
Abstract
Background:
Cervical cancer remains one of the most preventable yet deadly diseases affecting women in low-resource and conflict-affected regions such as Syria. Persistent challenges including limited access to health care, disrupted health infrastructure, sociocultural taboos, and inadequate health education have severely restricted the implementation and uptake of screening programs. Understanding the multifaceted determinants of women’s awareness, perceptions, and health-seeking behavior is essential for designing sustainable, context-sensitive prevention strategies.
Objectives:
This study aimed to evaluate Syrian women’s knowledge, attitudes, and screening practices toward cervical cancer and to identify demographic, educational, and psychosocial predictors influencing these domains. It also sought to explore the paradoxical role of education in shaping self-efficacy, awareness, and screening-related attitudes within this population.
Design:
A descriptive cross-sectional design was employed.
Methods:
Data were collected between November 2024 and May 2025 in Damascus, Syria, using a validated self-administered electronic questionnaire. A total of 606 women aged 15 years and above participated voluntarily. The questionnaire assessed knowledge, attitudes, and self-efficacy related to cervical cancer and screening behaviors. Descriptive statistics and linear regression analyses were performed to examine associations between sociodemographic factors and outcome measures.
Results:
Although 49% of respondents demonstrated moderate knowledge, only 10% had ever undergone a Pap smear. Major barriers included embarrassment (59%), fear of discomfort (51%), and financial limitations (21%). Higher education significantly predicted better knowledge (p < 0.05) but was paradoxically linked to less favorable attitudes and lower self-efficacy. Greater knowledge correlated positively with self-efficacy, while older age showed a negative association.
Conclusion:
A profound disconnect persists between awareness and screening behavior among Syrian women. Interventions must extend beyond information delivery to address cultural, emotional, and economic barriers through comprehensive, community-based, and empowerment-oriented public health initiatives.
Introduction
Cervical cancer represents a significant global health challenge, ranking as the fourth most prevalent malignancy among women and a leading cause of cancer-related mortality, particularly in low- and middle-income countries. 1 This burden is a public health paradox, as the disease is largely preventable. The primary etiology is well-established—persistent infection with high-risk human papillomavirus (HPV)—and effective primary (HPV vaccination) and secondary (routine screening) prevention strategies exist. 2 Other well-documented risk factors include early sexual debut, multiple sexual partners, high parity, long-term hormonal contraceptive use, and tobacco smoking.3,4
The success of preventive efforts, however, is contingent upon robust healthcare systems and high levels of public awareness, conditions that are severely compromised in conflict-affected regions.
In Syria, cervical cancer constitutes a meaningful share of women’s cancer morbidity; however, incidence and mortality are likely underestimated because population-based cancer registration is absent and conflict has disrupted health information and reporting systems. According to GLOBOCAN 2022 estimates, the age-standardized incidence rate (ASR, World) of cervical cancer in Syria is 2.5 per 100,000 women, and the ASR mortality rate is 1.3 per 100,000 women, underscoring the need for robust locally generated epidemiological data to guide prevention and screening.5–7 Syrian women, in particular, represent a population facing compounded vulnerabilities due to over a decade of armed conflict, mass displacement, and the systemic disruption of national health infrastructure. 8 This protracted crisis has severely eroded access to essential services, including routine preventive care like cervical cancer screening, magnifying the health risks for millions. 9
Adding a critical layer of complexity is the global syndemic of obesity (body mass index (BMI) ⩾30 kg/m2), an independent risk factor for numerous noncommunicable diseases, including at least 13 types of cancer. 10 For women, obesity not only contributes to physiological changes that can elevate cancer risk but also introduces profound barriers to health care. These can include social stigma, limited mobility, equipment inaccessibility in clinical settings, and potential provider bias, all of which can deter engagement in preventive health behaviors. 11 The intersection of displacement-related trauma and obesity-related health disparities creates a unique and unstudied vortex of vulnerability for Syrian women. 12
To date, a critical gap exists in literature, as no studies have specifically investigated cervical cancer awareness, screening practices, and barriers at the nexus of these overlapping vulnerabilities. Therefore, this descriptive cross-sectional study aimed to assess the level of knowledge regarding cervical cancer risk factors, prevention, and screening among Syrian women with obesity. A primary objective was to identify the perceived socioeconomic, cultural, and health care–system barriers they face in accessing screening services. The findings from this research are intended to provide crucial, evidence-based insights to inform the development of targeted, culturally sensitive interventions and ultimately promote health equity for this critically underserved population.
