
Abstract
Background:
Survivors of intimate partner violence are at elevated risk for HIV acquisition, yet there is limited research on the best strategies to optimize biomedical HIV prevention, such as pre-exposure prophylaxis among this population. Domestic violence agencies are critical collaborating partners and function as potential entry points into HIV prevention services for survivors; however, limited knowledge regarding HIV prevention has been an important barrier to advocate-led discussions. This study aimed to develop, implement, and evaluate an HIV prevention intervention for domestic violence advocates.
Setting:
A nonrandomized, group-based intervention with pre-intervention, immediate post-intervention, and 3-month post-intervention periods were conducted with multiple domestic violence agencies in Mississippi.
Methods:
Overall, 25 domestic violence advocates participated in the two-session intervention. Surveys were administered to assess pre-exposure prophylaxis knowledge, self-efficacy, subjective norms, and willingness to provide HIV prevention services to intimate partner violence survivors. Generalized estimating equations were conducted to assess change in behavioral outcomes over time.
Results:
Compared to pre-intervention, there were significant increases at immediate and 3-month post-intervention in advocates’ intervention acceptability, pre-exposure prophylaxis knowledge, and self-efficacy to provide HIV prevention information, discuss pre-exposure prophylaxis eligibility criteria, assist pre-exposure prophylaxis-engaged clients, and initiate pre-exposure prophylaxis counseling.
Conclusion:
This group-based intervention enhanced domestic violence advocates’ acceptability, pre-exposure prophylaxis knowledge, and self-efficacy to offer HIV care information, discuss pre-exposure prophylaxis eligibility, assist pre-exposure prophylaxis-engaged survivors, and initiate pre-exposure prophylaxis counseling with intimate partner violence survivors. Efforts should focus on training domestic violence advocates in HIV prevention care for survivors and also include these agencies in collaborative strategies to reduce HIV incidence.
Introduction
Survivors of intimate partner violence (IPV) have a greater risk of HIV acquisition than individuals who have not experienced IPV.1,2 A meta-analysis found that survivors of IPV were 28% more likely to have HIV compared to their counterparts. 1 IPV survivors face several social and structural factors (e.g. poverty, stigma, and trauma) that constrain their access and ability to use and prioritize HIV prevention.3,4 Therefore, research examining the adoption of partner-independent HIV prevention among IPV survivors is critically needed.
Pre-exposure prophylaxis (PrEP), a biomedical HIV prevention strategy, might be an optimal partner-independent strategy for IPV survivors. PrEP does not require negotiation like condoms.3,5 In addition, PrEP can be taken independent of the sexual encounter and still protect against HIV.3,6
Despite these advantages, there is a consistent PrEP efficacy–effectiveness–implementation gap in the United States. Specifically, PrEP initiation (i.e. receiving a prescription) is lowest in the South compared to other regions 7 and PrEP initiation is lower among women than men. 8 Among the few women using PrEP, PrEP initiation is significantly lower among Black women than White women. 9 This is particularly important as Black women are disproportionately affected by HIV among women 10 and the HIV epidemic is most pronounced in the Deep South. 11 Furthermore, IPV escalates heterosexual transmission of HIV among women12,13 and Black women experience some of the highest rates of IPV nationally. 14 The confluence of gender, racial, and geographic disparities in PrEP initiation and IPV should be addressed in interventional research aimed at increasing PrEP adoption among women.
Optimizing PrEP implementation in non-medical settings, such as domestic violence agencies, may increase PrEP access and initiation among IPV survivors. Domestic violence agencies are safe, formal social structures in which survivors can openly discuss their relationships15,16 and access resources to rebuild their lives. 15 Despite their pivotal role in survivors’ lives, there is a dearth of research integrating HIV prevention into domestic violence agencies. Prior research has conducted individual-level interventions to increase HIV prevention among survivors,17,18 but few interventions have been designed to increase advocate awareness and understanding of HIV prevention, specifically PrEP. Educational interventions are effective methods for training non-clinician service providers in health promotion and risk prevention.19,20 A PrEP educational intervention adapted to the context of domestic violence agencies and the lives of IPV survivors may be a promising, novel strategy to address PrEP implementation barriers to increase PrEP initiation among survivors. The purpose of this study was to develop and pilot-test a PrEP educational intervention for domestic violence advocates providing care to women in HIV geographical hotspots.
