
Abstract
Background:
HIV remains a global public health concern, and women continue to be disproportionately affected. Understanding the factors associated with pre-exposure prophylaxis awareness among women is crucial as an effective HIV prevention strategy.
Objectives:
We investigated the prevalence and associated factors of pre-exposure prophylaxis awareness among women in Burkina Faso.
Design:
This was a cross-section study that used population-based data.
Methods:
A total of 17,659 women of reproductive age (15–49 years) from the 2021 Burkina Faso Demographic and Health Survey were analyzed. Percentage and multivariable logistic regression model were used to examine the prevalence and factors associated with pre-exposure prophylaxis awareness.
Results:
The prevalence of pre-exposure prophylaxis awareness was 8.2% (95% confidence interval = 7.8%–8.6%). Women’s age was positively associated pre-exposure prophylaxis awareness. Women with primary and secondary education had 39% and 48% higher odds of pre-exposure prophylaxis awareness, when compared with women with no formal education. The odds of pre-exposure prophylaxis awareness were 1.40 (95% confidence interval = 1.19–1.66) times higher among Christians when compared with the Muslims. Women who were exposed to mass media including newspaper or magazine, radio, TV, and Internet had higher odds of pre-exposure prophylaxis awareness, when compared with those without exposure to mass media channels. Women who have previously tested for HIV had 37% higher odds of pre-exposure prophylaxis awareness, when compared with those who have not been tested (adjusted odds ratio = 1.37; 95% confidence interval = 1.09–1.72).
Conclusion:
This study found women’s age, geographical region, education, religion, exposure to mass media channels, employment, and HIV testing to be associated with pre-exposure prophylaxis awareness. These findings can inform the development of targeted interventions and public health campaigns to increase awareness and practice to pre-exposure prophylaxis, particularly among key population.
Introduction
Global HIV/AIDS remains a major public health concern with Sub-Saharan Africa (SSA) accounting for more than 70% of the global burden of infection by 2022.1,2 Despite the Sustainable Development Goal Target 3.3 aiming to end the epidemic by 2030, 1.3 million people were newly infected with HIV worldwide in 2022. 3 Two-thirds of these infections occurred in SSA by 2022, where young women aged 15–24 years have eight times higher rates of HIV infection than their male counterparts.4 –6 This highlights the need for closing the gender gap in HIV prevention for women who are unable to access and negotiate current prevention options.7,8
In 2022, an estimated 0.7% HIV prevalence rate was reported among women aged 15–49 years in Burkina Faso, making 56,000 women aged 15 years and over living with HIV and accounts for 57.7% of all adults and children living with HIV. 9 Although considerable efforts have been made to combat HIV transmission through various interventions, 10 a relatively new approach known as pre-exposure prophylaxis (PrEP) has been recommended in the global fight against HIV. 4 PrEP involves taking antiretroviral medication before sex by individuals at high risk of contracting HIV to prevent infection.5,11 The efficacy of PrEP has been documented in the literature, indicating that using an overall sero-neutral approach has led to reductions in population-level HIV incidence at regional and city levels.12,13 Despite the acclaimed success rates, research on the prevalence and factors associated with PrEP knowledge for HIV prevention among Burkinabe women has not been explored. The prevalence of PrEP knowledge for HIV prevention among Burkinabe women, especially for adolescents and young women aged 15–25 years, is relatively low. 14 Women, particularly those in high-risk groups, such as sex workers and women in sero-discordant relationships, need access to accurate information about PrEP to make informed decisions about their sexual health.8,15