Methods
Study design
This descriptive cross-sectional study was conducted between November 2024 and April 2025, to assess knowledge, attitudes, and practices regarding cervical cancer and Pap smear screening among Syrian women visiting hospitals in Damascus. The data were collected by the authors as interviews with patient using a self-administered electronic questionnaire distributed via Google Forms. Participants were randomly approached in hospital waiting areas and recruited after providing informed consent. The survey was conducted through 3 month period starting December 2024 ending in February 2025.
Participants and data collection
The researchers distributed the electronic questionnaire to patients and their companions who were attending governmental hospitals and medical centers. Participants accessed the self-administered questionnaire via a secure Google Forms link, which was provided directly by the research team using mobile devices or tablets at the study sites. For illiterate participants, trained research assistants read the questions aloud and recorded responses confidentially, ensuring independent and unbiased data entry. Incomplete data were excluded from the study. Six hundred six individuals aged 15 and older were randomly selected to participate in the study. To ensure participants’ understanding and interaction, the study’s objectives and importance were explained in advance, highlighting its role in raising awareness about cervical cancer. Each participant was allowed to complete the questionnaire only once to maintain data integrity and prevent duplicate answers. In addition, participants were encouraged to answer truthfully, with assurance of their anonymity and confidentiality at the beginning of the questionnaire. Participants were also informed that participation was voluntary and therefore would receive no compensation for their participation. The participating women were included regardless of their ages and whether they were married or unmarried. Exclusion criteria included incomplete responses, refusal to participate, and cognitive or psychological impairments. This study was conducted in accordance with the principles of the Declaration of Helsinki. This study was conducted in accordance with the STROBE checklist. 13
Response rate
A total of 606 women accessed the questionnaire, of whom 561 completed it in full and were included in the analysis, resulting in a response rate of approximately 93%. The remaining 45 participants (7%) were excluded because of incomplete responses or failure to meet inclusion criteria. While the calculated minimum sample size was 196, a larger sample was ultimately recruited and analyzed to enhance statistical power and generalizability. All analyses reported in this study are based on the final dataset of 561 completed questionnaires.
Questionnaire translation and validation
The questionnaire included validated scales, multiple-choice questions, and open-ended questions covering demographic information, knowledge, attitude, practices, and self-efficacy. The full Arabic and English versions of the questionnaire have been submitted as Supplemental Material with this manuscript. The questionnaire was distributed in Arabic to ensure it reached the target group. The original English version was translated into Arabic using a forward–backward translation reviewed by language experts to ensure accuracy and cultural relevance. It was then translated back into English. A pilot study involving 50 visitors confirmed clarity and content validity. The questionnaire was reviewed based on initial statistical study, and its reliability was assessed using Cronbach’s alpha test, which demonstrated high internal stability (0.869).
Measures
This study utilized a structured and validated questionnaire that has been previously published by Ghalavandi et al. 14 to assess women’s knowledge, attitudes, and self-efficacy regarding Pap smear screening. The focus of the questionnaire was exclusively on Pap smear (Papanicolaou test) as the primary cervical cancer screening modality, reflecting current national practice and availability in Syria. Other cervical cancer screening methods, such as HPV DNA testing or visual inspection with acetic acid, were not assessed, as they are not routinely available or widely implemented in the Syrian healthcare setting. The questionnaire comprises four main sections. The first section consists of demographic questions (including age at first sexual intercourse, and previous history of Pap smear testing). The second section assesses knowledge through 13 questions with 3-item responses (correct, incorrect, don’t know) such that correct answers received a score of 1, incorrect and don’t know a score of 0. The third section examines attitudes toward Pap smear screening using 12 items rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), focusing on psychological barriers (such as embarrassment or fear of pain) and financial concerns. The final section evaluates self-efficacy through eight items, also rated on a 5-point Likert scale, measuring the participant’s confidence in performing health-seeking behaviors such as initiating discussions with healthcare providers, scheduling the test, and attending follow-up appointments. The self-efficacy domain of this questionnaire is based on the questionnaire used by Fernández et al. 15 among Mexican-American women.