Methods
Procedures
Between March and June 2021, domestic violence advocates participated in a nonrandomized two-session, group-based educational intervention trial to increase awareness and self-efficacy to offer HIV prevention information to their clients. The intervention was led by PhD-level and MPH-level trained facilitators who were not affiliated with the domestic violence agencies. Advocates were eligible for the study if they were aged 18 years or above, spoke English, and were currently employed at a domestic violence agency in Mississippi.
Advocates were initially recruited through the state domestic violence coalition agency. Eligible staff were sent emails before the scheduled training to invite them to participate in the intervention and to complete the pre-intervention survey. Study participation was voluntary, and participants had the option to attend the training without intervention enrollment. Before study enrollment, participants provided informed written consent. Immediately following the intervention, participants were invited to complete the post-intervention survey. In 3 months following the intervention, participants were asked to complete the final survey. Participants received continuing education credits for their participation in the training. Participants were remunerated US$15 for completing the 3-month post-intervention survey. The Johns Hopkins University Bloomberg School of Public Health Institutional Review Board (IRB) approved all study procedures (IRB#15804).
Intervention components
Table 1 highlights the key components of the intervention, including the determinants and related content. Similar to prior research on clinical interventions 21 and HIV prevention, 22 this intervention was guided by two theoretical frameworks: Information, Motivation, and Behavioral Skills 23 and Theory of Planned Behavior. 24 Thus, this study hypothesized that offering knowledge regarding HIV epidemiology and prevention, and discussing the benefits of HIV prevention for IPV survivors would enhance advocate knowledge, promote positive attitudes toward HIV prevention, and enhance advocate’s self-efficacy to discuss HIV prevention with survivors. While information, motivation, and self-efficacy were derived from the Information, Motivation, and Behavioral Skills framework, 23 this study also include subjective norms as a construct from Theory of Planned Behavior. 24 Subjective norms within the institution (i.e. domestic violence agencies) refer to the belief of whether the organization would approve or disapprove of advocates discussing and disseminating HIV prevention information in these settings. These subjective norms may be an important contributor to advocate’s behavior change (i.e. discussing HIV prevention with clients/survivors). The intervention was administered in two sessions. Each session lasted 60 min with a total of 120 min involved in the intervention.
Intervention components.
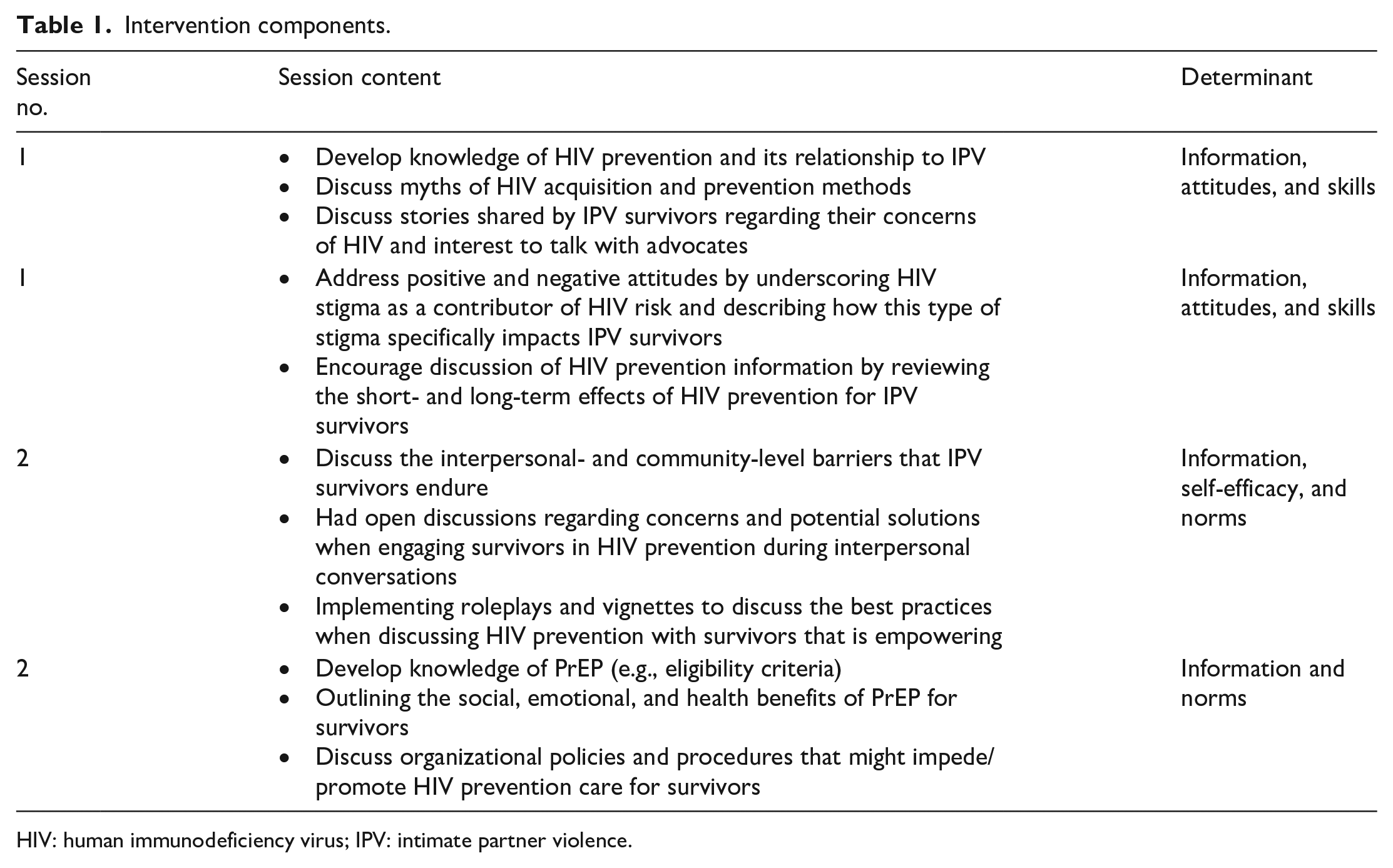