There are reports that suggest several factors that could explain the low PrEP knowledge and uptake among women, such as poverty, limited access to education, low literacy rates, and HIV-related stigma. 16 According to the 2021–2022 Human Development Index report, more than 40% of Burkina Faso’s population lives below the poverty line, ranking 184th out of 191 countries. 17 Limited access to education and low literacy rates among women in Burkina Faso could hinder their ability to access or understand health-related information, including PrEP.17,18 Studies have shown that the correlation between education and PrEP awareness is significant, with the less-educated being less likely to know about PrEP as a preventive measure against HIV/AIDS.19,20 HIV-related stigma is another significant barrier to PrEP knowledge. Women who are at risk for HIV may avoid seeking information about PrEP due to fear of judgment and discrimination, both within their communities and from healthcare providers. 19
In Burkina Faso, PrEP drugs are primarily sourced through public health programs, non-governmental organizations (NGOs), and private healthcare providers. The government may procure PrEP drugs through partnerships with international organizations like the Joint United Nations Programme on HIV/AIDS (UNAIDS), the World Health Organization (WHO), or through donations from pharmaceutical companies. NGOs and private healthcare providers may also distribute PrEP drugs as part of their HIV prevention programs. Access to PrEP drugs in Burkina Faso may vary depending on factors such as location, socioeconomic status, and availability of healthcare services. Limited access to healthcare services, especially in rural areas, also hinders women’s opportunities to receive information about PrEP or the drugs. 21
In the context of stigmatization, many women could lack regular contact with healthcare providers, which makes it difficult to obtain the knowledge needed to make informed decisions about their HIV prevention options.22,23 Cultural and religious beliefs are also key barriers to PrEP knowledge and use. For instance, cultural and religious beliefs may discourage women from seeking information related to orthodox medicine such as the uptake of PrEP.24,25 Furthermore, gender inequities in Burkina Faso could play a role in limiting women’s access to health information. Women often have less decision-making power in sexual relationships and may not be able to negotiate for the use of preventive medicine, 26 especially in the context of repeated intimate partner violence.8,27
Enhancing PrEP knowledge among women in Burkina Faso is vital for several reasons. First, it empowers women to take charge of their sexual health and make informed choices about HIV prevention.6,8 It can also reduce the risk of new HIV infections, 24 which is especially important in the context of the ongoing HIV epidemic in the country. 28 Moreover, improved PrEP knowledge can contribute to decreasing the stigma surrounding HIV infection and increasing awareness of the importance of regular HIV testing. 10 Despite the importance of PrEP awareness and uptake, yet, research to explore the prevalence and factors associated with PrEP awareness among women in Burkina Faso, to the best of our knowledge, has received limited attention. Identifying these factors and enhancing PrEP awareness are essential for reducing HIV transmission rates and promoting women’s health. 6 The objective of this study was to determine the level of awareness and associated factors of PrEP awareness among women of reproductive age in Burkina Faso. The findings would be useful for policymakers and stakeholders in healthcare system to institutionalize PrEP as an effective HIV prevention strategy among key population in the country.
Methods
Data source
Data from women’s survey questionnaire from the 2021 Burkina Faso Demographic and Health Survey (BDHS) was analyzed in this study. A total of 17,659 women of reproductive age (15–49 years) were included in the sample. Using systematic sampling with probability proportional to size, a two-stage stratified sample was used in the 2021 BDHS. Only the sample of women who provided an answer to the question about their awareness of PrEP was used for analysis in this article. This study is based on the analysis of secondary data that has been completely de-identified from the participants. We were given approval by Opinion Research Corporation (ORC) Macro, Inc. to use the Demographic and Health Survey (DHS) data in this investigation. Public access is available to the DHS data. The National Ethics Committee of Burkina Faso and the Internal Review Board (IRB) of the Centers for Disease Control (CDC) in Atlanta have given their ethical approval to the survey method and tools used. 29 We used the consensus-based checklist for reporting of survey studies (CROSS) to prepare this article.
