
Abstract
Background:
Cervical cancer is one of the leading causes of morbidity and mortality among women globally, particularly in regions with limited access to preventive healthcare services. Despite the availability of effective screening methods, uptake remains suboptimal among healthcare professionals.
Objectives:
This study assessed the knowledge, attitudes, and barriers to cervical cancer screening among female healthcare professionals at Tamale Teaching Hospital.
Design:
An institution-based cross-sectional study was conducted among 221 female nurses, 27 female midwives, and 30 female medical doctors in the Tamale Metropolis from October to December 2024.
Methods:
A total of 278 female healthcare professionals were recruited using a simple random sampling method to ensure a representative sample. Data were collected through structured questionnaires and analyzed using SAS JMP Pro Statistical Software version 17.1: JMP Statistical Discovery, LLC (a subsidiary of SAS Institute).
Results:
Of the 278 respondents, more than half (58.6%) had good knowledge of cervical cancer and its screening methods. Factors associated with knowledge of cervical cancer were education (p = 0.002) and professional category (p = 0.039). Moreover, attitudes toward cervical cancer screening were generally positive, with 92.8% agreeing on its importance and 91.8% willing to encourage others to participate. However, the utilization of cervical cancer screening was low (33.1%). The most common barriers to screening utilization included having no reason (72.8%), tight schedules (71.1%), financial constraints (69.5%), and fear of screening outcomes (66.3%).
Conclusion:
Despite positive knowledge and attitudes toward cervical cancer screening, barriers hindered uptake. Workplace-based screening programs are needed to improve screening participation among female healthcare professionals.
Introduction
Cervical cancer is a major global public health challenge, 1 and the fourth leading cause of gynecological cancer-related deaths among women worldwide. 2 It is predominantly caused by persistent infection with high-risk strains of the human papillomavirus (HPV), which can progress from preinvasive cervical lesions to invasive cancer.3,4 In 2020, the global burden of cervical cancer was estimated at 604,000 new cases and 341,000 deaths.5,6 Although high-income countries have significantly reduced incidence and mortality through widespread HPV vaccination, routine screening, and early treatment,7,8 low- and middle-income countries (LMICs) continue to bear the greatest burden due to limited access to preventive services.9,10
According to the Global Cancer Observatory (GLOBOCAN 2022), cervical cancer remained a major concern in 2022, with 662,301 new cases (6.9% of female cancers), ranking fourth after breast, lung, and colorectal cancers.2,11 It caused 348,874 deaths worldwide, and the 5-year prevalence was 1,948,521 cases. In Africa, the disease is particularly devastating, with approximately 119,284 new cases and 81,687 deaths annually among women aged 15 years and older.2,5 These figures highlight the disproportionate burden of cervical cancer in low- and middle-income regions, where access to HPV vaccination, routine screening, and early treatment remains limited. 12
In response, international health authorities have developed clear guidelines and targets. The American College of Obstetrics and Gynecology recommends Pap smear screening every 3 years for women aged 21–29 and HPV testing every 5 years until age 65.13,14 Similarly, the World Health Organization launched a strategy in 2020 aiming to eliminate cervical cancer by 2030 through the 90-70-90 targets: vaccinating 90% of girls against HPV by age 15, screening 70% of women by ages 35 and 45, and treating 90% of women with cervical disease.15,16 Despite these global efforts, many LMICs, including Ghana, continue to face challenges in cervical cancer prevention. 17
In Ghana, cervical cancer remains the second most common female cancer and the third leading cause of cancer deaths among women aged 15–44.18,19 The country records an annual incidence of 18.3 cases per 100,000 women, 20 corresponding to approximately 3151 new diagnoses and 2119 deaths each year.21,22 Factors contributing to poor outcomes include late detection, low awareness, socioeconomic constraints, limited healthcare infrastructure, and cultural or religious beliefs.18,23 Alarmingly, fewer than 3% of eligible women are screened for cervical pre-cancer in Ghana, and HPV vaccination is not yet part of the national immunization program.24,25 Barriers include limited knowledge, high costs, fear of diagnosis, procedural discomfort, gender of screeners, privacy concerns, stigma, misconceptions, and cultural or religious resistance.9,22,26,27