HIV: human immunodeficiency virus; IPV: intimate partner violence.
Measures
Acceptability
Participants were asked four items regarding their level of agreement of their ability to discuss topics related to HIV prevention among IPV survivors. The following four items were developed by White Hughto et al. 21 and modified to HIV prevention and IPV context: “I can define terms related to HIV risk and prevention”; “I can identify social factors that place women experiencing partner violence at the risk of HIV acquisition”; “I can communicate with women experiencing partner violence using language that respects and is non-judgmental of women’s sexual risk behaviors”; and “I can explain strategies to effectively take a sexual history.” Response options were on a 5-point Likert-type scale (1 = Strongly Disagree to 5 = Strongly Agree). The responses were summed to create a total score.
Feasibility
Feasibility was measured by enrollment and retention rates, and participants’ satisfaction with the educational intervention. A research team member kept track of the number of referrals, enrollment rates, and retention rates. Satisfaction was measured at the end of the post-intervention period. Participants were asked whether they would recommend the training to others with the response options of Yes (1) versus No (0).
Screening
Participants were asked if they will routinely screen clients for sexual risk history. Participants were able to respond as Yes (1) versus No (0).
PrEP knowledge
A five-item validated PrEP Knowledge scale was used. 25 Each correct answer was coded as 1 and incorrect answers were coded as 0. The final scores were calculated by summing across all five items.
Self-efficacy
Four self-efficacy items were asked to assess confidence in offering HIV prevention information, discussing PrEP eligibility criteria, assisting PrEP-engaged clients, and initiating PrEP counseling. Response options were on a 5-point Likert-type scale (1 = Strongly Disagree to 5 = Strongly Agree).
Institutional subjective norms
Seven items were asked to assess subjective norms regarding implementing HIV prevention in domestic violence agencies. The scale was developed by White Hughto et al. 21 and modified to HIV prevention in domestic violence agencies: “HIV prevention is an important issue for residents at my domestic violence agency”; “Domestic violence agencies are an appropriate place to address HIV”; “Domestic violence agency involvement in HIV prevention could have positive impacts on clients’ health”; “Domestic violence agencies should not address HIV risk with clients”; “Domestic violence agencies should not address PrEP with clients”; “People who influence my workplace behavior think that I should provide HIV prevention information to clients”; and “People who influence my workplace behavior think that I should provide PrEP information to clients.” Response options were on a 5-point Likert-type scale (1 = Strongly Disagree to 5 = Strongly Agree). The responses were summed to create a total score.