Sample design
The BDHS sampling was designed to ensure adequate representativeness of the main indicators (apart from adult mortality and maternal mortality) at the national level, at the level of the 13 regions, at the city level of Ouagadougou, at the level of other cities, and at the level of rural areas. This is a stratified, two-stage area survey. The urban part and the rural part of each region each correspond to a sampling stratum. In total, 26 sampling strata were created. The primary sampling unit, also called a cluster, is the enumeration area (EA). At the first stage, 600 clusters including 195 located in urban areas and 405 in rural areas were selected to be mapped and surveyed. The clusters were drawn according to a systematic drawing with probability proportional to their household size, from the list of clusters established during the General Population and Housing Census carried out in 2019 by the Institute National Statistics and Demography. At the end of the first-stage drawing, a mapping and household enumeration operation was organized, from April 27 to June 28 2021 in the clusters drawn. This operation, which targeted all 600 clusters, was finally carried out in 572 clusters and made it possible to establish a location plan and a detailed sketch of the cluster by marking its limits, the locations of each structure found, and to draw up the updated list of households in each cluster.
The listing of households in the sample clusters was carried out using tablets which also made it possible to record the Global Positioning System (GPS) coordinates of the clusters and concessions. After drawing up the updated list of households in each cluster, a second-stage sample of 32 households per cluster in the Sahel region and 26 households in all other regions was drawn systematically and with equal probability. The BDHS sample focused only on ordinary households and therefore does not take into account the populations of collective households (hospitals, prisons, refugee, internally displaced persons camps, etc.). In the selected households, all women aged 15–49 years usually living there, or having spent the night before the interview, were eligible to be surveyed. Then, in a subsample of one in two households of all households in the sample, all men aged 15–59 years were eligible to be surveyed. In this subsample, all women aged 15–49 years were eligible for anemia testing; similarly, in this subsample, all children aged 6–59 months were eligible for testing for anemia and malaria. Finally, in this subsample of households, all women aged 15–49 years as well as all children under 5 years old were eligible to be measured and weighed to assess their nutritional status. In BDHS sample household, a single person was randomly selected from among women aged 15–49 years to answer the module’s questions regarding domestic violence. The details of DHS sampling design has been reported previously.29,30
Measures
Outcome variable
The outcome variable for this study is the awareness of PrEP among women of reproductive age in Burkina Faso. This was computed from the variable—V859 “Knowledge and attitude to PrEP to prevent getting HIV.” Women responded: “0—Haven’t heard,” “1—Heard and approve to take it every day,” “2—Heard, but don’t approve to take it every day,” and “3—Heard, but not sure about approving its use.” This variable was recoded dichotomously as “0” if have not heard and “1” if a woman has heard irrespective of her attitude toward it.
Explanatory variables
The factors examined in this study include sociodemographic and health variables such as age (in years) (15–19/20–24/25–29/30–34/35–39/40–44/45–49); geographical region (Boucle du Mouhoun/Cascades/Centre/Centre-Est/Centre-Nord/Centre-Ouest/Centre-Sud/Est/Hauts-Bassins/Nord/Plateau-Central/Sahel/Sud-Ouest); type of place of residence (urban/rural); religion (Muslim/Christian/other religion); sex of household head (male/female); exposure to newspaper or magazine (not at all/less than once a week/at least once a week); exposure to radio (not at all/less than once a week/at least once a week); exposure to television (not at all/less than once a week/at least once a week); exposure to Internet (not at all/less than once a week/at least once a week/almost every day); health insurance (not covered/covered); marital status (single/living in union/separated or widowed); age at first sex (never had sex/<18/18+); ever been tested for HIV (no/yes) and wealth status (poorest/poorer/middle/richer/richest). A composite index based on the household’s ownership of consumer items such as television, car, drinking water, and toilet facilities. In addition, women’s education (none/primary/secondary/higher) was also examined as an important socioeconomic variable. 31 These variables were included in the multivariable logistic regression model as they could be associated with PrEP awareness. For example, women who are covered by health insurance may have better access to health information during counseling at the health facilities.
Analytical approach
We used the survey module’s (“svy”) command to account for sampling design (clustering, stratification, and weighting) to take into account the multistage stratified cluster sample design. In the univariate analysis, percentage was used. In DHS data, sampling weights are crucial for producing nationally representative estimates. These weights are typically generated through a multistage process. First, inverse probability weights are calculated to adjust for the differential selection probabilities at each stage of sampling. This ensures that individuals from underrepresented groups have a proportionate influence on the final estimates. Next, non-response weights are applied to account for differences in response rates across various demographic groups. Finally, post-stratification weights are often used to align the sample with known population totals for key demographic variables, ensuring that the survey results are representative at the national level.