Healthcare professionals play a pivotal role in reversing the cervical cancer burden, as they serve as frontline advocates for awareness, screening, and vaccination. 28 However, in Ghana, evidence indicates substantial knowledge gaps and low screening uptake among healthcare professionals themselves. For instance, a study in the Upper East Region reported poor knowledge (51.7%) and low participation in cervical cancer screening (64.9%). 29 Similarly, in the Greater Accra Region, only 34% of healthcare professionals had undergone screening, while about 40% demonstrated inadequate knowledge of cervical cancer signs and symptoms. 30 Another study in Accra revealed significant knowledge gaps regarding cervical cancer risk factors and attitudes toward cervical cancer vaccination. 31 In the Central Region, although healthcare professionals demonstrated some knowledge of cervical cancer, their patronage of recommended screening practices remained low. 32 This is concerning, as healthcare professionals are expected to model preventive health behaviors and influence community practices. Despite their critical role, there is limited literature focusing on healthcare professionals in Northern Ghana, where healthcare disparities are often more pronounced. 33 Without an assessment of their knowledge, attitudes, and barriers to screening, important gaps may remain unaddressed, which can lead to continued low uptake of preventive services, late diagnosis, and persistently high mortality rates. This study, therefore, sought to assess the knowledge, attitudes, and screening barriers among female healthcare professionals at Tamale Teaching Hospital (TTH). Findings are expected to generate context-specific evidence that will inform targeted interventions and policy strategies aimed at improving cervical cancer prevention and control in Northern Ghana.
Materials and methods
Study design
An institution-based cross-sectional study was conducted to assess the knowledge, attitudes, and barriers to cervical cancer screening utilization among female healthcare professionals, including nurses, midwives, and medical doctors, at TTH. The study was conducted over a 3-month period, from October 2024 to December 2024. The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for cross-sectional studies. 34
Study area and population
The study was conducted at TTH, the only tertiary hospital in Northern Ghana, which provides a wide range of healthcare services, including Trauma and Orthopedics, ENT, and Obstetrics and Gynecology, among others. The hospital has a total of 814 nursing professionals (including female nurses and midwives) and 97 female medical doctors, bringing the total number of female healthcare professionals to 911. This study focused on permanently employed female nurses and doctors at the hospital, as they represent the largest group of frontline providers involved in direct patient care. Their role puts them at greater risk, as they play a crucial part in health education and cervical cancer screening.
Inclusion and exclusion criteria
Eligible respondents were female healthcare professionals (nurses, midwives, and medical doctors) permanently employed at the hospital, belonging to the designated professional categories, who provided consent and were willing to participate voluntarily in the study. Respondents who were on leave and absent during the study period were excluded from the study.
Sample size determination and sampling method
The sample size for this study was determined using Yamane’s formula for a known population: n = N/(1 + N(e) 2 ). 35 With a target population (N) of 911 and a margin of error (e) of 5%, the calculated sample size (n) was 278. A proportionate sampling approach was applied to allocate the sample across professional categories, resulting in 248 nursing professionals and 30 female medical doctors. Individual respondents were selected using a simple random sampling technique, facilitated by SAS JMP Professional Statistical Software version 17.1: JMP Statistical Discovery, LLC (a subsidiary of SAS Institute). A comprehensive list of health system employees (female nursing professionals and medical doctors) available during the study period was obtained from hospital management and imported into SAS JMP. Using the “Random-Sample Size” function, the desired sample size was specified, and the software randomly selected participants from the list. The selected nursing professionals and medical doctors were then traced to their respective wards, where data collection took place during their shifts.
Data collection tool
A structured, validated questionnaire, adapted from a previous study, 36 was used to collect data from the respondents. The questionnaire consisted of four sections. The first section gathered sociodemographic information through eight questions, including age, professional category, rank, education, religion, marital status, family history of cervical cancer, work experience, and number of children. The second section collected data on respondents’ knowledge of cervical cancer and its screening methods through 19 questions, with response options “Yes/No/I don’t know.” Knowledge levels were measured by assigning a score of “1” to correct answers and “0” to incorrect or “don’t know” responses. The total score ranged from 0 to 19, with a median score of 10 or above indicating “good knowledge,” while a score below 10 represented “poor knowledge.” The third section assessed respondents’ attitudes toward cervical cancer and its screening through six items, with response options ranging from “Strongly disagree” to “Strongly agree.” Higher scores indicated more positive attitudes toward cervical cancer and its screening. The fourth section assessed barriers to cervical cancer screening uptake through nine items, with response options “Yes/No,” and multiple responses were allowed to capture the various factors that might hinder respondents from participating in cervical cancer screening (Supplemental Material).