Barriers to HIV prevention
At the 3-month follow-up, issues related to impediments in providing HIV prevention information in domestic violence agencies were assessed using a six-item validated scale developed by Rountree et al. 26 We modified this scale to include 12 additional items regarding training, organizational policies, time, and additional resources. Response options were Disagree, Agree, and Unsure. We calculated the frequency of agreement with each of the items. Participants were also asked two follow-up qualitative questions to assess recommendations and solutions for addressing some of the aforementioned challenges.
Demographics and employment characteristics
Participants were asked to self-report: age (in years), sex (female versus male), race and ethnicity (Black, White, Hispanic, Asian, Native Hawaiian or Other Pacific Islander, American Indian or Alaska Native, and Other), primary role (e.g. counselor, victim advocate), years of experience in the profession, and having direct contact with survivors.
Data analysis
Descriptive statistics (e.g. mean, frequencies) were conducted among all demographic characteristics. Changes in the means of the outcomes (i.e. acceptability, screening, HIV prevention competence, self-efficacy, and institutional subjective norms) were calculated (Hedge’s g). Eight linear regression models were conducted using generalizing estimating equations (GEE) to examine change over time in the outcomes.27,28 To assess change over time, time was entered into all GEE models as the primary predictor with pre-intervention as the referent.
Results
Overall, 25 advocates participated in the training, and 20 completed the pre-intervention survey, 20 completed the immediate post-intervention survey (100% retention), and 9 completed the 3-month post-intervention survey (45% retention). The domestic violence agencies experienced significant turnover during the follow-up period which contributed to the low retention rate. There was high satisfaction with the educational intervention. At pre-intervention and immediate post-intervention, 100% of the participants reported that they would recommend the training to others in their field. At 3-month post-intervention, 67% of the participants reported that they did recommend the training to others in their field.
The average age was 42.1 (SD = 10.6) years, and the average number of years of experience was 5.3 (SD = 3.9) years. The full sample self-identified as female (20/20). Half of the sample identified as non-Hispanic Black (9/20), and slightly less than half of the sample identified as non-Hispanic White (7/20). Half of the sample reported having direct contact with IPV survivors (10/20).