Statistical analysis
The data collected through electronic questionnaire on Google Form were exported to Excel for analysis. Statistical analysis was carried out using the SPSS Inc. version 23 software package. Chi-square and one-way ANOVA were used to identify any correlation between demographic variables and level of knowledge related to cervical cancer information. A p-value of less than 0.05 was considered statistically significant.
Sample size
In order to calculate the necessary sample size (n), Cochran’s sample size formula was utilized by the research team. The formula took into consideration a 95% confidence level, represented by Z = 1.96, a margin of error of 7%, represented by e, and an estimated proportion (p) of 50% or 0.5 for the attribute of interest within the population. Additionally, q was determined as 1 − p:

By using the formula, the necessary sample size for this study was determined to be 196.
Results
The participants had an average age of 39.55 ± 12.37 years and a mean BMI of 26.91 ± 5.61. The majority resided in rural areas (55%) and identified as chaperones (66%). Most experienced their first menses between 13 and 14 years (48%) and had their first sexual intercourse at an average age of 16.56 ± 8.37 years. A significant proportion were married (76%), held a secondary education (43%), and reported a good financial status (66%). Additionally, a large percentage were unemployed (68%), while 29% were smokers (Table 1).
Baseline characteristics of the subjects under study.

BMI: body mass index; SD: standard deviation.
Nearly half (49%) of participants were aware of cervical cancer, mainly from the internet (19%) and family/friends (11%), yet only 10% had undergone a Pap smear. While 75% supported annual screenings, misconceptions persisted, with 51% finding exams uncomfortable and 59% feeling embarrassed. Key concerns included cost (21%) and effectiveness (20%). Knowledge and attitude scores averaged 5.14 ± 2.36 and 35.25 ± 3.82, respectively. Most participants felt confident discussing Pap tests with providers (83%) and scheduling (74%), but concerns about pain, cost, and discouragement affected 18–25%. The self-efficacy score averaged 30.13 ± 5.86 (Tables 2–4).
Knowledge about Pap smear.

SD: standard deviation.
Attitude toward Pap smear.
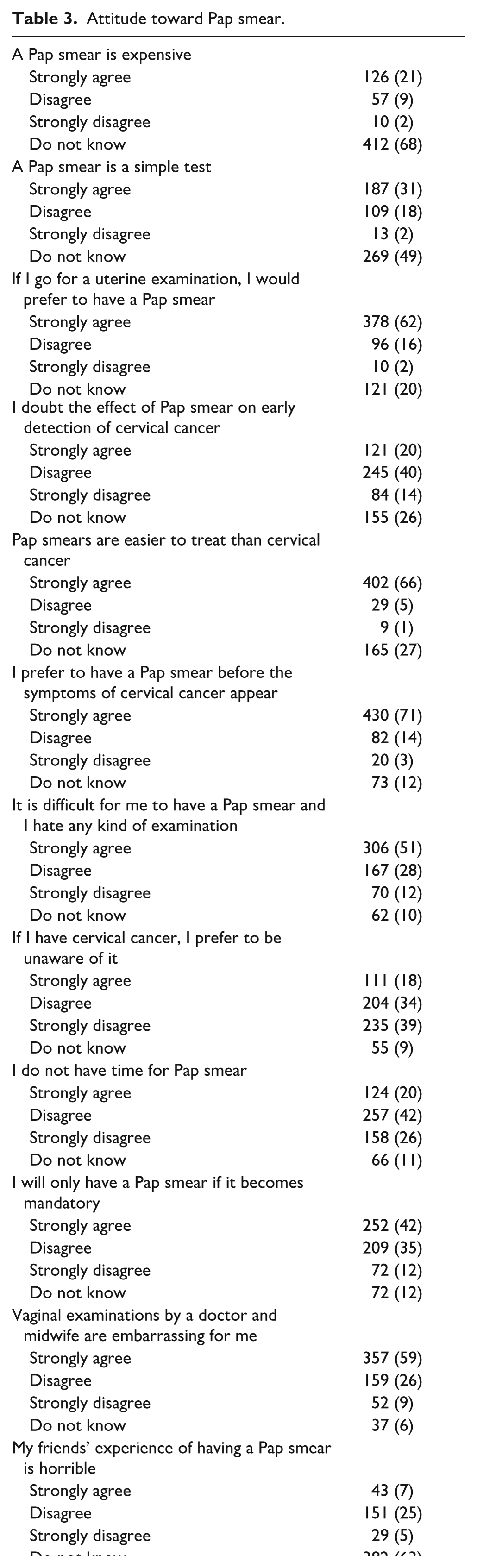
SD: standard deviation.