Validity and reliability
The principal investigator, who also supervised the study, organized a 1-day training for the research team. The structured questionnaire was evaluated to ensure accuracy and consistency. To establish content validity, experts were consulted, and their feedback was critically analyzed to refine the questionnaire items. The final questionnaire content validity was established by consulting five experts in the field, who rated each questionnaire item for relevance using a 4-point scale (1 = not relevant to 4 = highly relevant). The item-level content validity index (I-CVI) was calculated for each item, and items with an I-CVI ⩾0.80 were retained. The overall scale-level CVI was 0.92, indicating excellent content validity. Reliability was assessed using established statistical methods: the knowledge questionnaire demonstrated good internal consistency with a Kuder-Richardson formula 20 (KR-20) value of 0.79; the attitude scale showed acceptable reliability with a Cronbach’s alpha of 0.75; and the barriers to cervical cancer screening uptake section had a KR-20 of 0.72. The KR-20 was employed for the knowledge and barrier items because they were dichotomously scored (yes/no), which makes KR-20 the most appropriate reliability coefficient for such measures. 37 In contrast, Cronbach’s alpha was used for the attitude scale since it was measured with a Likert format, where internal consistency is best captured using alpha coefficients. 38 Together, these results indicate that the tool was both valid and reliable for assessing knowledge, attitudes, and barriers to cervical cancer screening among the study population.
Data collection procedure
Data collection began after obtaining permission from the hospital and informed consent from the respondents. Respondents were given 10–20 min to complete the questionnaire at their convenience, ensuring privacy and confidentiality. The questionnaires, along with consent forms, were placed in envelopes and sealed. This was done privately, using nurse managers’ rooms where available. Upon completion, the principal investigator reviewed the questionnaires for completeness and securely stored them in locked bags accessible only to the research team.
Statistical analysis
Microsoft Excel 2021 was used to clean the data, which was subsequently exported to SAS JMP Pro Statistical Software version 17.1: JMP Statistical Discovery, LLC (a subsidiary of SAS Institute) for statistical analysis. For categorical variables, frequency and percentage were computed, while means and standard deviations were computed for numerical variables and summarized in simple tables. An exploratory factor analysis was conducted to identify the underlying dimensions of attitudes toward cervical cancer and its screening. The analysis extracted two factors: factor 1—Emotional response and perception, and factor 2—Willingness to encourage others to participate in screening. To assess the association between cervical cancer knowledge and sociodemographic factors, the Cochran-Armitage test for trend was used for ordinal variables (age, education, work experience, number of children) to detect significant linear trends, with results presented as Z statistics (Z) and p-values. The chi-square test assessed associations with nominal variables (professional category, religion, marital status, family history of cervical cancer), with results also reported as chi-square statistics (χ2) and p-values. Moreover, one-way analysis of variance and independent two-sample t-tests were used to examine the relationship between attitudes toward cervical cancer screening and sociodemographic characteristics. Assumptions for all statistical tests were checked and verified prior to analysis. Statistical significance was considered at p < 0.05.
Ethical considerations
Ethical approval was obtained from the Committee on Human Research, Publications, and Ethics at Kwame Nkrumah University of Science and Technology (CHRPE/AP/1001/24). Permission was also granted by the Research and Development Unit of Tamale Teaching Hospital (TTH/R&D/SR/24/059). Respondents were fully informed of the study’s purpose, and both written and verbal informed consent were obtained. Confidentiality was maintained, with no personal identifiers linked to responses. Participation was voluntary, and respondents were assured of their right to withdraw at any time. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Sociodemographic characteristics
A total of 278 questionnaires were distributed, all of which were completed and returned, yielding a 100% response rate. As shown in Table 1, the majority of respondents were aged 26–30 years (35.6%), identified as Muslim (57.6%), and were married (54.0%). Professionally, nurses represented the largest group (83.1%). Regarding educational attainment, 43.9% held a bachelor’s degree. More than half of the respondents (56.5%) had less than 5 years of work experience, and 44.6% reported having no children. Only 6.5% indicated a family history of cervical cancer.