The measures of acceptability and institutional subjective norms demonstrated adequate internal consistency. For acceptability, the Cronbach’s alpha = 0.71 at pre-intervention, 0.87 at immediate post-intervention, and 0.72 at 3-month post-intervention. For institutional subjective norms, the Cronbach’s alpha = 0.69 at pre-intervention, 0.71 at immediate post-intervention, and 0.60 at 3-month post-intervention.
Table 2 displays the means, standard deviations, and effect sizes of all the outcomes from pre-intervention to 3-month post-intervention. Compared to pre-intervention, all outcome variables tended to increase during the immediate post-intervention and 3-month post-intervention periods. There were moderate to large effect sizes for acceptability, the self-efficacy constructs, and PrEP knowledge.
Means, standard deviations, and effect sizes of intervention outcomes across all timepoints.
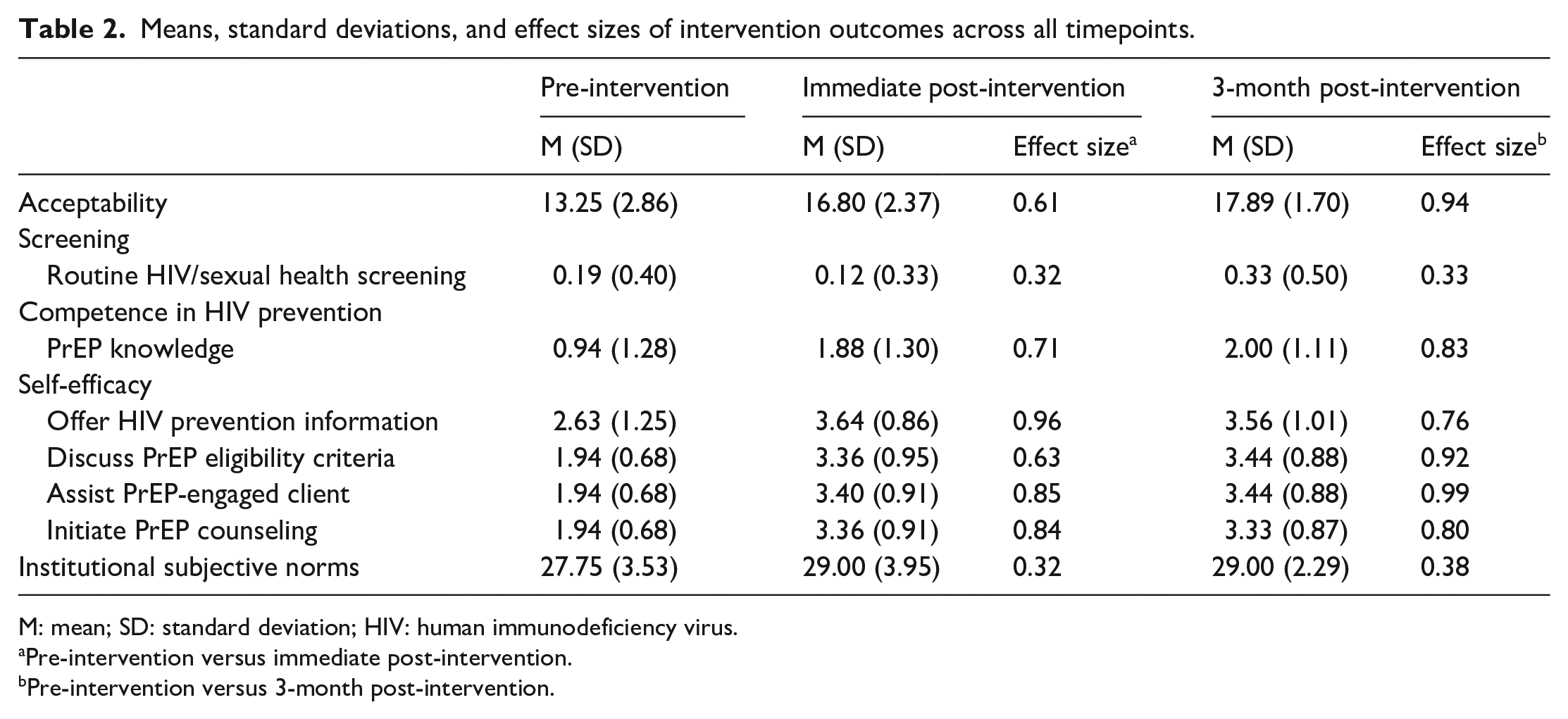
M: mean; SD: standard deviation; HIV: human immunodeficiency virus.
Pre-intervention versus immediate post-intervention.
Pre-intervention versus 3-month post-intervention.
Table 3 displays the effect estimates representing changes in outcomes over time. Compared to the pre-intervention period, all participants’ acceptability increased at immediate post-intervention (B (95% CI) = 3.68 (2.60, 4.76), p = 0.00) and 3-month post-intervention (B (95% CI) = 4.59 (3.47, 5.71), p = 0.00). Similarly, participants’ PrEP knowledge increased at immediate post-intervention (B (95% CI) = .94 (0.43, 1.44), p = 0.00) and 3-month post-intervention (B (95% CI) = 1.04 (0.30, 1.78), p = 0.00) compared to the pre-intervention period. Compared to the pre-intervention period, participants’ self-efficacy to offer HIV prevention information increased at immediate post-intervention (B (95% CI) = 1.01 (0.36, 1.66), p = 0.00) and 3-month post-intervention (B (95% CI) = 0.93 (0.23, 1.63), p = 0.00). Compared to the pre-intervention period, participants’ self-efficacy to discuss PrEP eligibility criteria increased at immediate-post-intervention (B (95% CI) = 1.42 (1.10, 1.78), p = 0.00) and 3-month post-intervention (B (95% CI) = 1.51 (0.98, 2.02), p = 0.00). Compared to the pre-intervention period, participants’ self-efficacy to assist PrEP-engaged clients increased at immediate-post-intervention (B (95% CI) = 2.92 (2.23, 3.60), p = 0.00) and 3-month post-intervention (B (95% CI) = 2.88 (1.87, 3.89), p = 0.00). Finally, participants’ self-efficacy to initiate PrEP counseling increased at immediate post-intervention (B (95% CI) = 0.92 (0.43, 1.40), p = 0.00) and 3-month post-intervention (B (95% CI) = 1.07 (0.17, 1.96), p = 0.02) compared to the pre-intervention period.
Changes in primary and secondary outcomes at immediate post-intervention and 3-month post-intervention.

CI: confidence interval; HIV: human immunodeficiency virus. Pre-intervention is the reference timepoint.