The chi-square test was conducted to examine the association between PrEP awareness and women’s characteristics. The factors which were significant in the bivariate analysis (chi-square test) were included in the multivariable logistic model. To examine the factors associated with PrEP awareness, multivariable logistic regression was used. In the multivariable binary logistic regression model, we computed the standard errors of the parameter estimates through several steps. First, the model coefficients were estimated using maximum likelihood estimation. Then, the variance-covariance matrix of the coefficient estimates was computed, which accounts for the uncertainty in the parameter estimates. This matrix was used to calculate the standard errors of the parameter estimates. Finally, confidence intervals for the parameter estimates were constructed using the standard errors. This process accounts for the uncertainty in the estimates and allows for the assessment of the precision of the parameter estimates in the logistic regression model.
Based on the estimation of multivariable logistic regression model, we predicted the probability of PrEP awareness. Thus

where Set[E = e] reflects putting all observations to a single exposure level e, and Z = z refers to a given set of observed values for the covariate vector Z. Furthermore,
Ethical consideration
Secondary data set that is available to the general public and has identifiers removed was analyzed. Following a recognized ethical procedure, BDHS obtained the respondents’ informed consent. No additional participants’ consent was needed because the authors were given permission to use these data which were collected following ethical standards. Here is where you can find details on DHS guidelines: http://goo.gl/ny8T6X.
Results
Table 1 shows the distribution of women’s characteristics by PrEP awareness. The prevalence of PrEP awareness among women in Burkina Faso was 8.2% (95% confidence interval (CI) = 7.8%–8.6%). Across the age categories, women aged 30–35 years had 10.0% (95% CI = 8.3%–11.9%), those from Sahel region had 20.8% (95% CI = 16.1%–26.5%), urban had 11.2% (95% CI = 9.6%–13.0%), those with higher education had 20.9% (95% CI = 15.7%–27.3%), and those who are covered by health insurance had 26.6% (95% CI = 18.3–37.0) PrEP awareness, respectively. Table 1 shows the variations of the level of PrEP awareness across women’s characteristics.