Sociodemographic characteristics of respondents (N = 278).
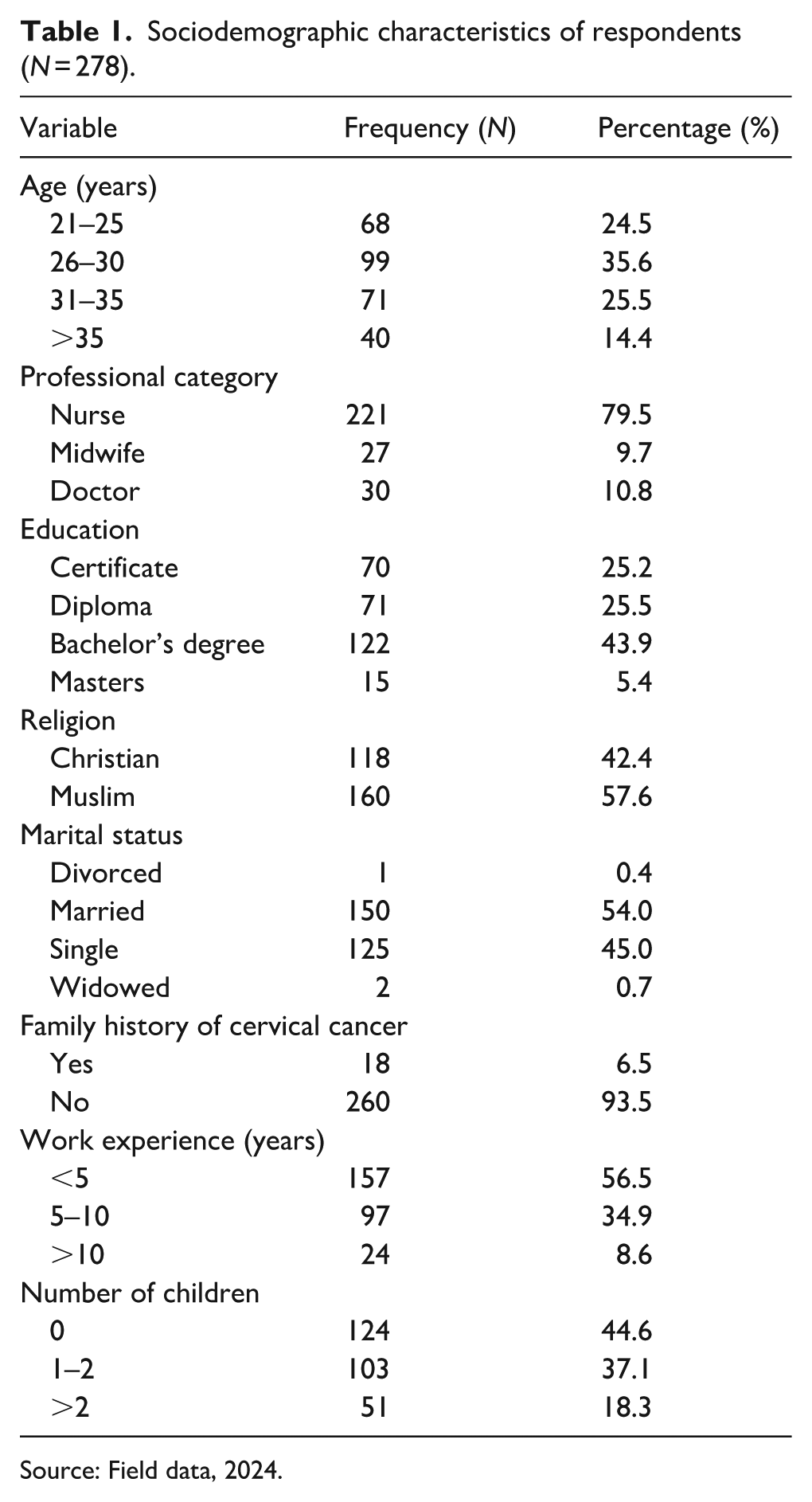
Source: Field data, 2024.
