total of 1517 articles, of which 596 duplicates were excluded. The title and abstract of 921 articles were screened for relevance and 624 were excluded. After full-text review, an additional 245 articles were excluded because the study population was not majority (i.e. the highest percentage of all groups included in the study) Black cisgender women (n = 170), the study was not focused on women in the United States (n = 25), the study population was less than 18 years old (n = 22), the study was not PrEP focused (n = 13), or the study design did not meet our criteria (i.e. laboratory/pre-clinical studies, review; n = 10). Fifty-nine studies were included in the final review (Figure 2). No ethical approval was needed to utilize the existing published studies included on this review.

PRISMA diagram.
The date range for this review was unlimited, but the included study dates ranged from 2012, the year PrEP became FDA-approved and available for use, through August 2021, when the present review was completed. The number of studies published grew substantially from 2012 to 2021. In comparison to 2012 to 2015, during which five (8%) studies were published, from 2019 to 2021, 38 (64%) of the studies included in this review were published. The most frequently used study design was a cross-sectional survey design (n = 24, 41%). Cohort studies were the next most frequent (n = 10, 17%), followed by qualitative interviews or focus group studies (n = 9, 15%), and mixed methods studies (n = 7, 12%). Quasi-experimental (n = 5, 8%) and randomized controlled trials (RCTs; n = 2, 3%) were the least used study designs (Table 1).
Study characteristics, n(%).
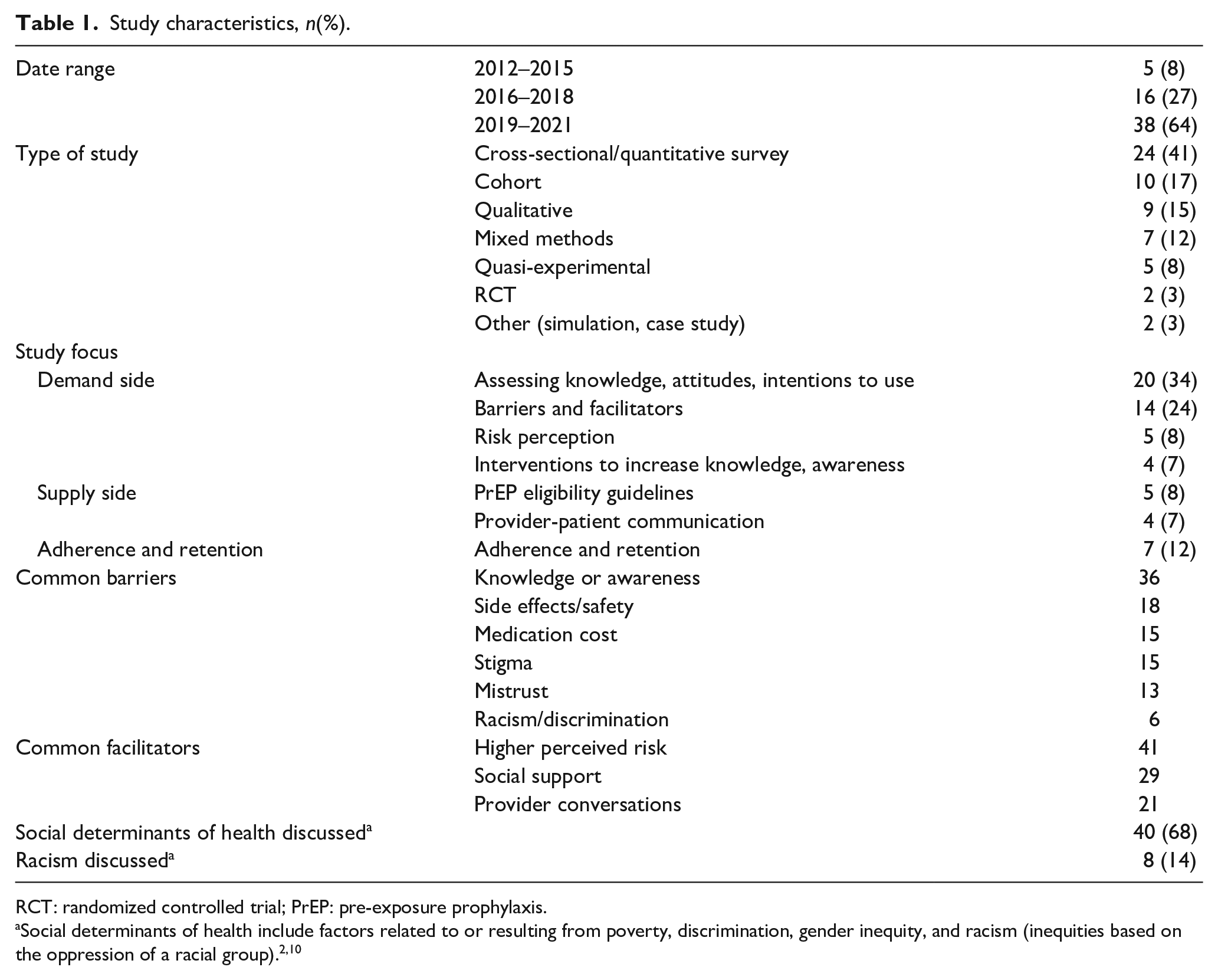
RCT: randomized controlled trial; PrEP: pre-exposure prophylaxis.