Self-efficacy regarding the Pap smear test.
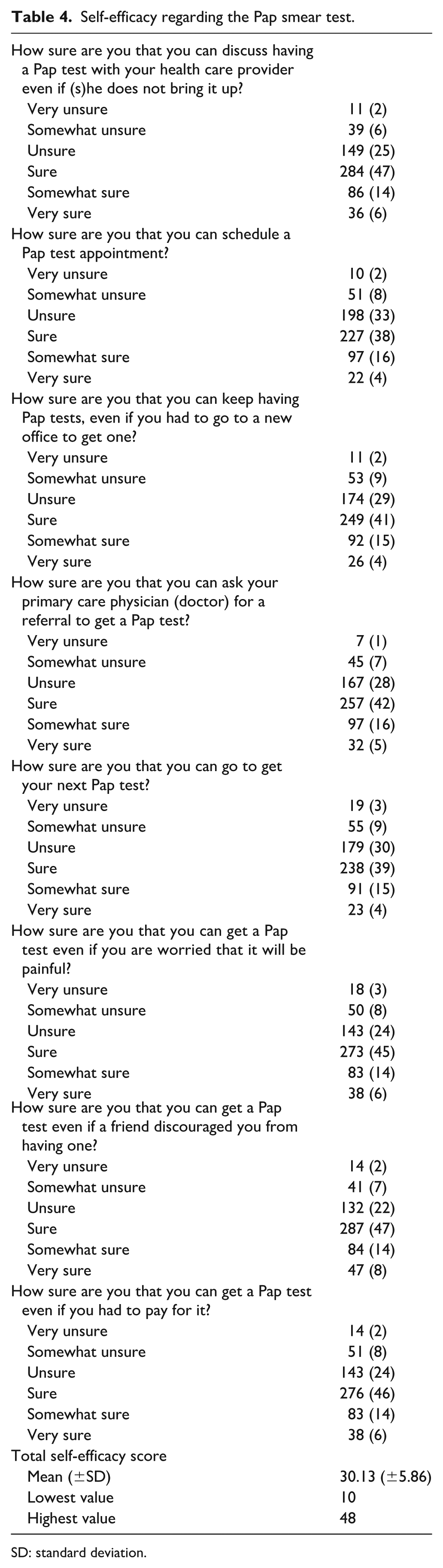
SD: standard deviation.
Simple and multiple linear regression analyses identified higher education and prior cervical cancer knowledge as key predictors of better knowledge scores. University education was linked to higher scores in both the simple (B = 0.35, 95% confidence interval (CI): 0.13 to 0.56, p = 0.0015) and multiple models (B = 0.27, 95% CI: 0.02 to 0.52, p = 0.0296*). Similarly, prior knowledge significantly improved scores in the simple (B = 0.33, 95% CI: 0.14 to 0.51, p = 0.0005) and multiple models (B = 0.27, 95% CI: 0.08 to 0.47, p = 0.0056; Table 5).
Association between baseline characteristics and knowledge score regarding the Pap smear test.

BMI: body mass index; CI: confidence interval.
represents statistical significance at p < 0.05.
Both simple and multiple linear regression analyses identified education level as the sole significant predictor of attitude scores, with higher education linked to lower scores (B = −0.65, 95% CI: −1.00 to −0.30, p = 0.0003) and (B = −0.65, 95% CI: −1.06 to −0.24, p = 0.0019; Table 6).
Association between baseline characteristics and attitude scores regarding the Pap smear test.

BMI: body mass index; CI: confidence interval.
represents statistical significance at p < 0.05.