Knowledge of cervical cancer and its screening methods
As shown in Table 2, the mean knowledge score for cervical cancer and its screening methods was 11.30 ± 3.93. Overall, 58.6% of respondents demonstrated good knowledge in this domain. Corresponding results in Table 3 indicated that over half of respondents (55.4%) recognized that cervical cancer is preventable through vaccination of young girls, while a large majority (89.9%) believed it is curable when diagnosed early. In addition, 84.5% correctly disagreed with the statement that cervical cancer could not be transmitted from one person to another. Regarding signs and symptoms, the most frequently identified was pain in the genitalia during sexual intercourse (74.8%). In terms of risk factors, half of the respondents (50.0%) identified HPV infection as a cause. For screening methods, the most commonly recognized were cervical biopsy (88.1%), colposcopy (82.7%), and visual inspection with acetic acid (78.4%).
Descriptive results of knowledge of cervical cancer and its screening methods, and different dimensions of attitudes toward cervical cancer and its screening (N = 278).

Source: Field data, 2024.
SD: standard deviation.
Knowledge of cervical cancer and its screening methods among respondents (N = 278).

Source: Field data, 2024.
HPV: human papillomavirus.
Attitude toward cervical cancer and its screening
As shown in Table 2, the overall mean attitude score toward cervical cancer and its screening was 4.08 ± 0.67 on a 5-point Likert scale, indicating a generally positive attitude among the respondents.
Factor 1: emotional response and perception
As shown in Table 2, this factor recorded a mean score of 3.62 ± 0.89, indicating notable concern about cervical cancer among respondents. Corresponding results in Table 4 revealed that nearly three-quarters (73.4%) agreed or strongly agreed that the thought of cervical cancer scares them, and the same proportion (73.4%) reported being afraid of receiving a bad diagnosis. However, perceptions of personal susceptibility were comparatively lower, with only 41.7% believing they were at risk of developing cervical cancer.
Attitude toward cervical cancer and its screening among respondents.

Source: Field data, 2024.
Factor 2: willingness to encourage others to participate in screening
As presented in Table 2, this factor achieved the highest mean score (4.53 ± 0.73), reflecting strong advocacy and support for cervical cancer screening. Findings in Table 4 showed that an overwhelming majority (92.8%) believed cervical cancer screening is important, 91.8% expressed willingness to encourage colleagues, including nurses, midwives, and medical doctors, to undergo screening, and 89.3% indicated personal interest in participating in cervical cancer screening.
Barriers to cervical cancer screening utilization
As illustrated in Figure 1, the utilization of cervical cancer screening among respondents was low (33.1%). The study further identified several barriers to screening uptake. The most frequently reported barriers were having no reason to undergo screening (72.8%), tight schedules (71.1%), financial constraints (69.5%), and fear of screening outcomes (66.3%). The least reported barriers included lack of knowledge about screening (16.5%), discomfort with the screening process (15.7%), lack of screening facilities (14.1%), lack of interest (12.4%), and the perception of not being at risk (11.6%).

Barriers to cervical cancer screening uptake among respondents.
Factors associated with knowledge of cervical cancer
As shown in Table 5, the analysis showed that knowledge of cervical cancer was significantly associated with professional category and education level. Among professional categories, doctors (70.0%) and nurses (60.2%) had the highest proportion of good knowledge compared to midwives (37.0%; χ² = 6.483, p = 0.039). Regarding education, respondents with a Bachelor’s degree (68.9%) and Diploma (63.4%) had higher proportions of good knowledge than those with a Certificate (38.6%) or Master’s degree (46.7%) (Z = 3.083, p = 0.002). Other sociodemographic variables, including age, religion, marital status, family history of cervical cancer, work experience, and number of children, were not significantly associated with knowledge (p > 0.05).
Association between knowledge of cervical cancer and sociodemographic factors among respondents.