Characteristics and distribution of pre-exposure prophylaxis awareness (n = 17,659).
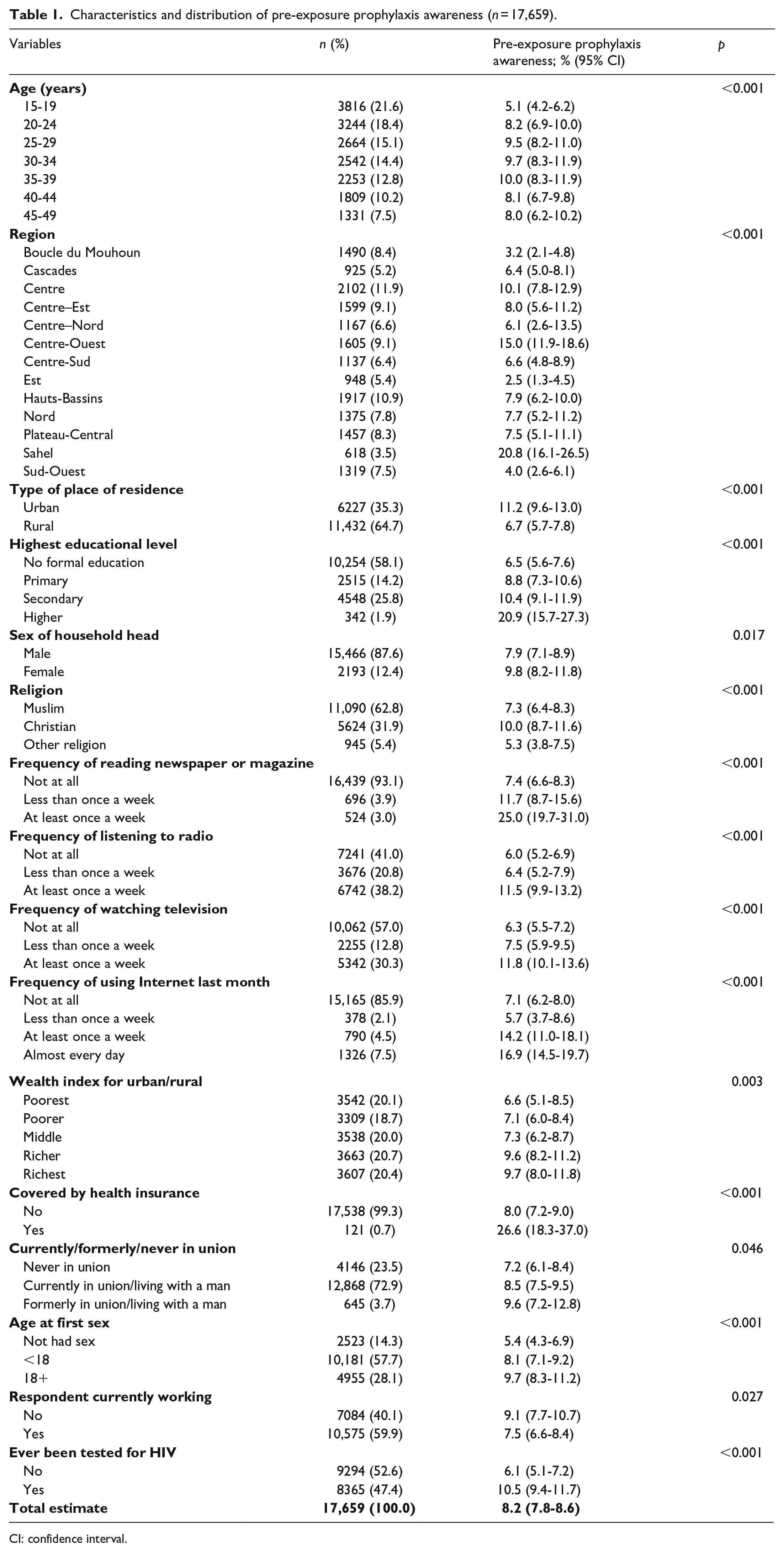
CI: confidence interval.
Results in Table 2 show that the odds of PrEP awareness were higher among older women, when compared with women aged 15–19 years. The geographical region was significantly associated with PrEP awareness. Women who have primary and secondary education had 39% (adjusted odds ratio (aOR) = 1.39; 95% CI = 1.13–1.72) and 48% (aOR = 1.48; 95% CI = 1.16–1.89) higher odds of PrEP awareness when compared with women with no formal education, respectively. The odds of PrEP awareness were higher among Christians, when compared with the Muslims (aOR = 1.40; 95% CI = 1.19–1.66). Women who were exposed to mass media including newspaper or magazine, radio, TV, and Internet had higher odds of PrEP awareness, when compared with those without exposure to mass media channels. Women who have previously tested for HIV had 37% higher odds of PrEP awareness, when compared with those who have not been tested (aOR = 1.37; 95% CI = 1.09–1.72) (see Table 2 for the details).
Measures of association of the factors associated with pre-exposure prophylaxis awareness.

CI: confidence interval.
In Table 3, the results of predictive marginal effect model are presented. This is to provide additional interpretation to the effects of the selected factors on the PrEP awareness among women in Burkina Faso. The predictive marginal model revealed that the probability of having PrEP awareness among women aged 35–39 years, Sahel, and the urban dwellers were 10.50%, 26.60%, and 8.80%, respectively. Also, assuming that the distribution of all factors remained constant among women, whereas every woman had higher education, 9.42% of the women are expected to have PrEP awareness. If every woman had ever been tested for HIV, we would expect 9.20% of them to have PrEP awareness (see Table 3 for the details).
Predictive marginal effect of the factors associated with pre-exposure prophylaxis awareness.