Linear regression analyses identified knowledge, attitude, age, and education level as significant predictors of self-efficacy. Higher knowledge scores were strongly linked to increased self-efficacy (crude: B = 0.82, p < 0.0001; adjusted: B = 4.83, p < 0.0001), whereas a more positive attitude was associated with lower self-efficacy (crude: B = −0.32, p < 0.0001; adjusted: B = −3.41, p < 0.0001). Additionally, age negatively influenced self-efficacy (crude: B = −0.04, p = 0.0121; adjusted: B = −1.42, p = 0.0439), and higher education was linked to lower self-efficacy in the adjusted model (B = −1.04, p = 0.0005; Table 7).
Association between baseline characteristics and self-efficacy score regarding the Pap smear test.

BMI: body mass index; CI: confidence interval.
represents statistical significance at p < 0.05.
Discussion
This study explored awareness of cervical cancer among Syrian women, analyzing the influence of key demographic, socioeconomic, and behavioral factors. Our findings reveal significant knowledge gaps and highlight multifaceted barriers to prevention and early detection, underscoring the urgent need for targeted intervention strategies.
Age and health experience
A key finding was the positive correlation between age and awareness, with a mean participant age of 39.55 ± 12.37 years and a 49% awareness rate. This suggests that accumulated life experience and greater exposure to health information contribute to enhanced knowledge. This aligns with prior research reporting a 42.2% awareness rate in a similar demographic, where older age was associated with more educational and health-related opportunities.16,17 However, awareness rates vary significantly across studies, with some reporting rates as high as 89.5% for women over 30, 18 illustrating that context-specific health campaigns and cultural factors are powerful moderators of knowledge.
Socioeconomic and geographic determinants
Socioeconomic and geographic factors emerged as powerful determinants of awareness. A majority of participants resided in rural areas (55%), where awareness was notably lower than in urban settings. While secondary education was most common (43%), a high unemployment rate (68%) likely acts as a significant barrier to accessing health care, despite a majority (66%) describing their financial status as stable. Furthermore, the fact that most participants (66%) were accompanying other patients rather than seeking care for themselves suggests that their presence in a hospital did not necessarily correlate with a personal interest in preventive health. These findings are consistent with extensive research demonstrating that rural populations exhibit lower awareness and that higher educational attainment correlates with increased knowledge of cervical cancer.19–21 This pattern is echoed globally, with studies in Kenya and India confirming that older age, higher education, and socioeconomic status are strong predictors of both awareness and screening uptake.22,23
Psychosocial barriers to screening
A significant paradox emerged between participants’ stated willingness to engage in screening and the powerful psychosocial barriers they face. While a majority expressed confidence in discussing Pap smears (83%) and willingness to schedule an appointment (74%), significant percentages also reported that the procedure was uncomfortable (51%), embarrassing (59%), or ineffective (23%). These findings resonate strongly with a systematic review on barriers in low- and middle-income countries, which identified emotional challenges—such as shame, fear, and discomfort—along with lack of family support and financial obstacles as primary deterrents. Critically, mistrust in the healthcare system and doubts about its efficacy were also cited as key reasons for avoiding preventive care.24–26
Information-seeking behaviors and social influence
Information-seeking behaviors were dominated by modern and informal channels. The internet was the primary source of information (19%), followed by friends and family (11%), highlighting the influential roles of digital platforms and peer networks. This reliance is supported by some studies,16,22 yet it contrasts with other contexts where traditional media like television and radio remain more influential. 27
Biological risk factors and social norms
Our findings on biological and life-course factors highlight the influence of social norms on health risks. The average age of first sexual activity being under 18 reflects the prevalence of early marriage, a practice widely recognized as a risk factor for cervical cancer.28,29 Furthermore, key biological markers reported by participants, such as age at menarche (48% between 13 and 14) and marital status (76% married), are consistent with established risk profiles. 30 The crucial role of social support is further emphasized by literature, indicating that a husband’s encouragement can be a decisive facilitator for women seeking preventive care.31–33
Health consciousness and lifestyle factors
Finally, health-related behaviors such as smoking were prevalent in a notable percentage of participants. Beyond being a direct physiological risk factor, smoking often correlates with a general neglect of preventive health behaviors. Similarly, the role of obesity, as measured by BMI, was examined in our analysis. While a high proportion of participants were overweight or obese (mean BMI 26.91 ± 5.61), BMI was not found to be a significant predictor of knowledge, attitude, or self-efficacy regarding Pap smear screening in our regression models (see Tables 5–7). This finding is consistent with some reports indicating that, in resource-limited settings, cultural and economic barriers may have a greater impact on preventive behaviors than individual biomedical risk factors such as obesity. This observation is corroborated by research from China, which confirmed that smokers tend to be less health-conscious than nonsmokers, impacting their engagement with preventive medicine.34,35 Similarly, despite a high prevalence of being overweight (mean BMI 26.91 ± 5.61), screening uptake remained low (10%). This diverges from studies suggesting a positive link between being overweight and engaging in preventive screenings, 36 indicating that in this context, formidable cultural and economic barriers may override the health-consciousness associated with a recognized risk factor.