Articles and thematic findings were categorized according to the three phases of the adapted HIV Prevention Cascade—supply side, demand side, and adherence and retention. Seventy-three percent of articles (n = 43) focused on demand-side issues.9,10,11,20,24–61 The themes identified for the demand-side phase were as follows: (1) HIV risk and risk perception, (2) knowledge and attitudes toward PrEP, and (3) barriers and facilitators to PrEP use. Nine (15%) articles focused on supply-side issues.36,57,62–68 The themes identified for the supply-side phase were as follows: (4) provider–patient communication and (5) provider knowledge and referral. Finally, seven (12%) articles69–75 focused on adherence and retention. The theme for the adherence and retention phase was (6) adherence and retention.
Demand side
HIV risk and risk perception
Actual and perceived HIV risks are often discordant among Black cisgender women in the United States. Women perceived themselves as low risk, even with high-risk indicators such as having multiple sexual partners or engaging in condomless sex.51–53,55,58,74 In a survey of 109 Black women ages 18 to 45 at a family planning clinic, 67% reported recent condomless sex and 68% reported a recent STI test. However, 68% did not believe they were at risk for HIV. 45 Discordance between actual and perceived risk also occurs when women perceive themselves as low risk because they have few personal risk behaviors (e.g. only one partner), but have heightened actual risk because of population- or area-level risk factors (e.g. neighborhood or social networks with higher HIV burden).9,55 When women do perceive themselves to be at higher risk, they are more willing to use PrEP compared to women who do not perceive themselves to be at higher risk.37,43,48,59,61
Knowledge and attitudes toward PrEP
There is limited awareness and knowledge about PrEP among Black cisgender women in the United States included in the identified studies.31,34,35,38,41,42,46,53,76 Those who had friends or family members using PrEP and those at highest risk were most likely to be aware of PrEP. In two studies, women reported being aware of PrEP, but unaware it can be used for women because of significant marketing targeting MSM.31,74 Positive attitudes toward PrEP were associated with women feeling empowered to protect their health by being able to control their use of PrEP, belief in the effectiveness of the drug,40,43,48 and being younger. 42
After learning about PrEP, Black cisgender women generally had positive attitudes toward PrEP and are willing to consider using it.31,34,35,38,41,42,46,76 Women indicated that they want more outreach about PrEP.30,31 Educational interventions increased PrEP knowledge or intention to use.26,30,75 For instance, one study developed eHealth videos using avatars to educate women about PrEP. After viewing the videos, awareness of PrEP increased from 18% to 69%. 26 Moreover, a motivational interviewing intervention for 10 Black women to encourage use of PrEP led to increased knowledge and feelings of empowerment. 30 Another culturally tailored PrEP intervention increased Black women’s intention to initiate PrEP by 44% after referring women to PrEP providers. In the control arm, in which participants received educational handouts, only 37% of participants intended to initiate PrEP in the next 3 months. 75
Barriers and facilitators to PrEP use
The most common barriers that affected whether or not women wanted to initiate PrEP or adhere to a PrEP regimen once started were concerns about drug safety,30,31,41,46,49,52,53,77 cost,31,46,48,49,52,53 and low perceived risk of HIV.29,38,42,52,69,70,75 Moreover, women expressed concern about being stigmatized by family, friends, or other people in their communities if they found out they were taking an HIV prevention medication.44,52,53,74,76 Focus groups and surveys also revealed interpersonal and structural barriers to PrEP use, including sexual trauma, interpersonal and community violence, poverty, lack of child care, transportation, and homelessness.30,72,75 In addition, structural barriers were cited as a concern impacting adherence to the PrEP regimen once started.43,44,53,75 Concerns about the trustworthiness of medical systems’ and pharmaceutical companies’ intentions to help patients, as well as practical challenges of engaging with hospitals (e.g. scheduling appointments), were also cited barriers.30,33,38,71,72 Finally, some women and providers were unsure of the effectiveness of PrEP and therefore were less likely to want to take or prescribe it.25,39,44,52,69
The most often cited facilitators to women wanting to initiate PrEP or being able or willing to adhere to PrEP use were social networks and peer support.20,24,47,53,59,61,74 Women in social networks where HIV testing is more frequent were more likely to express interest in using PrEP. 47 Once taking PrEP, women were more likely to adhere to their medication regimen if their social network provided higher levels of peer support. 53 Women in relationships in which they did not know their partner’s status or were concerned about the challenge of negotiating the use of PrEP with a partner reported that the pill being a “woman-controlled” medication was a facilitator.25,26,31 Ease of use of the pills was similarly considered a facilitator, 53 in addition to the use of strategies such as pill boxes as reminders to take them daily.44,69 Provider support for and recommendation of PrEP48,53,61 was also cited as a facilitator.