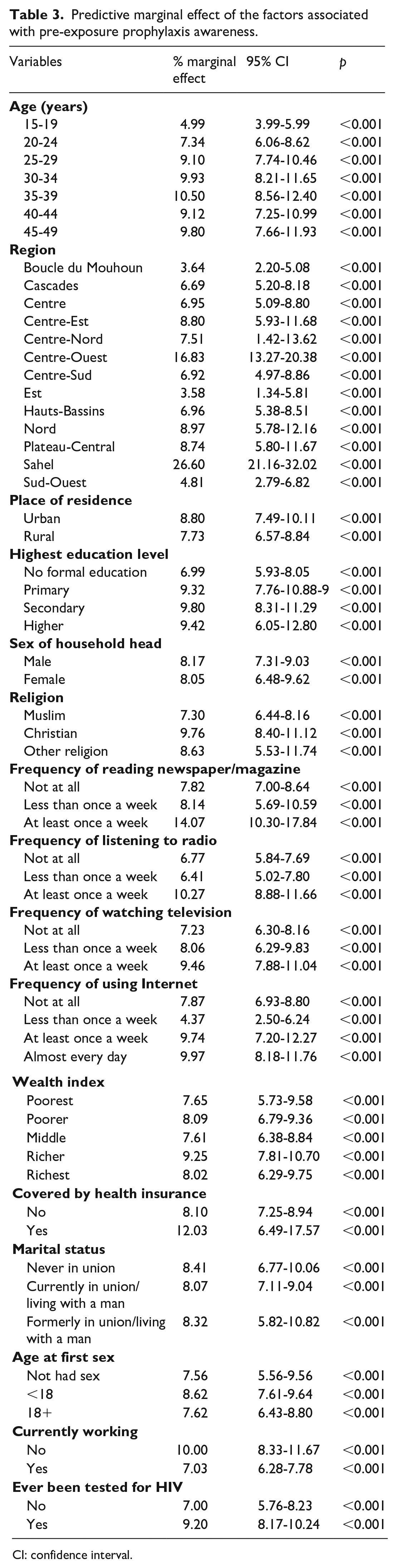
CI: confidence interval.
Discussion
The findings from this study provide crucial insights into the level of PrEP awareness among women in Burkina Faso. The study revealed that less than one-tenth (8.2%) of women had awareness of PrEP. This underscores the pressing need for concerted efforts in implementing HIV preventive interventions to increase both awareness and access to essential HIV prevention programs. Furthermore, the result highlights a substantial variation in PrEP awareness by women’s characteristics. Women’s age was positively associated with PrEP awareness. It suggests that as a woman gets older, her awareness about PrEP increases. This could be due to various factors such as increased access to information, more opportunities for education, or greater awareness campaigns targeting older women. It would be beneficial to explore this further to understand the implications and potential strategies for improving PrEP awareness among different age groups. In addition, women’s region was associated with PrEP awareness. Geographical region can, indeed, play a significant role in the availability, accessibility, and awareness of PrEP among women. Factors such as healthcare infrastructure, cultural norms, and government policies can vary widely between regions and impact the dissemination of information and services related to PrEP. Understanding these regional differences can help tailor interventions and education campaigns to improve PrEP uptake and awareness among women in different areas.
A remarkable proportion of women residing in urban locales demonstrated familiarity with PrEP. This finding is consistent with prior research emphasizing that urban areas typically possess superior healthcare infrastructure, easier access to health-related information, and greater awareness of HIV prevention strategies.33 –35 The pronounced urban–rural contrast underscores the need for tailored outreach programs designed to bridge this awareness gap, ensuring that rural communities gain equitable access to PrEP information and services. One of the most remarkable findings is the prevalence of PrEP awareness among women with higher education. As the level of education increases, so do the chances of women having awareness about PrEP. Women with primary and secondary education exhibit 20% and 30% higher odds of PrEP awareness, respectively, when compared to women with no formal education. This result is in harmony with previous studies that underscore the positive link between education and health literacy, encompassing understanding of preventive measures.36 –38 This emphasizes the need to bolster educational efforts to broaden PrEP awareness among women across all education levels.