Source: Field data, 2024.
Statistically significant at p < 0.05.
Categories of marital status were recoded.
Cochran-Armitage test for trend.
Chi-square test of association.
χ2 = chi-square statistics.
Z = Z-value.
Attitude toward cervical cancer and its screening by sociodemographic characteristics
Factor 1: emotional response and perception
As shown in Table 6, an independent samples t-test revealed a significant difference in emotional response and perception between respondents with a family history of cervical cancer and those without (p = 0.027). Respondents with a family history of cervical cancer had a higher emotional response and perception mean score (4.07 ± 0.65) compared to those without a family history (3.59 ± 0.90). However, no significant associations were observed between emotional response and perception and other sociodemographic factors, including age, professional category, education, religion, marital status, work experience, or number of children (p > 0.05).
Association between attitude toward cervical cancer and its screening, and sociodemographic factors among respondents.

Source: Field data, 2024.
SD: standard deviation.
Statistically significant at p < 0.05.
Factor 2: willingness to encourage others to participate in screening
As presented in Table 6, no significant associations were found between willingness to encourage others to participate in cervical cancer screening and any of the sociodemographic factors, including age, professional category, education, religion, marital status, family history of cervical cancer, work experience, or number of children (p > 0.05).
Discussion
The purpose of this research was to assess the knowledge, attitudes, and barriers to cervical cancer screening utilization among female healthcare professionals at TTH. The study revealed that more than half of the respondents indicated that cervical cancer cannot be transmitted from one person to another. This finding suggests that the majority of respondents have a correct understanding that cervical cancer itself is not contagious, while the underlying cause, HPV, is the transmissible agent. Recognizing this distinction is important, as it reflects awareness of the disease’s etiology rather than a misconception. This is consistent with a study in the Upper East Region of Ghana, which similarly found that a significant proportion of respondents indicated that cervical cancer is not transmissible. 29 In contrast, studies conducted in Rajasthan and Karad, India, respectively, reported that most respondents believed cervical cancer can be transmitted through multiple sexual partners and sexual contact.39,40 These variations across settings may be due to differences in the emphasis placed on HPV-specific education, the clarity of health messages, and cultural interpretations of sexually transmitted infections.
The study demonstrated that more than half of the respondents had good knowledge of cervical cancer and its screening methods. This is congruent with the results of studies in the Sidama Zone, Southern Ethiopia, the South Gondar Zone, North-Central Ethiopia, and in India, where the majority of respondents had a good level of knowledge of cervical cancer screening.41–43 However, this contrasts with studies in Northern Malawi, the East Gojjam Zone, Northwest Ethiopia, and King Fahad Medical City, Saudi Arabia, where a higher proportion of respondents exhibited poor knowledge about cervical cancer screening.15,44,45 These inconsistencies may be attributed to differences in the quality of health education or access to information among these healthcare professionals.
Despite the relatively high level of knowledge, the study identified that actual screening rates among respondents were low, at only 33.1%. This is a concerning finding, as it suggests that knowledge alone is not sufficient to motivate action. Interestingly, almost all respondents expressed a willingness to encourage their colleagues, including nurses, midwives, and medical doctors, to undergo screening. These findings are consistent with studies in Uttarakhand, India, Hossana Town, Southern Ethiopia, Harar Town, Eastern Ethiopia, and Northern Malawi, where less than half of the respondents had ever undergone screening.4,15,46,47 The study recommends that healthcare institutions implement workplace-based screening programs, making it easier for healthcare professionals to access screening services during their working hours.
The study also identified several barriers to cervical cancer screening uptake. The most common barrier was the lack of a specific reason to undergo screening, which is in agreement with the findings in Abakaliki, Southeastern Nigeria, where lack of a reason was the primary barrier. 48 Moreover, tight schedules and financial constraints were significant barriers, consistent with the findings in Cuenca, Ecuador, and the Upper East Region of Ghana.29,49 To address these barriers, the government should consider offering flexible screening schedules and providing on-site screening facilities to reduce the time and financial burden on healthcare professionals.