Limitations
The conclusions of this study should be considered with an awareness of its methodological constraints. The generalizability of our findings is limited by the use of a non-probability sample, which may not accurately reflect the experiences of Syrian women living in remote areas or seeking care outside of public hospitals. Furthermore, our analysis did not capture the full complexity of sociocultural influences, as regional variations in education and culture were not examined in detail. Additionally, as the data were self-reported, there is a potential for social desirability bias, particularly concerning sensitive topics such as embarrassment, fear, or attitudes toward screening. This may have led to underreporting or overreporting of certain behaviors, and thus, the findings should be interpreted with this limitation in mind. Deeper factors, including religious convictions and personal histories with the healthcare system, also remained outside of the scope of this research and would be more effectively explored using qualitative approaches. Additionally, the cross-sectional design precludes establishing causality or assessing changes in knowledge, attitudes, and behaviors over time, even though a sizable and diverse sample was analyzed. It is also crucial to note that the cross-sectional design allows us to identify associations but does not support an inference of causality between the studied variables. We acknowledge that a more detailed description of the methodological flow—particularly regarding recruitment and data collection in the context of ongoing conflict—would enhance understanding of behavioral shifts and barriers unique to conflict-affected populations.
Conclusion
This study demonstrates that women’s awareness of cervical cancer is shaped by a complex interplay of demographic, social, and psychological factors. Crucially, our findings indicate that insufficient knowledge about the disease and its prevention is not merely an informational deficit but is compounded by significant cultural and behavioral barriers that deter proactive screening.
These findings underscore the urgent necessity for comprehensive health interventions that are both evidence-based and tailored to the specific needs of local communities. Improving awareness must therefore be framed not as a simple educational goal, but as a core component of a national preventive strategy designed to reduce morbidity and mortality from cervical cancer. To achieve this, we recommend the implementation of community-based awareness programs, the expansion of access to screening, and the development of culturally sensitive health policies to ensure the long-term success of these vital efforts. Future research should incorporate longitudinal and qualitative approaches to identify specific, culturally tailored strategies, address persistent barriers, and capture the nuanced perspectives of women and healthcare providers in diverse sociocultural settings. Such studies will be critical to designing effective interventions and promoting sustained behavioral change.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261443140 – Supplemental material for Knowledge, attitudes, and practices regarding cervical cancer screening among women in Damascus, Syria: A cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057261443140 for Knowledge, attitudes, and practices regarding cervical cancer screening among women in Damascus, Syria: A cross-sectional study by Jamal Ataya, Batoul Alotaki, Kais Alhammadi, Toka Al Homsi, Waed abboud, Hamsa Sahlieh, Sahar Alzhouri, Ahmad Al-Bitar, Maram Alshikh Hamo, Dimah Kakat, Bayan Alhaj, Lutfallah Raffoul and Saeed Kadri in Women's Health
Footnotes
Acknowledgements
None.
Ethical Considerations
Ethics approval for the study was obtained from the Ethical Committee of Homs University, Faculty of Medicine, Syria (4245). Written informed consent was obtained from all participants prior to their inclusion in the study.
Consent to participate
For participants under 18 years of age, parental or guardian consent was secured. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent for publication
Written informed consent for publication of their clinical details and/or clinical images was obtained from all participants. A copy of the written consent is available for review by the editor-in-chief of this journal on request.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed during this study are included in this published article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.