Figure 1 is a joint display showing the top five barriers endorsed by participants. Overall, 43% of participants felt they need more training, 38% of participants endorsed needing more support from their supervisor, and 33% of participants endorsed feeling this was outside of their role as an advocate. However, 14% of participants indicated that they did not know of anywhere they could send a survivor for PrEP care, and 14% of participants endorsed not knowing of anywhere they could send a survivor for help if they identified being at risk for HIV. Potential solutions directly expressed by participants regarding needing more training were, “Learning more about the treatments,” “HIV assistance in my area for survivors,” “A follow-up training,” and “All topics related to HIV.” Furthermore, solutions indicated in response to needing more support from a supervisor included, “Making sure appropriate training is provided,” “More training opportunities—working on ways to discuss HIV risk with clients in a safe way,” and “In-service training by local resources.”
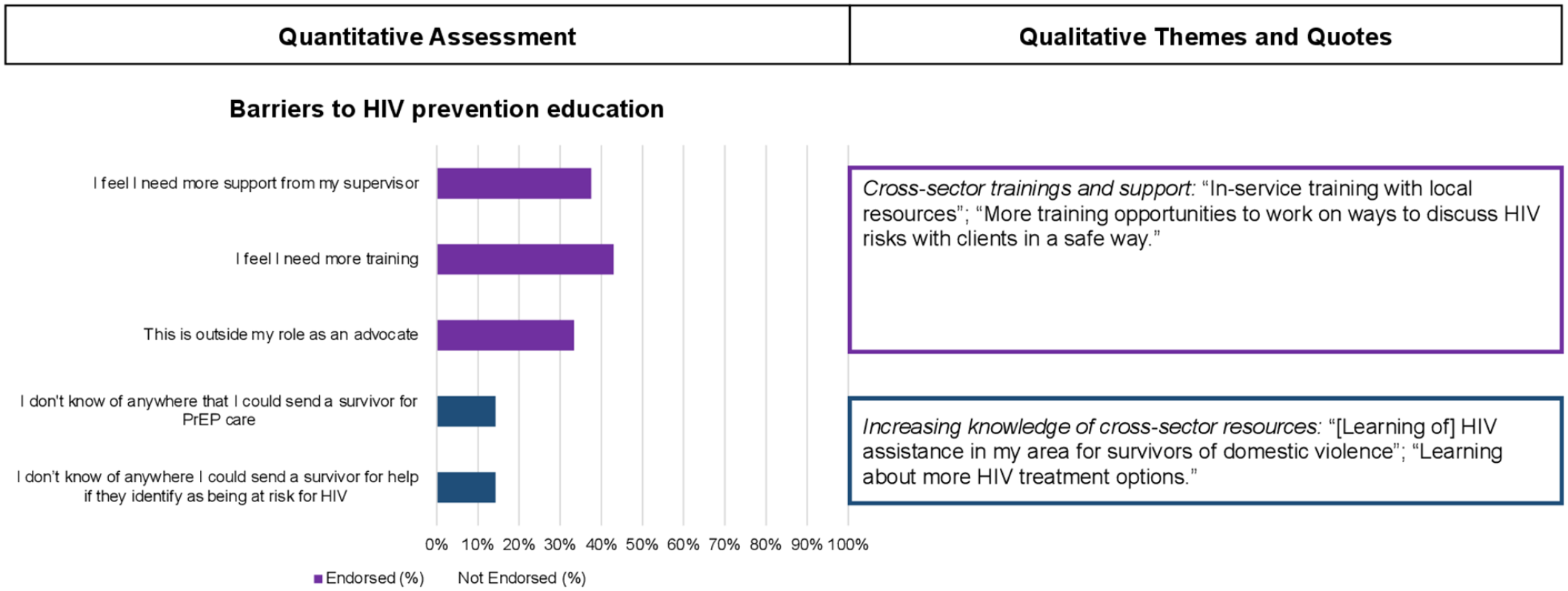
Joint display integrating quantitative and qualitative results on barriers to HIV prevention in domestic violence agencies and potential solutions.
Discussion
Leveraging foundational qualitative research with IPV survivors 5 and domestic violence advocates, 4 a group-based educational intervention based on the lived realities of IPV survivors and the context of domestic violence agencies was developed and implemented to employees with domestic violence agencies. Our preliminary findings indicate high acceptability and feasibility of the intervention, and evidence that the intervention can increase self-efficacy to provide HIV prevention information and care to IPV survivors, PrEP knowledge, and sexual health screening behaviors. This is one of the first studies to design an HIV prevention curriculum for domestic violence agencies with an emphasis on PrEP implementation. Given the importance of domestic violence agencies to IPV survivors, future research is needed to conduct a fully powered efficacy trial to assess the effects of the intervention on advocates’ behaviors and potentially patient-level outcomes as well.