Furthermore, fear of screening outcomes was another significant barrier to cervical cancer screening uptake among the respondents. This is consistent with studies in the Upper East Region of Ghana, Nigeria, and Northern Malawi, which reported that fear of the outcome served as a significant barrier to cervical cancer screening uptake among their respondents.15,29,50 This fear may stem from anxiety about potential diagnoses or a lack of understanding about the benefits of early detection. To mitigate this fear, it is essential to provide counseling and support services alongside screening programs, helping individuals understand the importance of early detection and the available treatment options.
The study found that education level and professional category were significantly associated with cervical cancer knowledge among respondents. This is comparable to the study results in Nagyatád, Hungary. 51 In addition, work experience was significantly associated with knowledge of cervical cancer and aligns with the findings in Eswatini, Southern Africa. 52 These findings suggest that more experienced and highly educated healthcare professionals are better informed about cervical cancer. Continuous professional development programs on cervical cancer are needed to provide female healthcare workers, irrespective of their experience or educational level, with equal access to accurate and up-to-date information about cervical cancer.
Limitations of the study
Although this study provides valuable insights into the knowledge, attitudes, and barriers to cervical cancer screening utilization among female healthcare professionals at TTH, it is not without limitations. One significant limitation is the cross-sectional design of the study, which restricts its ability to establish cause-and-effect relationships between the independent and dependent variables. This design also limits the exploration of hidden or confounding variables that may influence the attitudes and behaviors of the respondents. Another limitation is the reliance on self-reported data, which introduces the risk of response bias. Respondents may have overestimated their knowledge, attitudes, barriers, or screening behaviors due to social desirability or recall bias. In addition, the study’s focus on a single healthcare facility in a specific region may limit the generalizability of the findings. The results may not apply to other geographic areas or healthcare settings, even within the same region, due to differences in resources, cultural and religious norms, or healthcare policies.
Practical implications
The low screening rates among female healthcare professionals underscore the urgent need for healthcare institutions to take proactive measures to enhance the utilization of cervical cancer screening among their staff. Implementing workplace-based screening programs can provide convenient access to services, minimizing time constraints for busy professionals. Moreover, education and counseling initiatives can help dispel fears and misconceptions, empowering individuals to prioritize their health. Addressing financial and logistical barriers, such as subsidizing screening costs and offering flexible scheduling, can further improve accessibility and encourage higher participation rates among female healthcare professionals.
Conclusion
The study revealed that more than half of female healthcare professionals demonstrated good knowledge of cervical cancer and its screening methods. A positive attitude toward screening was also evident, as the majority recognized its importance and expressed willingness to encourage their colleagues to participate. Despite this awareness and positive attitude, actual screening rates remained low, highlighting a critical gap between knowledge, attitude, and practice. The study identified key barriers to screening utilization, such as the absence of specific reasons for screening, demanding work schedules, financial constraints, and fear of screening outcomes. In addition, significant associations were found between cervical cancer knowledge and sociodemographic factors such as education level, professional category, and work experience. Higher knowledge levels were observed among respondents with a Bachelor’s degree, those with less than 5 years of work experience, and those working as nurses.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251401319 – Supplemental material for Knowledge, attitudes, and barriers to cervical cancer screening utilization among female healthcare professionals in the Tamale Metropolis
Supplemental material, sj-docx-1-whe-10.1177_17455057251401319 for Knowledge, attitudes, and barriers to cervical cancer screening utilization among female healthcare professionals in the Tamale Metropolis by Abdul-Malik Abdulai, Iddrisu Mohammed Sisala, Ibrahim Issah, Catherine Kyiu, Yakubu Fatimata, Mudasir Mohammed Ibrahim and Abubakari Wuni in Women's Health
Footnotes
Acknowledgements
We thank all the respondents for spending their time and participating in the study.
Ethical Considerations
This study was approved by the Committee on Human Research, Publications, and Ethics at Kwame Nkrumah University of Science and Technology (approval number: CHRPE/AP/1001/24) and the Research and Development Unit of Tamale Teaching Hospital (approval number: TTH/R&D/SR/24/059).
Consent to participate
Written informed consent was obtained from all respondents prior to their involvement in the study.
Consent for publication
All respondents in this study provided both written and verbal informed consent to have their results reported anonymously.
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the conclusions of this study are available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.