Supply side
Provider–patient communication
Women are open to having conversations about sexual health and HIV prevention with their health care providers and are more likely to take PrEP when recommended by a provider.45,46,49,56,59,61 Women report perceiving some providers as being uncomfortable discussing sexual health, but that honest conversations with providers can help decrease stigma, increase trust, and increase PrEP use.36,43,48,64,66,74 In comparison to White women, Black women are significantly more likely to report intention to use PrEP if recommended by a provider. 61 However, in a study of patients in a Louisiana clinic, of the 43% of women who had heard of PrEP, the majority (77%) heard about it through the media and only 11% from their provider. 28 In another study of 2406 women, only 10% of participants had heard of PrEP and fewer than 25% discussed sexual health with their provider. However, 30% would take PrEP if recommended by their provider. 48
Provider knowledge and referral
Providers had varying levels of knowledge about PrEP use and inconsistently referred Black women for PrEP. In a cross-sectional study (N = 1404) of primarily Black women aged 18 to 25 with high-risk behaviors (e.g. multiple partners, STI diagnosis, infrequent condom use), only 2.4% were prescribed PrEP. 65 Moreover, a qualitative study examined 12 providers’ understanding and practices of prescribing PrEP. Ninety-two percent knew that PrEP is used before a potential HIV exposure, and 70% agreed that PrEP was effective and safe. However, 21.4% believed that PrEP would increase risky sexual behaviors, number of sexual partners, and rates of other STIs. 67 In addition, in a study examining a 1.5-h educational intervention to increase provider knowledge of PrEP, 66% of patients reported that their provider discussed PrEP with them following the training and 18% of patients accepted off-site PrEP referral. 57
Narrow PrEP eligibility guidelines may not accurately assess Black cisgender women’s HIV risk. Two studies examined whether current PrEP eligibility guidelines developed by the CDC and the United States Public Health Service (USPHS) Commissioned Corps accurately categorize HIV risk in Black women. Among a group of sexually active Black women (n = 566), 16% had a diagnosis of an STI but failed to report any risk factors for HIV. Thus, they were not deemed eligible for PrEP. However, the inclusion of partner characteristics in screening—such as a history of intimate partner violence or criminal justice system involvement—better differentiated STI status than the standard questions in USPHS-based guidelines. Even women reporting known HIV risk factors and motivation to take PrEP may not be considered eligible for PrEP according to the criteria set forth in CDC guidelines.51,58 However, they would be considered eligible if guidelines were expanded to include partner characteristics.