Our formative research with IPV survivors and domestic violence advocates4,5 illustrated important provider-level barriers to PrEP initiation, including a lack of PrEP knowledge, among domestic violence advocates. Therefore, this brief educational intervention trained domestic violence advocates on HIV prevention with an emphasis on PrEP use and its advantages for survivors of IPV. This educational intervention comprised PrEP efficacy, modalities, and coverage in addition to strategies to incorporate trauma-informed policies and PrEP services. Our evaluation of the intervention demonstrates preliminary efficacy to address key components that would influence advocates’ behaviors, such as self-efficacy and PrEP knowledge. Also, our findings indicate that some of the intervention effects are retained over time. Future testing of the intervention should recruit a large sample of domestic violence advocates in multiple HIV hotspots.
Finally, participants highlighted some key barriers to HIV prevention education in their setting but identified potential solutions. While the intervention was highly acceptable and feasible, some advocates felt that they needed more inter- and intra-organizational support for HIV prevention resources and raised the PrEP purview paradox 29 (i.e. concerns about whether this form of care was outside their role). Participants shared that cross-sector training and resources would help increase not only the awareness of local HIV prevention resources but also facilitate collaborations with local community partners to educate, counsel, and empower survivors to access PrEP.
There are study limitations. Since the primary goal of the pilot study was to demonstrate acceptability and feasibility, the study was not a fully powered efficacy trial. Randomization at the individual level was not possible because multiple domestic violence agencies were able to attend the training sessions. Some of the participants did not report direct contact with IPV survivors because direct care was not their primary role (i.e. front desk receptionist). The educational intervention was offered to all employees regardless of their direct or indirect contact with survivors because all employees participate in the organizational policies, climate, and subjective norms that may influence the acceptability of HIV prevention in these unique community-based settings. This study was also conducted with domestic violence advocates in the US South in an Ending the HIV Epidemic priority area, but the findings may not be generalizable to geographic areas outside of this priority area.
Conclusion
This study is among the first to develop and evaluate a PrEP educational intervention among domestic violence advocates and providers. Findings from this study demonstrate the potential for community-based organizations, such as domestic violence agencies, to be important collaborators in HIV prevention programming for IPV survivors. As trauma-informed approaches become integrated into PrEP services, collaborative relationships with domestic violence agencies could be a critical step toward curbing the risk of HIV infection among IPV survivors.
Supplemental Material
sj-docx-1-whe-10.1177_17455065211070548 – Supplemental material for Enhancing domestic violence advocates’ ability to discuss HIV pre-exposure prophylaxis (PrEP): Feasibility and acceptability of an educational intervention
Supplemental material, sj-docx-1-whe-10.1177_17455065211070548 for Enhancing domestic violence advocates’ ability to discuss HIV pre-exposure prophylaxis (PrEP): Feasibility and acceptability of an educational intervention by Tiara C Willie, Laurel Sharpless, Mauda Monger, Trace S Kershaw, Wendy B Mahoney and Jamila K Stockman in Women’s Health
Footnotes
Acknowledgements
The authors thank the Mississippi Coalition Against Domestic Violence for allowing them to share their educational intervention. The authors also thank the participants who completed the study activities for this project.
Author contributions
T.C.W. formulated the overarching research aims for this study; T.C.W. and W.B.M. maintained the research data for initial use; T.C.W. and L.S. conducted the statistical analyses to synthesize the research data; T.C.W. acquired the funding to support this project; M.M., T.S.K., and J.K.S. participated in the conduct of the research investigation processes and also provided guidance into the design of the research methodologies; T.C.W. and M.M. coordinated the research activity planning and execution; J.K.S. provided external mentorship to the core research team. L.S. and T.S.K. reviewed and validated the results from the statistical tests; L.S. designed the initial drafts of the data visualization. All authors reviewed the initial and revised versions of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.C.W. was supported by the National Institute on Minority Health and Health Disparities (NIMHD) of the National Institutes of Health under Award No. K01MD015005. This work was also supported by the Johns Hopkins Center for AIDS Research (P30AI094189) and the San Diego Center for AIDS Research (P30AI036214). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.