In addition, the study revealed PrEP awareness disparities among women who practice different religion in Burkina Faso. There is a substantial difference in PrEP awareness between Christians and Muslims, with Christians having a 40% higher likelihood of PrEP awareness, when compared with their Muslim counterparts. This variation may be associated with differences in religious teachings, stigmas and religious norms regarding orthodox medicine such as HIV preventive methods.39 –41 This finding underscores the need for proactive efforts by religious or community organizations to educate their members about modern medicines such as HIV prevention strategies, including PrEP. Several studies have reported the influence of religious institutions on healthcare awareness and practices in diverse settings.42 –44 The government of Burkina Faso could use the religious platforms to disseminate health information to the populace.
Exposure to various media channels, including newspapers, magazines, radio, and the Internet, was linked to increased odds of PrEP awareness. This finding corroborates with previous research emphasizing the pivotal role of mass media in disseminating health-related information, including strategies for HIV prevention.45,46 Access to these media outlets can foster heightened awareness and understanding of PrEP intervention. Furthermore, women who had engaged in sexual activity were 1.40 times more likely to possess PrEP awareness, when compared with those who have never had sex. This suggests that individuals with a history of sexual activity may exhibit a greater inclination to seek information regarding sexually transmitted infections prevention methods, including the PrEP. This is consistent with the findings from previous studies that reported sexual activity served as a significant catalyst for interest in and awareness of HIV prevention strategies.47 –49 This study also identified women who had undergone HIV testing had a 30% higher likelihood of PrEP awareness in comparison to those who had not been tested. This could be attributed to the counseling and informational support typically provided alongside HIV testing services. Existing research has highlighted the significance of HIV testing centers as valuable platforms for disseminating information about PrEP and other preventive measures.50,51
Strengths and limitations
This study looked at awareness of PrEP for HIV prevention using a nationally representative large data set and was representative of all women of reproductive age. Therefore, the findings are suitable for making plausible comparisons. In the context of Burkina Faso, the study is the first of its kind. Furthermore, the survey was carried out in 2021, so the country’s current state of affairs is reflected in the current level of awareness about PrEP for HIV prevention. Our study did, however, have a few drawbacks. Because we conducted secondary data analysis, we had no control over the variable selection, data quality, or indicator measurement. However, since data from a cross-sectional study were analyzed, only association, not causality, can be established. Furthermore, what was measured in the DHS data were whether a person had heard of PrEP. This is quite different than having knowledge about PrEP (e.g. understanding that a person can use PrEP to prevent HIV, knowledge about the effectiveness of PrEP, knowledgeable about side effects, or knowledge about how to access the drug). Therefore, only awareness and not knowledge of PrEP could be examined in this study.
Conclusion
This research underscores the significance of factors such as age, geographical region, education, religiosity, exposure to mass media channels, employment, and HIV testing in shaping women’s awareness of PrEP in Burkina Faso. These findings can guide the design of focused initiatives and public health campaigns aimed at enhancing understanding and accessibility to PrEP. Consequently, this study emphasizes the need for concerted efforts in enhancing PrEP awareness, especially in rural settings and among women with diverse educational backgrounds. In addition, it suggests that partnerships with religious and community organizations can be an effective means for disseminating information regarding HIV prevention.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241259350 – Supplemental material for Prevalence and factors associated with pre-exposure prophylaxis awareness among cisgender women of reproductive age in Burkina Faso
Supplemental material, sj-docx-1-whe-10.1177_17455057241259350 for Prevalence and factors associated with pre-exposure prophylaxis awareness among cisgender women of reproductive age in Burkina Faso by Michael Ekholuenetale, Semiu Adebayo Rahman, Chimezie Igwegbe Nzoputam, Osaretin Godspower Okungbowa and Amadou Barrow in Women’s Health
Footnotes
Acknowledgements
The authors appreciate the MEASURE DHS project for the approval and access to the original data.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.