Adherence and retention
Education and targeted prevention messages help Black cisgender women address multiple barriers to PrEP adherence and retention. Seven studies37,69–71,73–75 examined Black women’s adherence to and retention of PrEP use. We included initiation of PrEP in retention. Both retention and adherence were less than expected based on women’s expressed intention. One longitudinal study of PrEP uptake showed that after referral by a provider, 7 of 30 Black women who initially expressed interest in starting PrEP followed up at PrEP clinic. 72 Another study found that after 6 months, only 18% (n = 18) of younger women continued taking PrEP for the duration of a 6-month study. 74 Reported barriers to adherence included forgetting or not being near pill boxes, uncertainty about risk, and concerns about access and medication efficacy.69,74 A study designed to address barriers utilized a 48-week text messaging intervention that incorporated significant support from study coordinators. 70 At week 48, 62% of participants (n = 121) were retained in the study while 18% were able to adhere to a six-dose per week regimen of PrEP. 70 At follow-up 3 months later, 36 of 65 women continued PrEP. Of the 26 who stopped, one-third were concerned about side effects, approximately 16% did not think they were at risk, and another 16% had no health insurance or had not seen a provider. 70 Another study showed that when primary care providers incorporated PrEP education into their practice, one-third of patients were able to adhere to a PrEP regimen. In that study, it was suggested that adherence could be improved with multiple exposures to risk messaging for women while taking the medication instead of just during the initial visit. 73
Discussion
In the United States, Black cisgender women are disproportionately affected by HIV. 8 ., 20 The purpose of this scoping review was to describe the types of research studies that have been done and major findings from those studies, as well as the gaps in knowledge and potential areas of research needed to increase PrEP use and decrease HIV transmission in this vulnerable population. Fifty-nine studies were included in this review. The majority were cross-sectional quantitative survey designs published from 2019 to 2021. Results of the study were classified according to the three phases of the HIV Prevention Cascade—demand side, supply side, and adherence and retention. Demand-side studies were over five times more common than supply-side or adherence and retention studies.
Demand side
The majority (73%) of studies on Black women and PrEP focus on understanding Black women’s knowledge of, awareness of, and interest in taking PrEP. Our review showed that while women’s risk may be high, risk perception is low. Higher risk was linked to personal factors like condomless sex, interpersonal factors like intimate partner violence, social factors like stigma, and structural factors like higher neighborhood burden of HIV and the effects of racism. Sixty-eight percent and 14% of studies discussed structural determinants of health and racism, respectively. Social determinants of health most often focused on economic vulnerability, inadequate housing, carceral systems, and intimate partner violence, which negatively impact Black women’s opportunities to protect their health.30,44,47,60 Discussions of racism outlined the importance of intersectional identities (e.g. race and sex) in increasing Black women’s HIV risk and how interventions should be tailored to the unique needs and experiences of Black women.2,10,72 However, none of the studies were designed to specifically intervene to improve factors that increase Black women’s risk for HIV. One study looked at PrEP interest among those with an arrest history and suggested expanding PrEP screening to that population to address the effects of structural determinants of health. 60 More observational and experimental studies are needed to explore how and where interventions that address racism and root causes of social and structural determinants of health might be implemented to mitigate HIV transmission among Black women.
We also found low percentages of Black cisgender women were aware of PrEP or knew what it was used for, especially if they were lower risk, older, or outside of a social network where HIV testing and PrEP use were common. Despite lack of knowledge and low-risk perception, after learning about PrEP, Black women were very willing to consider taking it. Various modes of education (e.g. eHealth and motivational interviewing) were successful at increasing knowledge of and interest in taking PrEP. However, most studies assessed knowledge, attitudes, and intention, but did not implement interventions to change knowledge, attitudes, or practices. Experimental and observational studies that introduce culturally responsive innovative interventions to increase awareness and knowledge are needed.
Even though women were willing to consider taking PrEP, they still voiced concerns that might be barriers to initiating or adhering to PrEP. The most common barriers were concerns about side effects and safety, low perceived risk, and cost. These barriers persisted even when women started taking PrEP, suggesting that education and support for women may be considered while they are on treatment and not just while they are initiating. Concerns about safety and side effects are in part connected to lack of knowledge about PrEP and may be addressed through education. However, research suggests that education around PrEP should be done in a manner that clarifies how the benefits outweigh the risks.
Furthermore, studies in this review focused on lower income and higher risk women. Health insurance status was not included in most studies, and therefore it is difficult to know whether concerns about cost were related to not having health insurance and paying out of pocket for medication, or uncertainty about whether the medication is covered with insurance. Interview and focus group studies may clarify why and for whom cost is a barrier and how that barrier might be mitigated, especially given that HIV risk is not limited to lower income women.
Finally, social networks and peer acceptance were also facilitators for PrEP use. Approaches that leverage the social interactions and networks of Black women may help overcome demand-side barriers. For instance, Black hair salons are places where Black women create and nurture social relationships and also share health-related information. 20 Interventions that leverage the social relationships in Black hair salons can potentially increase awareness, acceptability, and uptake of PrEP.
Supply side
Only 15% of studies in this review focused on supply-side issues. However, results from the literature revealed multiple opportunities to intervene in this phase of the Prevention Cascade. Black women trust providers and appreciate open and honest conversations with them about sexual health. Even if they have mistrust in the hospital system or pharmaceutical industry, they are willing to listen to providers and follow their recommendations. There are missed opportunities for providers in various settings—primary care, family planning, emergency departments, obstetric and gynecology offices—to initiate conversations and screening for PrEP use.28,43,45,57,65,67 This is especially concerning given that Black women are more likely to feel comfortable discussing PrEP with their providers and have a disproportionately high burden of HIV incidence relative to White women but are less likely to be on PrEP than White women. Providers’ discomfort discussing sex and lack of knowledge about PrEP among Black cisgender women are two primary reasons for not having these conversations. Additional studies are needed to assess providers’ decision-making process to assess what knowledge and quality improvement processes may increase their screening and comfort with prescribing.
Several studies also showed that current screening guidelines do not accurately predict HIV risk for Black women. Black women experience intimate partner violence at high rates and have social networks with higher numbers of people who have been incarcerated. Both factors increase risk of HIV, but neither is included in CDC or USPHS PrEP screening guidelines for providers. Therefore, even when providers do initiate conversations with their patients about sex, they may be underestimating the number of Black women who should be referred for PrEP use due to too narrow guidelines. One study used modeling to show the number of PrEP referrals missed by not including partner criminal justice involvement in screening and another interviewed cisgender WLWH to show how current guidelines did not adequately predict their risk. Additional studies are needed that show missed referrals due to leaving out intimate partner violence and criminal justice experience in screening. Advocating for changes to federal screening guidelines is also warranted if shown to improve referral and PrEP uptake for Black cisgender women.
Adherence and retention
The fewest number of studies (n = 7, 12%) looked at PrEP uptake or adherence. This was surprising given Black women’s high risk and high willingness to consider using PrEP. In the majority of uptake studies, less than half of women who initially expressed interest and willingness to use PrEP actually followed through by going to a PrEP clinic. After initiation, only one study showed the majority of women adhering to PrEP through the duration of the study, with significant support from study coordinators. Importantly, barriers persist even after women decide they want to take PrEP and are actively taking the medication. Thus, although women may start PrEP, continuous support and messaging reiterating HIV risk and benefits of taking PrEP would be beneficial while women are on the PrEP regimen. Women expressed concern about safety as a major barrier to both initiation and uptake. Additional studies assessing women’s experiences while on PrEP are needed to understand what side effects may be common and how women can prevent or address them.
Limitations
While the scoping review method allowed for a comprehensive assessment of the literature on PrEP use and Black cisgender women, there were several limitations. One limitation is that a study quality assessment was not included in this review. 78 However, the purpose of this review was to gain knowledge about existing PrEP promotion research studies focused on Black cisgender women in the United States and where there are opportunities for more research. The current method met the goal of this review. Future reviews that focus on answering a specific question in HIV prevention for Black women may benefit from a quality assessment. Another potential limitation is that this study focused on Black cisgender women living in the United States. While this may limit generalizability of the results, the review focused on this group because of the dearth of existing literature on HIV prevention in this population.
Conclusion
This review found many gaps in the literature and multiple places to intervene along the HIV Prevention Cascade to increase PrEP use and ultimately decrease HIV infection among Black cisgender women. First, there are multiple personal, social, and structural factors that increase Black cisgender women’s risk for HIV. More interventions are needed that increase risk perception and PrEP awareness using innovative platforms and by leveraging social networks. Studies exploring why Black cisgender women are at higher risk for HIV are needed to begin to address the social, structural, and behavioral factors that impact Black cisgender women’s HIV risk. Second, despite low-risk perception and knowledge of PrEP, Black women are willing to use PrEP. Providers should make it a practice of initiating conversations about sexual health to increase awareness and referral for PrEP use and decrease stigma. Third, Black women may not be aware that PrEP is appropriate for them because they are more likely to see men instead of women reflected in PrEP marketing campaigns. Studies that assess women’s preferences for messaging are also warranted to increase effective and targeted prevention initiatives. Finally, researchers must move beyond assessing knowledge, attitudes, and risk perception to experimental and observational studies that look at women’s uptake of and adherence to PrEP. These studies will yield much-needed data on women’s lived experiences on PrEP, specific information on how to increase Black women’s initiation of PrEP, as well as long-term retention and adherence.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Gilead Sciences, Inc.
Supplemental material
Supplemental material for this article is available online.
Ethical approval
This article utilized existing published literature and does not contain any studies with human participants or animals performed by any of the authors.